Masterclass in Thumb and Finger Reconstruction: Toe-to-Hand Transfer
Key Takeaway
Single-stage toe-to-hand transfer is a pinnacle microsurgical procedure for thumb and digit reconstruction. By utilizing the great, second, or third toes, surgeons can restore critical pinch, grip, and opposition. This comprehensive guide details the preoperative vascular mapping, dual-team surgical dissection, precise microvascular anastomoses, and rigorous postoperative rehabilitation protocols required to achieve optimal functional and aesthetic outcomes in complex hand trauma reconstruction.
INTRODUCTION TO THUMB AND FINGER RECONSTRUCTION
The thumb is the biomechanical cornerstone of the human hand, responsible for approximately 40% to 50% of overall hand function. Its unique capacity for opposition, combined with robust pinch and grip strength, makes its loss a devastating functional impairment. The evolution of thumb reconstruction represents one of the most profound advancements in modern orthopedic microsurgery.
In 1900, Nicoladoni first reported his experiences with a staged pedicle transfer of the toe for thumb reconstruction. However, the necessity for prolonged, awkward immobilization of the arm and leg, coupled with the resulting stiffness and insensitivity of the reconstructed digit, prevented widespread adoption. The paradigm shifted dramatically in 1966 when Buncke et al. reported the first successful single-stage transfer of a toe to the hand in primates using microvascular anastomoses. Shortly thereafter, in 1967, Cobbett performed the first single-stage toe-to-hand transfer in a human. Remarkably, at a 30-year follow-up, Cobbett’s patient remained gainfully employed as a manual laborer, underscoring the long-term durability and functional success of this microsurgical marvel.
Today, single-stage free tissue transfer of the great toe, second toe, or combined second and third toes remains the gold standard for restoring prehension, sensation, and aesthetic appearance in the mutilated hand.
PREOPERATIVE EVALUATION AND PLANNING
Meticulous preoperative planning is the absolute determinant of success in toe-to-hand transfers. The surgeon must evaluate both the recipient hand's requirements and the donor foot's vascular anatomy.
Vascular Assessment
The vascular anatomy of the foot is highly variable. The dominant arterial supply to the great and second toes may arise from the dorsal system (dorsalis pedis artery and first dorsal metatarsal artery [FDMA]) or the plantar system (posterior tibial artery and plantar metatarsal arteries).
* Clinical Examination: Palpation of pulses and handheld Doppler mapping are mandatory.
* Angiography: High-resolution, two-plane angiography or MR angiography (MRA) is strongly recommended to document the adequacy of the posterior tibial arterial supply and to delineate the course of the FDMA. This ensures that harvesting the dorsal system will not compromise the viability of the remaining foot.
Donor Selection and Templating
While the ipsilateral great toe is most commonly utilized, the contralateral great toe should be considered if the medial skin of the foot is required for soft-tissue coverage on the reconstructed thumb.
Clinical Pearl: Buncke advocated for the use of clay or plaster models (created from alginate impressions of the patient’s toes) placed in the thumb position. This three-dimensional templating is invaluable for determining toe selection, osteotomy angles, and the precise amount of skin required for tension-free closure.
Soft-Tissue Optimization
The recipient area must have adequate, well-vascularized soft tissue. If the recipient bed is heavily scarred or deficient, traditional coverage techniques (e.g., pedicled groin flaps, radial forearm flaps) should be performed prior to thumb reconstruction. Alternatively, a dorsal foot flap can be incorporated with the great toe transfer as a chimeric flap. Generally, split-thickness skin grafting is preferred on the recipient hand rather than the donor foot, as grafting on the dorsum of the foot yields unpredictable healing and higher morbidity.
SURGICAL TECHNIQUE: SINGLE-STAGE TRANSFER OF THE GREAT TOE
Preparation and Positioning
- Positioning: Place the patient supine so that both the donor foot and the recipient hand are simultaneously accessible.
- Thermal Regulation: Utilize a padded operating table equipped with a heating and cooling blanket. Core temperature must be strictly monitored via esophageal or rectal probes to prevent hypothermia-induced vasospasm.
- Monitoring: Insert an indwelling urinary catheter to monitor output and ensure adequate intravascular volume.
- Dual-Team Approach: Two synchronized surgical teams are required—one preparing the recipient hand and the other harvesting the donor toe. This minimizes total ischemia time.
- Marking: Using skin-marking pencils, outline the incisions on both the hand and foot, ensuring adequate soft-tissue flaps for tension-free closure.
Foot Dissection (Donor Site)
- Venous Mapping: Before exsanguination, hold the foot in a dependent position over the edge of the table to allow venous engorgement. Outline the large superficial veins on the dorsum of the foot and the tributaries to the greater saphenous system (typically located on the medial side of the first metatarsal).
- Tourniquet Application: Exsanguinate the limb by elevation or elastic wrapping, and inflate the pneumatic tourniquet.
- Dorsal Dissection: Make straight, curved, or zigzag dorsal incisions. Identify and meticulously preserve the dorsal veins, the dorsalis pedis artery, and its distal continuation, the FDMA.
- Arterial Mobilization:
- If the FDMA is dorsal: Proceed from proximal to distal, protecting the artery and ligating/clipping side branches.
- If the dominant artery is plantar: Dissect from the first web space proximally. Extend a longitudinal plantar incision just lateral to the weight-bearing area over the first metatarsal head. Dividing the transverse metatarsal ligament is often necessary to mobilize a plantar metatarsal artery.
- If in doubt: Begin in the first web space and dissect proximally. Ligate the artery to the second toe and mobilize the first metatarsal artery proximally until its dorsal or plantar dominance is confirmed.
- Nerve Harvest:
- Follow the dorsal artery to the extensor hallucis brevis (EHB). Divide and elevate the EHB to expose the deep peroneal nerve lateral to the dorsalis pedis artery. Preserve this nerve for coaptation.
- In the first web space, dissect the plantar digital nerve on the lateral side of the great toe, separating it from the common digital nerve. Similarly, mobilize the medial plantar digital nerve.
- Tendon Harvest:
- Section the extensor hallucis longus (EHL) tendon near the extensor retinaculum.
- Make a transverse incision in the mid-to-proximal plantar surface of the foot to locate the flexor hallucis longus (FHL) tendon. Separate it from its interconnections (Master Knot of Henry) with the flexor digitorum longus to obtain adequate length.
- Osteotomy: Separate the toe at the metatarsophalangeal (MTP) joint. If reconstructing a new metacarpophalangeal joint, harvest the joint capsule. The plantar aspect of the metatarsal head must be preserved to prevent transfer metatarsalgia; however, a dorsal oblique osteotomy of the first metatarsal may be taken with the toe.
Surgical Warning: Do NOT transect the proximal vascular attachments until complete vascularization through the arteriovenous pedicle is ensured, and the hand dissection is fully prepared to receive the transplant.
- Tourniquet Release: Deflate the tourniquet, achieve meticulous hemostasis in the foot, and confirm robust perfusion to the isolated toe before final pedicle division.
Hand Dissection (Recipient Site)
- Incisions: Outline a curved incision on the dorsoradial aspect of the thumb base (near the anatomical snuffbox) and a palmar incision along the thenar crease, extending over the carpal tunnel into the distal forearm.
- Dorsal Preparation: Identify and mobilize the extensor pollicis longus (EPL), extensor pollicis brevis (EPB), and abductor pollicis longus (APL) tendons. Isolate the cephalic vein, the radial artery (and its princeps pollicis branch), and the superficial radial nerve branches.
- Palmar Preparation: Identify the digital nerves to the thumb, the flexor pollicis longus (FPL) tendon, the adductor pollicis, and abductor pollicis brevis tendons. Isolate suitable palmar digital arteries.
- Bone Preparation: Create a hollow recess (cup-and-cone configuration) in the base of the proximal phalanx of the toe, allowing the thumb metacarpal remnant to be remodeled and inset securely.
Microsurgical Transfer and Reconstruction
- Bony Fixation: Transfer the toe to the hand. Achieve rigid bony apposition using longitudinal and crossed Kirschner wires, or intraosseous wiring/mini-plates depending on the bone stock.
- Tendon Repair: Balance the biomechanical forces on the transferred toe.
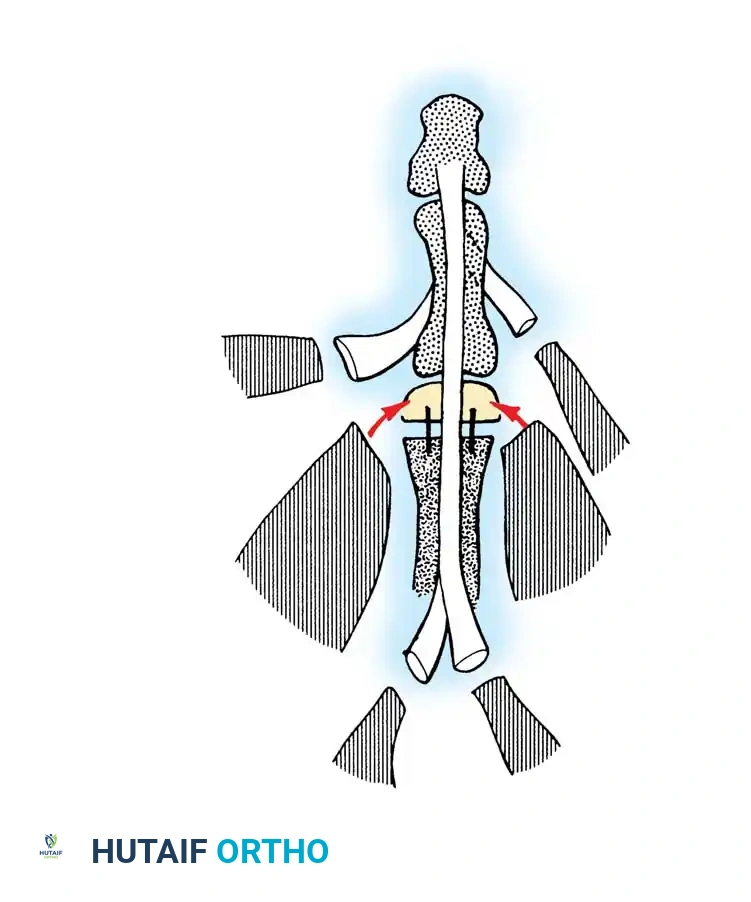
Fig. 60-63 Transfer of great toe to thumb. Scheme suggested by May for reconstruction of available tendon attachments. Abh, abductor hallucis; AbPB, abductor pollicis brevis; ADD, adductor hallucis; EHB, extensor hallucis brevis; EHL, extensor hallucis longus; EPB, extensor pollicis brevis; EPL, extensor pollicis longus; FHL, flexor hallucis longus; FPL, flexor pollicis longus. (From May JW, Bartlett SP: Great toe-to-hand free tissue transfer for thumb reconstruction, Hand Clin 1:271, 1985.)
- Arterial Anastomosis: Ensure pulsatile flow from the recipient radial artery. Perform an end-to-end or end-to-side anastomosis between the dorsalis pedis artery and the radial artery (or first metacarpal artery) using 9-0 or 10-0 nylon under the operating microscope.
- Venous Anastomosis: Anastomose the saphenous venous system of the toe to the cephalic venous system of the hand. Typically, one robust arterial and one to two venous anastomoses are sufficient.
- Neurorrhaphy: Suture the lateral plantar digital nerve of the toe to the ulnar digital nerve of the thumb, and the medial plantar digital nerve to the radial digital nerve. Coapt the superficial radial nerve branches to the deep peroneal nerve.
- Closure: Loosely close the wounds over small, thin rubber drains. Apply split-thickness skin grafts to any residual defects to avoid tension over the vascular pedicle. Apply a bulky, non-constricting plaster splint.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative phase is as critical as the microsurgery itself. The primary goal is the prevention of vasospasm and thrombosis.
- Environment & Positioning: The patient is kept in a warm, quiet room. Both the reconstructed hand and the donor foot are elevated.
- Anticoagulation: Intravenous low-molecular-weight dextran or continuous heparin infusion is typically administered for 3 to 5 days, based on institutional preference and intraoperative flow characteristics.
- Monitoring: Clinical observation (capillary refill, turgor, color, temperature) is paramount. Implantable Doppler probes or surface temperature monitors are highly recommended for the first 72 hours.
- Donor Site Management: To minimize foot morbidity, the patient is kept strictly non-weight bearing on the involved foot for 2 to 4 weeks. An elastic support stocking is used after suture removal to control edema.
- Hand Rehabilitation: Bandage changes are delayed for 5 to 7 days if possible. The thumb is protected in a splint for 3 to 4 weeks. Following clinical and radiographic evidence of bony union, gentle protected active motion is initiated. Aggressive strengthening and dynamic splinting are delayed until 10 to 12 weeks. Strenuous manual labor is restricted until protective sensory return is documented.
SECOND AND THIRD TOE TRANSPLANTATION
While great toe transplantation is exceptional for isolated thumb loss, severe crush injuries or amputations involving the thumb and multiple digits require a more expansive reconstructive strategy. A hand lacking both a thumb and opposing digits is profoundly impaired.
Indications and Leung's Classification
Transplantation of the second toe, or en bloc transfer of the second and third toes, is indicated to restore opposition and broad pinch grip in severely mutilated hands. Leung developed a highly useful classification system for thumb loss to guide the selection of microsurgical reconstructive procedures, often favoring the second toe over the great toe to preserve foot biomechanics.
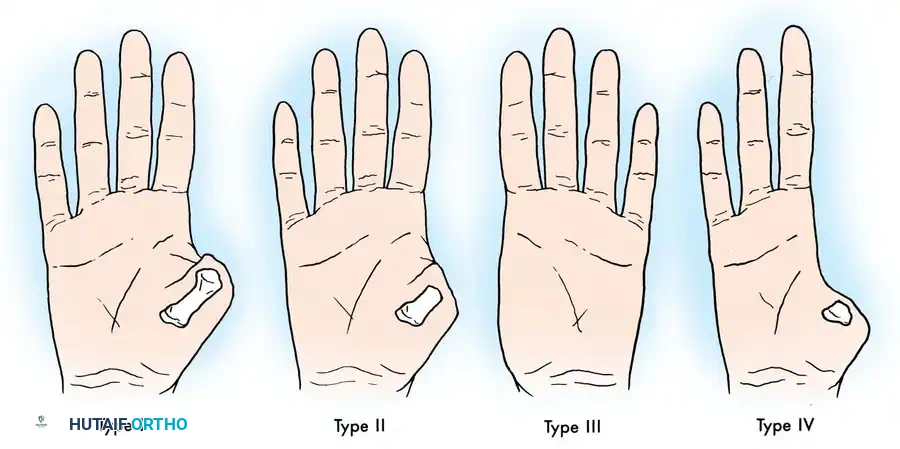
Fig. 60-64 Leung’s classification of thumb loss, useful when considering different types of thumb reconstructive microsurgical procedures. (From Leung PC: Thumb reconstruction using second-toe transfer, Hand Clin 1:285, 1985.)
Double Toe Transplantation
For hands with only one or two remaining digits, double toe transplantation (harvesting the second toe from each foot, or the second and third toes from a single foot) significantly improves function and appearance.
* Simultaneous vs. Sequential: Gordon et al. demonstrated that simultaneous double toe transplantation (utilizing two surgical teams) reduces overall operative time, hospital stay, and cost compared to sequential staged procedures.
* Donor Morbidity: The risk of impaired ambulation is minimized when single toes are harvested from separate feet, rather than removing two adjacent toes and their metatarsal segments from a single foot. Strict adherence to a non-weight bearing protocol postoperatively ensures minimal long-term foot morbidity.
Clinical Outcomes and Functional Restoration
The integration of toe-to-hand transfers yields remarkable functional restoration. The transplanted digits provide a stable, sensate post for opposition.

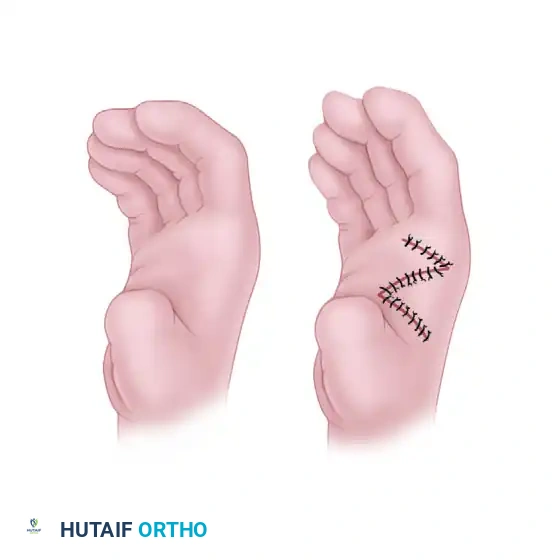
Intraoperative view demonstrating the inset of the toe transfer with a skin graft applied over the dorsal vascular pedicle to ensure a tension-free closure.

Dorsal view of the healed reconstructed hand, showing excellent integration of the skin graft and restoration of the first web space.

Palmar/oblique view of the reconstructed digits, demonstrating the restoration of digit length and the creation of a functional opposition post.

Final functional outcome: The patient demonstrates robust pinch strength, fine motor control, and the ability to hold a pen, highlighting the profound success of microsurgical toe-to-hand transfer.
Conclusion
Thumb and finger reconstruction via toe transfer is a highly complex, demanding procedure that requires profound anatomical knowledge, meticulous microsurgical skill, and rigorous postoperative care. Whether utilizing the great toe for isolated thumb loss or multiple toes for catastrophic hand injuries, these techniques offer unparalleled restoration of hand biomechanics, allowing patients to return to functional independence and, often, their previous occupations.
📚 Medical References
- toe-to-hand transfers, Ann Plast Surg 54:24, 2005.
- Lavin PA, Henderson CL, Vaghadia H: Non-alkalinized and alkalinized 2-chloroprocaine vs lidocaine for intravenous regional anesthesia during outpatient hand surgery, Can J Anaesth 46:939, 1999.
- Lilsanantti O, Luukkonen J, Rosenberg PH: High-dose bupivacaine, levobupivacaine and ropivacaine in axillary brachial plexus block, Acta Anaesthesiol Scand 48:601, 2004.
- McCartney CJL, Brull R, Chan VWS, et al: Early but no longterm benefi t of regional compared with general anesthesia for ambulatory hand surgery, Anesthesiology 101:461, 2004.
- Nystrom UM, Nystrom NA: Continuous cervical epidural anesthesia in reconstructive hand surgery, J Hand Surg 22A:906, 1997.
- Perris TM, Watt JM: The road to success: a review of 1000 axillary brachial plexus blocks, Anaesthesia 58:1220, 2003.
- Reuben SS, Duprat KM: Comparison of wound infi ltration with ketorolac versus intravenous regional anesthesia with ketorolac for postoperative analgesia following ambulatory hand surgery, Reg Anesth 21:565, 1996.
- Reuben SS, Steinberg RB, Klatt JL, et al: Intravenous regional anesthesia using lidocaine and clonidine, Anesthesiology 91:654, 1999.
- Rodriguez J, Barcena M, Lagunilla J, et al: Increased success rate with infraclavicular brachial plexus block using a dualinjection technique, J Clin Anesth 16:251, 2004.
- Rodriguez J, Barcena M, Taboada-Muniz M, et al: A comparison of single versus multiple injections on the extent of anesthesia with coracoid infraclavicular brachial plexus block, Anesth Analg 99:1225, 2004.
- Smith DW, Peterson MR, DeBerard SC: Regional anesthesia: nerve blocks of the extremities and face, Postgrad Med 106:69, 1999.
- Sylaidis P, Logan A: Epinephrine in digital blocks: revisited, Ann Plast Surg 43:572, 1999.
- Tham CHJ, Lim BH: A modifi cation of the technique for intravenous regional blockade for hand surgery, J Hand Surg 25B:575, 2000.
- Thompson WL, Malchow RJ: Peripheral nerve blocks and anesthesia of the hand, Mil Med 167:478, 2002.
- Turkan H, Baykai B, Ozisik T: Axillary brachial plexus block ade: an evaluation of three techniques, Mil Med 167:723, 2002.
- Vatashsky E, Aronson HB, Wexler MR, et al: Anesthesia in a hand surgery unit, J Hand Surg 5:495, 1980.
- Wilson KM: Distal forearm regional block anesthesia for
You Might Also Like