Surgical Management of Spastic Swan-Neck & Thumb Deformities
Key Takeaway
Swan-neck deformities in cerebral palsy result from intrinsic spasticity and secondary volar plate laxity at the proximal interphalangeal (PIP) joint. Surgical correction often requires the Curtis sublimis tenodesis to create a stabilizing flexion contracture. Concurrently, thumb-in-palm deformities are addressed via the Manske technique, redirecting the extensor pollicis longus to restore functional abduction and extension. This guide details the biomechanics, indications, and step-by-step surgical execution for these complex spastic hand reconstructions.
Introduction to Spastic Hand Deformities
The upper extremity in cerebral palsy (CP) presents a complex reconstructive challenge characterized by predictable patterns of muscle imbalance, spasticity, and secondary joint contractures. While flexion and pronation deformities of the wrist and elbow are most common, digital deformities—specifically the swan-neck deformity of the fingers and the thumb-in-palm deformity—can be profoundly disabling. These deformities severely compromise prehension, pinch kinematics, and overall hand function.
Surgical intervention is indicated when conservative measures, such as orthotic management and targeted botulinum toxin injections, fail to provide durable functional improvement or hygiene maintenance. This comprehensive guide details the pathoanatomy, biomechanical rationale, and step-by-step surgical execution for correcting spastic swan-neck deformities via the Curtis sublimis tenodesis, as well as addressing the concurrent thumb-in-palm deformity using the Manske extensor pollicis longus (EPL) redirection technique.
Pathoanatomy of Spastic Swan-Neck Deformity
Compared with other deformities of the upper extremity in cerebral palsy, swan-neck deformities of the fingers are relatively infrequent; however, when present, they severely disrupt the normal cascade of the hand and preclude effective grasp.
The deformity is characterized by hyperextension of the proximal interphalangeal (PIP) joint and reciprocal flexion of the distal interphalangeal (DIP) joint. In the spastic hand, this is driven by a combination of primary muscle overactivity and secondary capsuloligamentous failure:
1. Intrinsic Spasticity: Hypertonia of the interossei and lumbricals exerts excessive proximal pull on the lateral bands of the extensor mechanism.
2. Extensor Imbalance: The middle extensor band becomes relatively shortened compared to the lateral bands due to the relentless tension exerted by both the extrinsic long extensors and the spastic intrinsic muscles.
3. Volar Plate Attenuation: Over time, the constant hyperextension force leads to secondary ligamentous and capsular relaxation at the PIP joint. The volar plate becomes attenuated, allowing the joint to collapse into fixed hyperextension.
Clinical Pearl: Preoperative evaluation must differentiate between a flexible, dynamically driven swan-neck deformity and a fixed articular contracture. Diagnostic nerve blocks (e.g., ulnar motor block) can temporarily eliminate intrinsic spasticity, revealing the true extent of fixed capsular contracture and guiding surgical decision-making.
Surgical Management of Swan-Neck Deformity
Several surgical techniques have been described to address the spastic swan-neck deformity, broadly categorized into intrinsic releases, lateral band translocations, and volar tenodesis procedures.
Lateral Band Translocation (Historical Context)
Lateral band translocation, originally described by Zancolli and later modified by Tonkin, Hughes, and Smith, involves translocating the radial lateral band volarly beneath a soft tissue sling. This sling is typically created by suturing the accessory collateral ligament to the radial slip of the flexor digitorum sublimis (FDS).
While early results reported by Tonkin et al. in 12 patients were excellent, the follow-up was limited to less than one year. More recently, long-term outcome studies by de Bruin evaluated lateral band translocation for swan-neck deformity in CP patients and found a significant degradation of results over time. The success rate decreased precipitously from 84% at 1 year to 60% at 5 years. Due to this high recurrence rate in the face of relentless spasticity, many master surgeons have abandoned this technique in favor of more rigid tenodesis procedures.
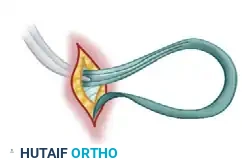
The Curtis Sublimis Tenodesis
For the spastic swan-neck deformity, the Curtis sublimis tenodesis of the PIP joint provides a highly reliable, durable mechanical block to hyperextension. By utilizing a slip of the FDS to create a tether across the volar aspect of the PIP joint, the surgeon induces a controlled, slight flexion contracture that resists the spastic extensor forces.
Step-by-Step Surgical Technique
Step 1: Exposure and Tendon Isolation
* Perform a volar Bruner zigzag incision or a mid-lateral incision over the affected PIP joint, extending from the mid-proximal phalanx to the mid-middle phalanx.
* Elevate the skin flaps, taking care to protect the neurovascular bundles.
* Incise the flexor tendon sheath, typically opening the C1 and A3 pulleys while meticulously preserving the A2 and A4 pulleys to prevent bowstringing.
* Retract the flexor digitorum profundus (FDP) tendon to expose the underlying FDS tendon at its bifurcation.
Step 2: FDS Slip Preparation and Bone Tunneling
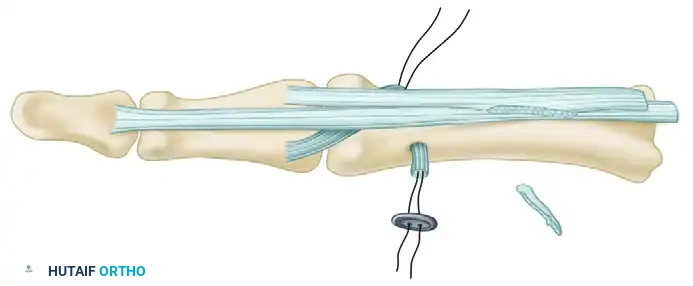
* Identify the two slips of the FDS tendon. Divide one half of the FDS tendon (typically the ulnar slip) at the level of its bifurcation, leaving its distal insertion intact.
* Using a small drill bit or burr, create a transverse or oblique osseous tunnel through the proximal phalanx, just proximal to the PIP joint articular surface.
Step 3: Tendon Routing and Fixation
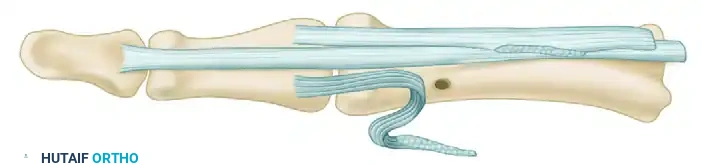
* Take the freed proximal end of the divided FDS slip and route it deep to the FDP tendon, carrying it to the opposite side of the proximal phalanx.
* Thread the tendon slip through the prepared osseous hole in the proximal phalanx.
* Anchor the tendon to the dorsal cortex using a pull-out suture over a button.
* Tensioning: The tendon must be anchored under sufficient tension to cause a slight flexion contracture of the PIP joint (typically 10 to 20 degrees). This mechanical tether prevents recurrent hyperextension and locking.

Surgical Warning: Over-tensioning the tenodesis can result in a severe PIP flexion contracture, exchanging a swan-neck deformity for a boutonniere-type posture. Ensure the tension allows for full passive flexion while blocking extension at exactly 10-15 degrees short of neutral.
Pathoanatomy of Thumb-in-Palm Deformity
The thumb-in-palm deformity is one of the most common and debilitating manifestations of the spastic upper extremity. It effectively traps the thumb within the palm, blocking the entry of objects into the hand and destroying pinch and grasp capabilities.
The deformity is multifactorial, driven by:
1. Spasticity of the Adductors and Flexors: Hypertonia of the adductor pollicis, flexor pollicis brevis (FPB), and first dorsal interosseous muscles pulls the first metacarpal into severe adduction and flexion.
2. Weakness of the Extensors and Abductors: The abductor pollicis longus (APL), extensor pollicis brevis (EPB), and extensor pollicis longus (EPL) are typically weak and overstretched, unable to counteract the spastic volar forces.
3. Joint Instability: The metacarpophalangeal (MCP) joint often becomes unstable. When the patient attempts to extend the thumb, the EPL (acting across a flexed and adducted metacarpal) paradoxically hyperextends the MCP joint rather than abducting the thumb out of the palm.
The Manske Technique for Thumb-in-Palm Deformity
To correct the thumb-in-palm deformity, soft tissue releases (e.g., adductor origin release, fractional lengthening of the flexor pollicis longus) are often required. However, restoring active abduction and extension is critical for functional recovery.
The Manske technique addresses this by redirecting the EPL tendon. By altering its anatomical routing, the EPL's moment arm is shifted. It is converted from a primary IP/MCP joint extensor into a robust abductor and MCP joint stabilizer, directly counteracting the spastic adductor forces.
Step-by-Step Surgical Technique
Step 1: Incision and Exposure
* Make a dorsal longitudinal or gently curved incision over the first metacarpal, extending proximally over the anatomic snuffbox and distally to the interphalangeal joint of the thumb.

- Carefully dissect through the subcutaneous tissues, identifying and protecting the sensory branches of the superficial radial nerve.
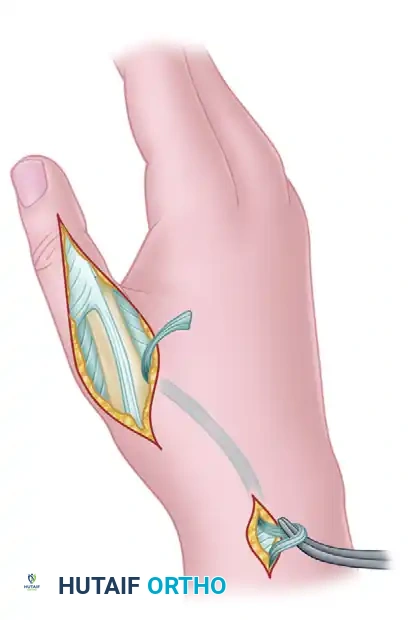
Step 2: EPL Mobilization and Redirection
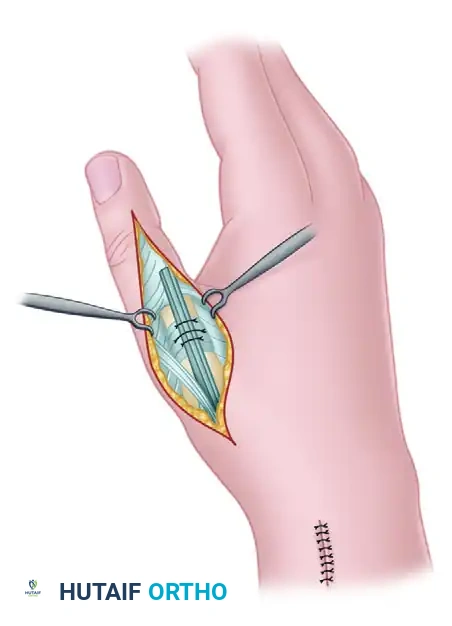
* Identify the EPL tendon within the third dorsal extensor compartment. Release the retinaculum over the third compartment and mobilize the EPL tendon proximally to its musculotendinous junction.
* Redirect the EPL tendon radially toward the first dorsal compartment.
* Attempt to route the EPL through the first dorsal compartment alongside the APL and EPB tendons.
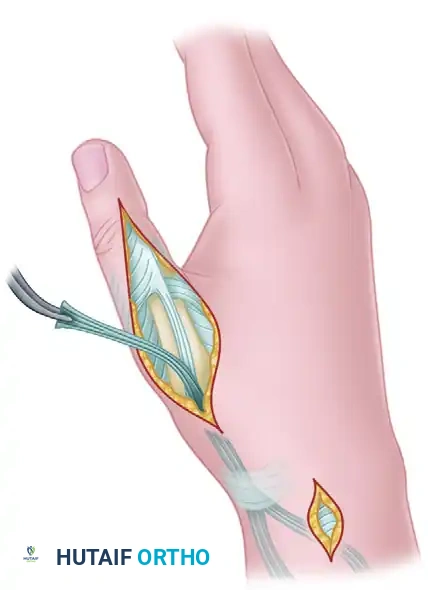
Surgical Pearl: If redirecting the tendon through the first compartment is excessively tight or difficult, the EPL can be safely routed subcutaneously around the EPB and APL tendons just proximal to the retinacular compartment, directing it into the dorsal incision on the thumb.
Step 3: MCP Joint Capsular Tunneling
* Expose the dorsal capsule of the thumb MCP joint.
* Create a transverse tunnel directly through the robust tissue of the MCP joint capsule.
* Pass the redirected EPL tendon through this transverse capsular tunnel.
- Addressing MCP Hyperextension: If the MCP joint is clinically hyperextensible (a common finding in thumb-in-palm deformities), this capsular tunnel must be placed proximal to the articular surface. This proximal placement creates a tenodesis effect that actively resists further hyperextension.
- In situations of severe MCP instability, insert a temporary 0.045-inch Kirschner wire (K-wire) across the MCP joint, pinning it in 10 to 15 degrees of slight flexion to protect the repair during healing.
Step 4: Distal Fixation and Tensioning
* Apply traction to the EPL tendon. It must be sutured under sufficient tension to advance it 1 to 2 cm from its original resting position, compensating for chronic overstretching.
* Suture the distal portion of the EPL tendon directly into the extensor aponeurosis. This critical step closes the longitudinal defect created during mobilization and prevents an iatrogenic flexion deformity at the interphalangeal joint.
- Verify the resting posture of the thumb. It should sit comfortably in palmar abduction and extension without excessive tension on the skin edges.

Step 5: Closure
* Deflate the tourniquet, achieve meticulous hemostasis, and close the incisions in a routine fashion using non-absorbable monofilament sutures for the skin.
Postoperative Care and Rehabilitation Protocol
The success of spastic hand reconstruction relies heavily on rigid adherence to postoperative immobilization and subsequent specialized hand therapy. The spasticity of the antagonist muscles will relentlessly challenge the surgical repair if not properly protected.
Phase I: Strict Immobilization (Weeks 0-4)
- Immediately postoperatively, the thumb and wrist are immobilized in a well-padded, short-arm thumb spica cast.
- The thumb must be meticulously positioned in wide palmar abduction and extension to relieve tension on the EPL transfer and maintain the stretch on the released adductor musculature.
- The cast remains in place undisturbed for exactly 4 weeks.
Phase II: Pin Removal and Transition (Week 4)
- At the 4-week mark, the cast is bivalved and removed.
- If a temporary Kirschner wire was inserted across the metacarpophalangeal joint to protect against hyperextension, it is extracted in the clinic at this time.
- The patient is immediately transitioned into a custom-molded thermoplastic removable thumb spica splint.
Phase III: Controlled Mobilization (Weeks 4-6)
- The removable thumb spica splint is worn continuously for an additional 2 weeks (up to 6 weeks postoperatively).
- During this period, the splint is removed strictly three to four times daily for controlled, active, and active-assisted range of motion exercises under the guidance of a specialized hand therapist.
- Passive stretching of the reconstructed EPL is strictly avoided to prevent attenuation of the transfer.
Phase IV: Long-Term Maintenance (Weeks 6+)
- Daytime splinting is gradually weaned as active control and strength improve.
- Critical Requirement: Nighttime splinting in abduction and extension must be maintained for a minimum of 6 months (and often indefinitely in severe CP) to prevent the recurrence of spastic contractures. The underlying upper motor neuron lesion remains unchanged, and lifelong orthotic vigilance is often the only safeguard against deformity recurrence.
📚 Medical References
- swan-neck deformity in the cerebral palsied hand, Clin Orthop Relat Res 48:167, 1966.
- Swanson AB: Surgery of the hand in cerebral palsy and muscle origin release procedures, Surg Clin North Am 48:1129, 1968.
- Tonkin MA, Hatrick NC, Eckersley JRT, et al: Surgery for cerebral palsy: Part 3. Classifi cation and operative procedures for thumb deformity, J Hand Surg 26B:465, 2001.
- Van Heest AE: Surgical management of wrist and fi nger deformity, Hand Clin 19:657, 2003.
- Van Heest AE, House JA, Cariello C: Upper extremity surgical treatment of cerebral palsy, J Hand Surg 24A:323, 1999.
- Wenner SM, Johnson KA: Transfer of the fl exor carpi ulnaris to the radial wrist extensors in cerebral palsy, J Hand Surg 13A:231, 1988.
- Williams R, Haddad RJ: Release of fl exor origin for spastic deformities of the wrist and hand, South Med J 60:1033, 1967.
- Wolf TM, Clinkscales CM, Hamlin C: Flexor carpi ulnaris tendon transfers in cerebral palsy, J Hand Surg 23B:340, 1998.
- Wright PA, Granat MH: Improvement in hand function and wrist range of motion following electrical stimulation of wrist extensor muscles in an adult with cerebral palsy, Clin Rehabil 14:244, 2000.
- Wright PA, Granat MH: Therapeutic effects of functional electrical stimulation of the upper limb of eight children with cerebral palsy, Dev Med Child Neurol 42:724, 2000.
- Zancolli EA, Goldner LJ, Swanson AB: Surgery of the spastic hand in cerebral palsy. Report of the Committee on Spastic Hand Evaluation, J Hand Surg 8A:766, 1983.
You Might Also Like

