Resection of Dyschondrosteosis Lesion: Vickers Technique

Key Takeaway
The Vickers and Nielsen technique for dyschondrosteosis involves the resection of the physeal bar and the abnormal volar Vickers ligament tethering the lunate to the radius. This procedure relieves the tethering effect on the volar-ulnar distal radius, allowing for corrective growth in skeletally immature patients with Madelung deformity. Key steps include precise physiolysis, ligament excision, and fat graft interposition to prevent recurrent bar formation.
INTRODUCTION TO DYSCHONDROSTEOSIS AND MADELUNG DEFORMITY
Léri-Weill dyschondrosteosis is a pseudoautosomal dominant skeletal dysplasia classically associated with mutations or deletions in the SHOX gene. Clinically, it manifests as mesomelic short stature and the characteristic Madelung deformity of the wrist. The hallmark of this deformity is a premature growth arrest of the volar-ulnar aspect of the distal radial physis, leading to an increased volar tilt, increased radial inclination, and secondary dorsal subluxation of the distal ulna.
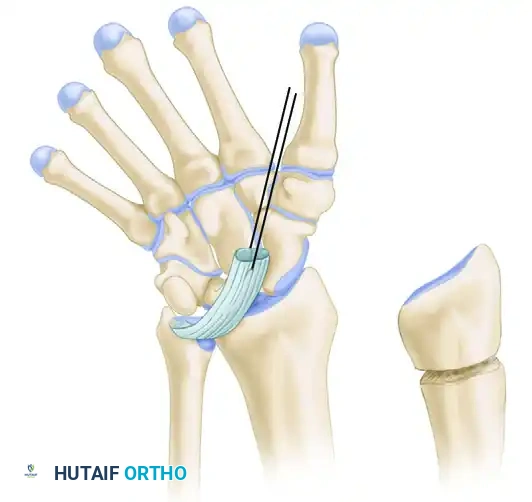
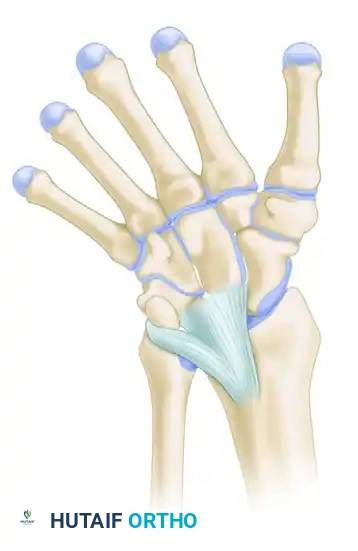
A critical pathoanatomic feature of this condition is the presence of the Vickers ligament—an abnormally thickened, short, and hypertrophic radiolunate ligament. This aberrant ligament creates a dense fibrous tether between the volar-ulnar metaphysis of the radius and the lunate, compressing the volar-ulnar physis and exacerbating the asymmetric growth arrest.
The Vickers and Nielsen technique for the resection of a dyschondrosteosis lesion is a highly specialized, joint-preserving procedure designed for skeletally immature patients. By performing a precise physiolysis (resection of the bony bar), excising the tethering Vickers ligament, and interposing a fat graft, the surgeon can restore the growth potential of the distal radius and prevent the progression of the Madelung deformity.
PATHOANATOMY AND BIOMECHANICS
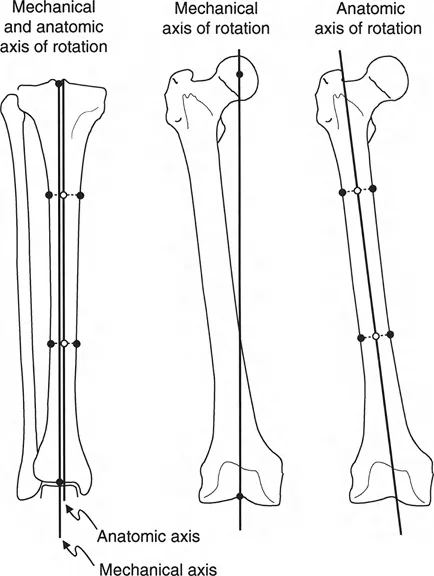
Understanding the biomechanical forces at play is essential for executing this procedure successfully. The normal distal radius physis grows symmetrically, maintaining a neutral to slight volar tilt and a standard radial inclination. In dyschondrosteosis, the Vickers ligament acts as a rigid volar-ulnar tether.
As the dorsal and radial aspects of the physis continue to grow, the tethered volar-ulnar corner acts as a hinge. This results in:
* Volar and Ulnar Angulation: The articular surface of the radius tilts progressively volar and ulnar.
* Carpal Subsidence: The lunate, tethered by the Vickers ligament, subsides proximally into the widened radioulnar space, creating a V-shaped carpal configuration.
* Ulnar Impaction: The distal ulna, unaffected by the radial growth arrest, continues to grow, resulting in positive ulnar variance and dorsal prominence.
💡 Clinical Pearl
The Vickers ligament is not merely a thickened capsule; it is a distinct, anomalous structure that often contains cartilaginous elements. It originates proximal to the physis on the radial metaphysis and inserts onto the lunate, crossing and compressing the physis. Failure to completely excise this ligament will result in recurrent deformity despite adequate bony bar resection.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Skeletally Immature Patients: The primary indication is a growing child (typically girls aged 8 to 12 years) with documented Léri-Weill dyschondrosteosis or idiopathic Madelung deformity.
- Progressive Deformity: Serial radiographs demonstrating worsening volar tilt, radial inclination, or carpal subsidence.
- Symptomatic Presentation: Pain at the volar-ulnar wrist or distal radioulnar joint (DRUJ), accompanied by a decreasing range of motion (specifically supination and wrist extension).
- Visible Physeal Bar: MRI or CT evidence of a localized volar-ulnar physeal bridge comprising less than 50% of the total physeal cross-sectional area.
Contraindications
- Skeletal Maturity: Patients with closed physes will not benefit from physiolysis. These patients require corrective osteotomies (e.g., Ranawat reconstruction or dome osteotomies).
- Extensive Physeal Arrest: If the bony bar involves more than 50% of the physis, resection is unlikely to restore symmetric growth, and an epiphysiodesis with corrective osteotomy is preferred.
- Advanced Degenerative Changes: Established radiocarpal or DRUJ osteoarthritis.
PREOPERATIVE PLANNING
Meticulous preoperative imaging is mandatory. Standard posteroanterior (PA) and lateral radiographs of the wrist will demonstrate the classic features of Madelung deformity. However, advanced imaging is required for surgical templating.
- Magnetic Resonance Imaging (MRI): MRI is the gold standard for identifying the Vickers ligament and mapping the exact location and extent of the cartilaginous/bony physeal bar.
- Computed Tomography (CT): A 3D CT scan with sagittal and coronal reconstructions is invaluable for mapping the bony bridge and planning the precise location of the osteotomy cuts.
SURGICAL TECHNIQUE: VICKERS AND NIELSEN
1. Patient Positioning and Setup
- Place the patient supine with the operative arm extended on a radiolucent hand table.
- Apply a well-padded pneumatic tourniquet to the proximal arm.
- Administer prophylactic intravenous antibiotics prior to tourniquet inflation.
- Exsanguinate the limb using an Esmarch bandage and inflate the tourniquet to 250 mm Hg (or appropriate pediatric pressure).
- Magnification is highly recommended. The use of 2.5x to 3.5x surgical loupes or an operating microscope is critical for distinguishing between the healthy physeal cartilage and the pathological bony bar.
2. Surgical Approach and Exposure
Make a volar transverse incision approximately 1.5 cm proximal to the most proximal wrist crease. The incision can pass either on the ulnar side of the flexor carpi radialis (FCR) and palmaris longus (PL) or on the radial side, depending on the surgeon's preference and the severity of the deformity.
⚠️ Surgical Warning
Extreme caution must be exercised to protect the palmar cutaneous branch of the median nerve, the median nerve itself, and the radial artery. The distorted anatomy in Madelung deformity often displaces these neurovascular structures from their standard anatomical beds.
Continue the deep dissection radial to the mass of the digital flexor tendons. Retract the flexor tendons ulnarward to expose the distal edge of the pronator quadratus muscle. Mobilize the radial end of the pronator quadratus and reflect it ulnarward to expose the volar metaphysis of the distal radius.
3. Identification of the Vickers Ligament
Once the pronator quadratus is reflected, inspect the volar-ulnar aspect of the radius. The Vickers ligament will appear as a thick, white, fibrous band originating from the volar metaphysis, crossing the physis, and inserting deep into the carpus (specifically the lunate).
Identify the abnormal volar ligament tethering the lunate to the radius. Carefully isolate this structure. In patients with extreme volar subluxation of the carpus, the lunate may be severely displaced proximally; take absolute care not to mistake the subluxated lunate for the underlying distal radius metaphysis.

4. Osteotomy and Exposure of the Physis
Using a fine, sharp osteotome, make the initial longitudinal osteotomy in the radius. This cut should be parallel to the long axis of the forearm and positioned approximately 5 mm from the radioulnar joint.
Reflect the small, 5-mm fragment of the distal radius ulnarward using the osteotome. The goal here is to preserve what exists of the flimsy, attenuated connections between this fragment and the ulna, thereby leaving some critical soft-tissue support for the lunate and the DRUJ.
Once this fragment is reflected, a sagittal section of the distal radius should be clearly visible.
5. Physiolysis and Bar Resection
If the initial osteotomy is too shallow, you will observe a white sheet of fibrous tissue and cartilage. You must proceed deeper to locate the true physis.
Make successive, highly controlled osteotomy cuts, exactly 1 mm thick, moving radially and dorsally until the physis is clearly identified. When first visualized, the healthy physis will appear thin, wavy, and significantly narrowed compared to a normal growth plate.
Once the physeal cartilage is clearly defined, carefully remove the pathological bone from the metaphyseal side. This is best achieved using a fine gouge or a high-speed diamond burr under continuous saline irrigation to prevent thermal necrosis.
💡 Clinical Pearl
The resection must be meticulous. Remove bone so that the profile of the healthy cartilage sits above the surrounding bone. The cartilage must be left completely intact from the dorsal periosteum to the volar periosteum. Leaving any residual bony bridge will inevitably lead to a recurrent tether and failure of the procedure.

6. Excision of the Vickers Ligament
With the bony bar resected, return your attention to the Vickers ligament. Excise this abnormal tether completely from its metaphyseal origin to its insertion on the lunate. Ensure that the lunate is completely freed from its volar tether to the radius, allowing the carpus the potential to remodel and translate dorsally as the radius grows.
7. Hemostasis and Preparation for Grafting
Deflate the pneumatic tourniquet. Obtain meticulous hemostasis using bipolar electrocautery. If there is persistent osseous bleeding from the metaphyseal bone, apply a minimal amount of bone wax, though this should be used sparingly to avoid foreign body reactions that might impede fat graft vascularization.
Reinflate the tourniquet once hemostasis is achieved. Flush the surgical cavity copiously with normal saline to remove all microscopic bone chips, dust from the burr, and residual blood clots. Any remaining osteogenic material can serve as a nidus for recurrent bar formation.
8. Fat Graft Interposition (Langenskiöld Principle)
To prevent the reformation of the bony bar across the resected physis, an interpositional material must be placed. Autologous fat is the gold standard.
Obtain a generous quantity of subcutaneous fat from the proximal forearm medially (often through a separate small incision or an extension of the primary incision).
Insert the fat graft to fill the surgical cavity completely. This fat must make intimate, gap-free contact with the entire length of the exposed physeal cartilage, effectively isolating the bony epiphysis from the bony metaphysis. The surrounding soft tissues and the reflected pronator quadratus will naturally fall together to hold the fat graft securely in place.
9. Closure
Allow the pronator quadratus to rest over the operative site. Suture the subcutaneous tissues with absorbable sutures and close the skin with a subcuticular stitch or interrupted non-absorbable sutures. Apply a sterile dressing.
ADJUNCTIVE PROCEDURES: RANAWAT RECONSTRUCTION
While the Vickers and Nielsen technique is ideal for skeletally immature patients, patients who present late with closed physes and severe deformity require a different approach. The Ranawat et al. reconstruction is a powerful salvage procedure for mature Madelung deformity.
This procedure involves a dorsal-based and radial-based closing wedge osteotomy of the distal radius to correct the volar tilt and radial inclination. This is performed in conjunction with a Darrach procedure (excision of the distal ulna) to address the severe positive ulnar variance and DRUJ incongruity.
Correct alignment is obtained under fluoroscopic guidance, and rigid internal fixation is achieved using a specialized volar or dorsal plate and screws.

POSTOPERATIVE CARE AND REHABILITATION
Immobilization Phase (Weeks 0-2)
- Immediately postoperatively, apply a short arm volar slab or a bulky crepe bandage, depending on the degree of the preoperative deformity and the stability of the fat graft.
- The wrist is immobilized in a neutral position.
- The bandage or splint should be worn continuously for 2 weeks.
- Strict elevation of the limb is required for the first 48 to 72 hours to minimize edema and prevent compartment syndrome.
- Immediate active range of motion of the fingers, thumb, elbow, and shoulder is encouraged to prevent stiffness and promote venous return.
Mobilization Phase (Weeks 2-6)
- At the 2-week postoperative mark, the splint and skin sutures are removed.
- The patient is transitioned to a removable thermoplastic wrist splint, to be worn during high-risk activities and at night.
- Supervised hand therapy is initiated. The focus is on restoring active and passive range of motion of the wrist, with particular emphasis on supination and wrist extension, which are typically the most restricted motions in Madelung deformity.
Long-Term Follow-Up
- Patients must be followed clinically and radiographically every 6 months until skeletal maturity.
- Serial radiographs are evaluated to confirm the resumption of symmetric physeal growth, the absence of recurrent bar formation, and the gradual remodeling of the carpal alignment.
- If a recurrent tether is identified early, revision physiolysis may be considered, though the success rate decreases with subsequent interventions.
COMPLICATIONS AND PITFALLS
- Recurrent Deformity: The most common complication is the reformation of the physeal bar. This is usually due to incomplete initial resection, failure to remove all bone dust, or inadequate fat graft interposition.
- Incomplete Ligament Release: Failure to completely excise the Vickers ligament will leave a persistent soft-tissue tether, preventing carpal remodeling even if the bony bar is successfully resected.
- Nerve Injury: The palmar cutaneous branch of the median nerve is at high risk during the volar transverse incision. Neuroma formation here can lead to debilitating chronic pain.
- DRUJ Instability: Over-resection of the 5-mm ulnar fragment of the radius can destroy the remaining radioulnar ligaments, leading to gross instability of the distal radioulnar joint.
- Thermal Necrosis: Using a high-speed burr without adequate saline irrigation can cause thermal necrosis of the adjacent healthy physeal cartilage, paradoxically worsening the growth arrest.
You Might Also Like