Reverse Wedge Osteotomy and Management of Madelung Deformity
Key Takeaway
The Carstam and Theander reverse wedge osteotomy is a definitive surgical intervention for correcting angular deformities caused by a delta phalanx. By excising a central osseous wedge, reversing its orientation, and reinserting it as an interpositional graft, surgeons can restore longitudinal alignment while preserving physeal growth potential. This technique is highly effective in pediatric patients presenting with severe clinodactyly.
INTRODUCTION TO CONGENITAL HAND AND WRIST DEFORMITIES
Congenital anomalies of the upper extremity present unique biomechanical and developmental challenges for the orthopaedic surgeon. Two distinct but highly significant pathologies frequently encountered in pediatric hand surgery are the delta phalanx (often resulting in severe clinodactyly) and Madelung deformity of the wrist.
While a delta phalanx is a localized digital anomaly characterized by a longitudinally bracketed epiphysis, Madelung deformity represents a complex, often genetically driven, multi-planar deformity of the radiocarpal and distal radioulnar joints. This comprehensive guide details the evidence-based management of both conditions, with a primary focus on the Carstam and Theander Reverse Wedge Osteotomy for the correction of a delta phalanx.
PART I: THE DELTA PHALANX AND REVERSE WEDGE OSTEOTOMY
Pathoanatomy and Biomechanics of the Delta Phalanx
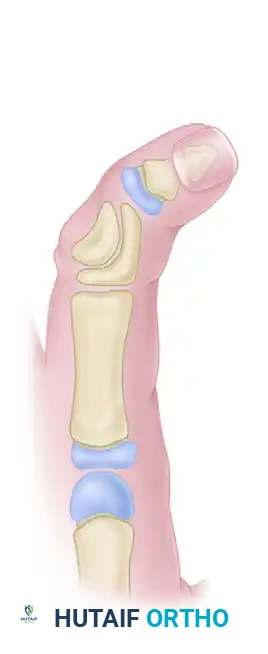
A delta phalanx is an abnormally shaped, triangular bone that causes progressive angular deformity in the digits, most commonly presenting as clinodactyly. The fundamental pathoanatomic lesion is a Longitudinally Bracketed Epiphysis (LBE).
Instead of a normal transverse physis at the base of the phalanx, the physis extends longitudinally along one side of the diaphysis, effectively tethering longitudinal growth on that side while allowing continued growth on the contralateral side. This asymmetric growth results in a progressive, rigid angular deformity. The middle phalanx of the small finger is the most frequently affected site, though it can occur in any digit, including the thumb.
Clinical Pearl: Simple closing wedge osteotomies are generally contraindicated for a delta phalanx. Because the affected digit is already pathologically short, a closing wedge will exacerbate the shortening. The Carstam and Theander reverse wedge osteotomy is the gold standard because it corrects the angulation while maintaining, or even slightly increasing, digital length.
Indications for Surgery
Conservative management (such as splinting) is entirely ineffective for a delta phalanx due to the rigid, osseous tethering of the bracketed epiphysis. Surgical intervention is indicated when:
* The angular deformity exceeds 20 to 30 degrees.
* The deformity causes functional impairment, such as overlapping digits during grip.
* The deformity is rapidly progressive in a young, growing child.
The ideal age for surgical intervention is typically between 2 and 6 years. Intervening early prevents secondary soft tissue contractures and allows the remodeled phalanx to grow normally.
Surgical Technique: Carstam and Theander Reverse Wedge Osteotomy
The Carstam and Theander technique is an elegant, length-preserving osteotomy. By excising the central wedge of the deformed bone, rotating it 180 degrees, and reinserting it, the surgeon simultaneously corrects the angular deformity and disrupts the abnormal longitudinal physis.
Anesthesia and Positioning:
The procedure is performed under general anesthesia. The patient is positioned supine with the affected arm extended on a radiolucent hand table. A pediatric pneumatic tourniquet is applied to the upper arm to ensure a bloodless field. Loupe magnification (2.5x to 3.5x) is highly recommended.
Step 1: Surgical Approach and Exposure
- Under tourniquet control, make a curved dorsal or mid-axial incision over the involved phalanx. The incision should extend from the distal portion of the proximal phalanx, traverse the entire length of the middle phalanx, and end at the proximal portion of the distal phalanx.
- Carefully elevate the skin flaps, preserving the dorsal sensory nerve branches and the delicate venous network.
Step 2: Extensor Mechanism Management
- Mobilize the edges of the extensor tendon apparatus to expose the underlying periosteum and bone.
- It is critical to visualize both the radial and ulnar borders of the delta phalanx.
- Identify and meticulously protect the insertion of the central extensor slip at the base of the middle phalanx. Damage to this structure will result in a secondary boutonnière deformity.
Figure A: Illustration of the pre-operative delta phalanx involving the middle phalanx, demonstrating the characteristic triangular shape and resulting angular deformity.
Step 3: Execution of the Osteotomy
- Identify the apex of the deformity.
- Remove a wedge-shaped piece of bone from the central portion of the delta phalanx.
- Instrument Selection: In infants and very young children, the bone is largely cartilaginous and the wedge can often be excised using a sharp #15 scalpel. In older children with more ossified bone, carefully pick away the wedge using sharp pediatric bone cutters or a fine osteotome, as described by Flatt.
- Ensure the osteotomy completely transects the abnormal longitudinal bracketed epiphysis to prevent recurrence.
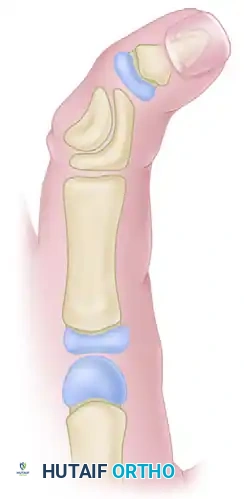
Figure B: The wedge-shaped piece of bone has been carefully excised from the central portion of the delta phalanx, creating a void that allows for the correction of the angular deformity.
Step 4: Wedge Reversal and Fixation
- Take the excised wedge-shaped piece of bone and reverse it 180 degrees.
- Manually correct the angular deformity of the digit, opening the concave side and closing the convex side.
- Insert the reversed wedge into the osseous defect. The wide base of the wedge should now sit on the previously concave side of the phalanx, acting as an interpositional structural graft that maintains the corrected alignment.
- Place a longitudinal Kirschner wire (typically 0.028-inch or 0.035-inch, depending on patient size) to secure the construct. Drive the K-wire retrograde through the distal phalanx, across the distal interphalangeal (DIP) joint, through the reconstructed middle phalanx, and into the proximal phalanx to hold the corrected position.
- Leave the K-wire protruding through the distal tip of the finger. Bend the tip and cap it to prevent migration and protect the patient.

Figure C: The wedge is reversed and reinserted. A longitudinal Kirschner wire is driven across the joints to provide rigid internal fixation of the corrected alignment.
Step 5: Closure
- Deflate the tourniquet and achieve meticulous hemostasis.
- Repair the extensor mechanism if it was split, using fine absorbable sutures (e.g., 5-0 Vicryl).
- Close the skin with interrupted non-absorbable sutures (e.g., 5-0 or 6-0 Nylon).
- Apply a sterile, non-adherent dressing followed by a well-padded short-arm splint that incorporates the affected digit in a safe position.
Surgical Warning: Failure to completely resect or disrupt the longitudinal bracketed epiphysis during the wedge excision will almost certainly lead to recurrence of the clinodactyly as the child grows.
Postoperative Care and Rehabilitation
- Immobilization: The splint and the protruding Kirschner wire are maintained for 4 to 6 weeks postoperatively.
- Pin Care: The pin site at the fingertip must be kept clean and dry to prevent superficial tracking infections.
- Hardware Removal: At the 4 to 6-week mark, clinical and radiographic healing is assessed. Once bridging callus is visible and the osteotomy site is stable, the K-wire is removed in the clinic.
- Rehabilitation: Gradually increased activity and active range of motion (AROM) exercises are permitted. Passive range of motion (PROM) and dynamic splinting may be initiated if joint stiffness persists.
PART II: MADELUNG DEFORMITY
While the delta phalanx affects the digits, Madelung deformity is a profound, progressive anomaly of the wrist. First described by Malgaigne in 1855 and later definitively characterized by Otto Madelung in 1878, this condition presents a complex reconstructive challenge.
Pathogenesis and the Ligament of Vickers
Madelung deformity is characterized by a growth disturbance of the volar-ulnar aspect of the distal radial physis. This asymmetric growth arrest leads to a multi-planar deformity:
1. Volar tilt of the distal radial articular surface.
2. Ulnar inclination of the distal radius.
3. Dorsal subluxation of the distal ulna (relative to the carpus and radius).
4. Proximal subsidence of the lunate into the widened distal radioulnar joint (DRUJ).
The primary anatomical culprit in idiopathic and genetic cases is the Ligament of Vickers. Vickers described an abnormal, hypertrophic radiolunate ligament that tethers the lunate to the distal radius, originating proximal to the physis. This unyielding ligament acts as a physical tether, impeding the growth of the ulnopalmar aspect of the distal radius and causing the characteristic volar-ulnar curvature.
Genetic and Syndromic Associations
Madelung deformity is a rare anomaly, accounting for approximately 1.7% of all congenital hand anomalies. It is predominantly bilateral and affects females significantly more often than males. The condition is frequently transmitted in an autosomal dominant pattern with variable penetrance.
Recent genetic advancements have identified mutations in the homeobox gene SHOX (Short Stature Homeobox), located at the pseudoautosomal region 1 of both the X and Y chromosomes, as a primary causative factor.
Madelung deformity is the hallmark wrist anomaly in Dyschondrosteosis (Léri-Weill syndrome), the most common form of mesomelic dwarfism. This syndrome presents with:
* Mild shortness of stature.
* Mesomelic shortening (shortness of the middle segments of the extremities, i.e., forearms and lower legs).
* Bilateral Madelung deformities.
Other associated systemic conditions include:
* Turner syndrome (XO karyotype, frequently associated with SHOX haploinsufficiency).
* Mucopolysaccharidosis (e.g., Hurler syndrome).
* Achondroplasia and Multiple Epiphyseal Dysplasia.
* Multiple Hereditary Exostoses (Diaphyseal aclasis).
* Ollier disease (Enchondromatosis).
Classification of Madelung Deformities
Vender and Watson classified Madelung and Madelung-like deformities into four distinct etiological groups:
1. Idiopathic: Classic presentation, often bilateral, with a positive family history but no systemic syndrome.
2. Genetic/Syndromic: Associated with defined chromosomal or genetic anomalies (e.g., Dyschondrosteosis, Turner syndrome).
3. Dysplastic: Associated with generalized bone dysplasias (e.g., Multiple exostoses, Ollier disease).
4. Posttraumatic: Acquired deformity resulting from repetitive microtrauma (e.g., in young gymnasts) or a specific physeal crush injury (Salter-Harris V) to the volar-ulnar distal radius.
Diagnostic Pearl: Vender and Watson suggested that acquired (posttraumatic) deformities can usually be distinguished from congenital forms by their unilaterality, a clear history of trauma or repetitive stress, less severe carpal derangement, and the absence of the classic Vickers ligament on MRI.
Clinical Presentation and Radiographic Evaluation
Clinical Signs:
The deformity is rarely obvious at birth. It typically manifests in late childhood or early adolescence (ages 8 to 14) during the pubertal growth spurt. Patients present with:
* Volar subluxation of the hand.
* A prominent, dorsally displaced distal ulnar head.
* Decreased wrist range of motion (particularly extension and supination).
* Minimal pain initially, though ulnocarpal impaction pain may develop as the deformity progresses.
Radiographic Findings:
Standard posteroanterior (PA) and lateral radiographs of the wrist reveal pathognomonic changes:
* Radius: The radius is curved with a dorsal and radial convexity. The distal articular surface is severely angulated in a volar and ulnar direction. The distal radial epiphysis appears triangular due to the failure of growth in the ulnar and volar aspects.
* Ulna: The ulna is relatively long compared to the shortened radius, resulting in positive ulnar variance. The ulnar head is enlarged and subluxated dorsally.
* Carpus: The carpus subluxates ulnarward and palmarward. The lunate acts as the apex of a wedge, subsiding proximally into the widened DRUJ.
* Osteophytes: Osteophyte formation may be visible at the volar-ulnar border of the radius, representing the osseous origin of the Vickers ligament.
Treatment Algorithm for Madelung Deformity
Conservative Management:
Because many children with Madelung deformity maintain excellent function and experience minimal pain despite the striking clinical appearance, a conservative approach is warranted initially. Observation, activity modification, and intermittent splinting for pain flare-ups are the mainstays of non-operative care.
Surgical Intervention:
Surgery is indicated for severe, progressive deformity, persistent pain (usually secondary to ulnocarpal impaction), or severe restriction of forearm rotation.
Surgical options are tailored to the patient's skeletal maturity:
* Early Intervention (Skeletally Immature): Physioloysis (release of the Vickers ligament) combined with dome osteotomy of the distal radius and/or epiphysiodesis of the distal ulna. Releasing the tether early can allow the remaining open physis to correct the deformity through subsequent growth.
* Late Intervention (Skeletally Mature): Corrective radial osteotomies (e.g., closing wedge or dome osteotomies) to restore the articular tilt, combined with ulnar shortening osteotomy or a Darrach procedure/Sauvé-Kapandji procedure to address the distal radioulnar joint incongruity and ulnocarpal impaction.
CONCLUSION
Both the delta phalanx and Madelung deformity represent complex disruptions of normal physeal growth. Mastery of the Carstam and Theander reverse wedge osteotomy provides the orthopaedic surgeon with a reliable, length-preserving technique to correct severe digital clinodactyly. Similarly, a deep understanding of the genetic basis, biomechanical tethering (Vickers ligament), and multi-planar nature of Madelung deformity is essential for appropriate patient counseling and surgical reconstruction of the pediatric wrist.
You Might Also Like