Orthopaedic Splinting: Advanced Principles, Biomechanics, and Surgical Techniques
Key Takeaway
Splinting is a fundamental orthopaedic intervention designed to immobilize tissues, correct deformities, and compensate for motor deficits. This comprehensive guide details the biomechanical principles of static and dynamic splinting, specific applications for peripheral nerve palsies, and evidence-based postoperative elevation protocols. Mastery of these techniques ensures optimal functional recovery, prevents contractures, and mitigates complications such as pressure necrosis in the rehabilitating hand and upper extremity.
Introduction to Orthopaedic Splinting
Splinting is an indispensable adjunct in operative orthopaedics, particularly in the management of the hand and upper extremity. The application of a well-designed orthosis serves as the critical bridge between surgical intervention and functional rehabilitation. In the postoperative or post-traumatic setting, splinting serves three primary, distinct purposes:
- Immobilization and Tissue Protection: To immobilize all or part of the hand in a physiological position that promotes optimal fibroplasia, protects healing repairs (tendon, nerve, or bone), and prevents the development of secondary deformities.
- Deformity Correction: To apply controlled, sustained mechanical forces to correct an existing contracture or deformity, thereby promoting the restoration of normal kinematic function.
- Motor Compensation: To supply external power to compensate for profound muscular weakness or paralysis, most notably in the setting of peripheral nerve palsies, allowing the patient to maintain functional prehension and grasp during the period of nerve regeneration.
Orthopaedic splints are broadly categorized into two functional classifications: static splints, which function to prevent motion and maintain a specific posture, and dynamic splints, which utilize elastic components to assist motion, provide continuous tension, or substitute for absent muscle power.
Clinical Pearl: The ideal immobilizing splint should be utilized for a limited, strictly defined duration. Prolonged, indiscriminate immobilization is the primary catalyst for iatrogenic joint stiffness. The splint must permit unaffected adjacent joints to function as normally as possible to maintain the gliding planes of uninjured tendons.
Biomechanical Principles of Splinting
The design and application of any splint must respect the complex biomechanics and viscoelastic properties of the hand.
Static vs. Dynamic Splinting
- Static Splints: These devices have no moving parts. They are utilized primarily for rest, protection, and positioning. When used to correct contractures, they are often applied as "static progressive" splints, which are periodically remolded to accommodate tissue elongation via the biomechanical principle of stress relaxation (a decrease in stress over time under a constant strain).
- Dynamic Splints: These incorporate moving parts, such as rubber bands, springs, or elastic cords. They apply a constant, gentle force to the tissues, utilizing the principle of creep (progressive tissue elongation under a constant load). Dynamic splints are highly effective in mobilizing stiff joints and substituting for paralyzed musculature.
Material and Fabrication Considerations
Modern splints are typically fabricated from low-temperature thermoplastic materials. These materials must be lightweight, durable, and highly conformable.
Surgical Warning: Care must be taken to ensure that the splint does not cause excessive skin pressure, particularly over bony prominences and superficial joints. Pressure sores can develop rapidly, leading to full-thickness skin necrosis, deep infection, and catastrophic interference with the postoperative therapy program.
An experienced orthotist or certified hand therapist (CHT) should be available for fabricating complex designs and making technical adjustments requiring specialized skills. However, the patient must be thoroughly educated on how to apply the splint, remove it safely, and make minor adjustments to ensure compliance.
Postoperative Management and Elevation Protocols
Postoperative edema is the primary enemy of the healing hand. Edema fluid is protein-rich; if allowed to stagnate, it organizes into dense fibrotic adhesions that bind the delicate gliding layers of tendons and ligaments, leading to irreversible stiffness. Strict postoperative elevation is mandatory.
Clinical Methods of Elevation
Elevation must place the hand strictly above the level of the heart to facilitate venous and lymphatic drainage.
FIGURE 64-31 (A): Postoperative elevation can be maintained with a specialized sling that keeps the hand higher than the elbow, utilizing gravity to assist venous return.

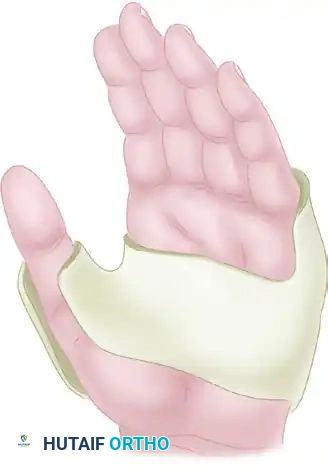
FIGURE 64-31 (B): Alternatively, a preformed rubber sponge block can be utilized in the supine patient to maintain rigid, comfortable elevation without relying on patient compliance.
The Pillow and Towel Method
Maintaining elevation while the patient is sleeping is notoriously difficult. A highly effective, simple method for home elevation utilizes standard household items: two standard-sized pillows, two rolled-up bath towels, and several large safety pins.

Surgical Diagram A: The foundation of the elevation construct. Two rolled towels are placed parallel to each other.
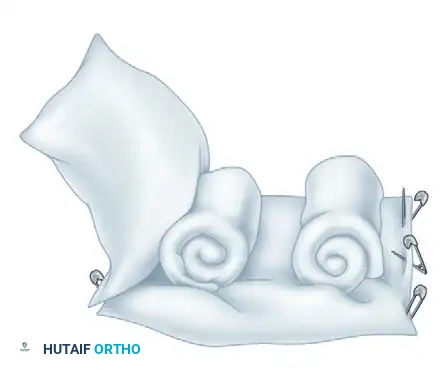
Surgical Diagram B: The towels are secured within the folds of the pillows using large safety pins, creating a stable trough.

Surgical Diagram C: The patient's forearm is placed securely between the bath towels inside the two pillows. This construct allows the patient to sleep comfortably on their back or side while hugging the pillows, ensuring the hand remains elevated throughout the night.
Splinting for Peripheral Nerve Palsies
Peripheral nerve injuries result in predictable patterns of motor loss and subsequent postural deformities due to the unopposed pull of intact antagonist muscles. Splinting is critical to prevent these contractures and to provide functional assistance.
Median Nerve Palsy
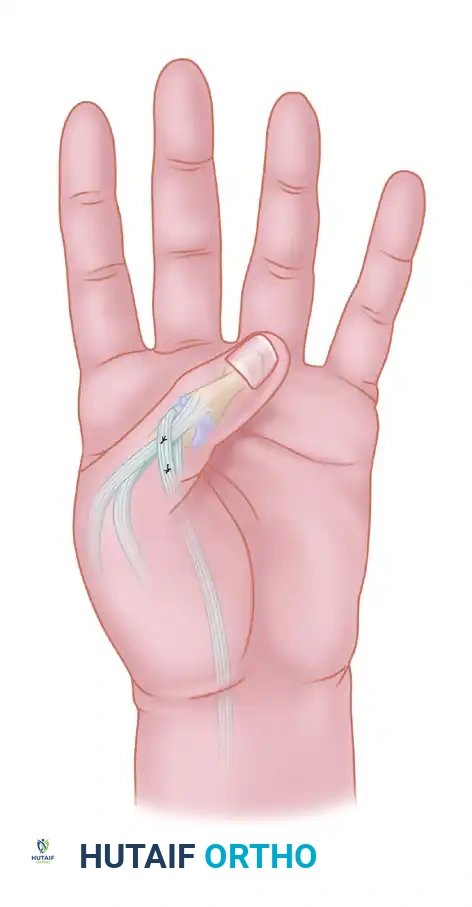
Low median nerve palsy (e.g., severe carpal tunnel syndrome or distal laceration) results in the loss of the thenar intrinsic muscles (abductor pollicis brevis, opponens pollicis, and the superficial head of the flexor pollicis brevis). This leads to an adduction contracture of the thumb and the inability to perform palmar abduction and opposition, severely crippling pinch and grasp.

FIGURE 64-34: Splint for low median nerve palsy. This lightweight, compact orthosis dynamically holds the thumb in abduction, extension, and opposition. By maintaining the first web space, it prevents a devastating adduction contracture while the nerve regenerates or prior to an opponensplasty tendon transfer.
Ulnar Nerve Palsy
Ulnar nerve palsy paralyzes the interossei and the ulnar two lumbricals. The loss of intrinsic muscle function at the ring and little fingers removes the primary flexors of the metacarpophalangeal (MCP) joints and the primary extensors of the interphalangeal (IP) joints. The unopposed extensor digitorum communis (EDC) hyperextends the MCP joints, while the unopposed flexor digitorum profundus (FDP) flexes the IP joints, resulting in the classic "claw hand" (intrinsic-minus posture).
Splinting for ulnar nerve palsy aims to block MCP hyperextension. By stabilizing the MCP joint in slight flexion, the force of the extrinsic EDC is transmitted distally to the central slip and lateral bands, allowing the patient to actively extend the IP joints (the Bouvier principle).

FIGURE 64-36: A static splint for ulnar nerve palsy. This low-profile orthosis prevents hyperextension deformity of the MCP joints of the ring and little fingers. It conforms perfectly to the shape of the transverse metacarpal arch and has no bulky attachments that hinder the overall function of the hand.

FIGURE 64-35: A dynamic splint for ulnar nerve palsy. This device dynamically forces the MCP joints of the ring and little fingers into flexion. However, a significant disadvantage of this specific design is that part of the palm is covered by rubber bands, which interferes with tactile feedback and grasp mechanics.
Radial Nerve Palsy
High radial nerve palsy results in the loss of wrist extension, finger extension at the MCP joints, and thumb extension/radial abduction. The resulting "wrist drop" severely impairs grip strength due to the loss of the normal tenodesis effect (active wrist extension is required for optimal flexor tendon excursion).

FIGURE 64-38: Splint for high radial nerve palsy. This dynamic orthosis supports the wrist in functional extension while dynamically splinting the digits and thumb in extension via elastic outriggers. This allows the patient to actively flex the digits to grasp objects, while the splint passively re-extends the digits to release the grasp.
Specialized Splinting Techniques
Beyond nerve palsies, specific splints are utilized for targeted joint mobilization and fracture management.
Dynamic Flexion Splinting
Stiffness in extension is a common complication following crush injuries, extensor tendon repairs, or prolonged immobilization.
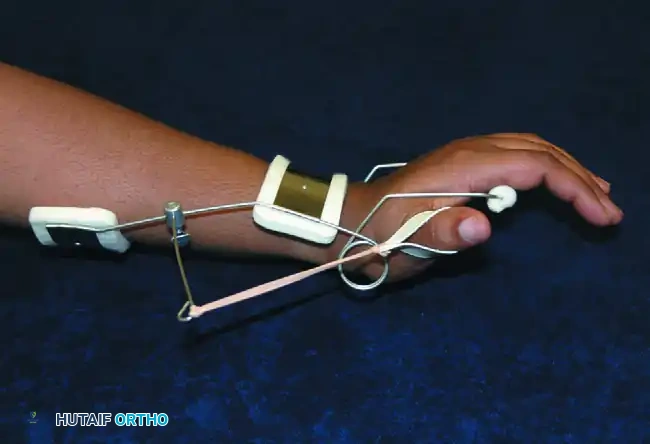
FIGURE 64-37: The Flexor Glove. This device dynamically forces the fingers into flexion, exerting continuous, gentle creep force on the proximal interphalangeal (PIP) and MCP joints. Care must be taken regarding the vector of pull; if the proximal eyelets are positioned too far proximally, it may inadvertently flex the wrist. When desirable, it may be applied over a rigid volar wrist splint to isolate the flexion force to the digits.
Digital Gutter Splints
For isolated phalangeal fractures, ligamentous sprains, or soft tissue injuries, localized immobilization is preferred to avoid stiffening adjacent uninjured digits.

FIGURE 64-39: Preformed plastic gutter splints for digits. These are easily adjustable in length, highly radiolucent, and provide excellent rigid support for soft tissue or fracture healing while allowing the unaffected fingers full range of motion.
Proximal Interphalangeal (PIP) Joint Splinting
The PIP joint is notoriously prone to flexion contractures due to the complex anatomy of the volar plate and collateral ligaments.
FIGURE 64-40: Proximal interphalangeal extension splint. This three-point pressure splint (often utilizing a Capener or dynamic spring design) applies a constant extension moment to the PIP joint while allowing active flexion, crucial for treating Boutonniere deformities or postoperative flexion contractures.
Patient Education and Compliance
The ultimate success of any splinting regimen relies heavily on patient compliance. The patient must thoroughly understand the biomechanical rationale for splint wear.
- Education: Explain the difference between resting splints and mobilizing splints.
- Skin Checks: Instruct the patient to perform frequent skin checks, looking for areas of erythema that do not blanch or resolve within 20 minutes of splint removal.
- Assessment: As treatment progresses, the surgeon and therapist can determine faithful use by observing the patient’s skill and fluidity in applying and removing the splint during follow-up clinic visits.
Pitfall: A splint that is too heavy, too bulky, or painful will simply not be worn. The best biomechanical design is useless if it remains in the patient's bag. Always prioritize a low-profile, comfortable fit.
Evidence-Based Perioperative Considerations
The application of splints often follows complex surgical procedures of the hand and upper extremity. A comprehensive understanding of the perioperative environment is essential for the operating surgeon.
Regional Anesthesia in Hand Surgery
The use of regional anesthesia has revolutionized ambulatory hand surgery. Ultrasound-guided brachial plexus blocks (axillary, infraclavicular, or supraclavicular) provide excellent intraoperative anesthesia and prolonged postoperative analgesia, which is critical for early tolerance of splinting and therapy.
* Efficacy: Studies by Abrahams et al. and Kapral et al. demonstrate that ultrasound guidance significantly improves the success rate and safety profile of peripheral nerve blocks compared to traditional electrical neurostimulation.
* Outpatient Benefits: Chan et al. and Hadzic et al. have shown that regional anesthesia offers superior intraoperative cardiovascular stability, reduces postoperative nausea, and significantly decreases hospital discharge times compared to general anesthesia.
Tourniquet Management
Bloodless fields are mandatory for meticulous hand surgery. However, tourniquet pain can limit the duration of procedures performed under local or intravenous regional anesthesia (Bier block).
* Forearm vs. Upper Arm: Research by Maury and Roy and Edwards et al. indicates that forearm tourniquets are significantly better tolerated by patients than traditional upper arm tourniquets, allowing for longer operative times under local anesthesia without the need for deep sedation.
Prophylactic Antibiotics and Anticoagulation
- Antibiotics: The routine use of prophylactic antibiotics in clean, elective hand surgery remains controversial. Studies by Rizvi et al. and Bykowski et al. suggest that in strictly elective, non-implant cases, the infection rate is exceptionally low, and routine prophylaxis may not be warranted.
- Anticoagulation: Historically, patients were instructed to cease anticoagulants prior to surgery. However, contemporary evidence (Wallace et al., Smit and Hooper) strongly supports continuing warfarin and other systemic anticoagulants for minor elective hand surgeries, as the risk of a thromboembolic event far outweighs the easily manageable risk of local hematoma.
Conclusion
Orthopaedic splinting is a dynamic, evolving science that requires a profound understanding of upper extremity anatomy, tissue biomechanics, and postoperative healing phases. Whether utilizing a static progressive orthosis to overcome a stubborn PIP contracture or a dynamic outrigger to substitute for a paralyzed radial nerve, the surgeon must prescribe splints with the same precision and care as a surgical incision. Through meticulous fabrication, rigorous patient education, and strict adherence to elevation protocols, splinting maximizes functional outcomes and ensures the success of the operative intervention.
You Might Also Like