Comprehensive Surgical Management of Pediatric Hand Anomalies: Congenital Trigger Digits and Camptodactyly
Key Takeaway
Congenital trigger digits and camptodactyly present unique reconstructive challenges in pediatric orthopedics. While trigger thumbs often require simple A1 pulley release, trigger fingers and camptodactyly demand complex exploration of the flexor-extensor mechanism. This comprehensive guide details the pathoanatomy, biomechanical principles, and step-by-step surgical techniques—including FDS slip excision and comprehensive volar releases—necessary to restore optimal digital kinematics and prevent permanent flexion contractures in the growing hand.
INTRODUCTION TO MISCELLANEOUS PEDIATRIC HAND ANOMALIES
The pediatric hand is a complex biomechanical marvel, and congenital anomalies disrupting its delicate flexor-extensor balance require meticulous evaluation and precise surgical intervention. Among the miscellaneous anomalies encountered by the orthopedic hand surgeon, congenital trigger digits and camptodactyly represent two distinct pathophysiological entities. While both present with flexion deformities, their underlying pathoanatomy, natural history, and surgical management differ profoundly.
This masterclass provides an exhaustive, evidence-based review of these conditions, tailored for the practicing consultant, fellow, and resident. It details the biomechanical principles, step-by-step surgical techniques, and postoperative rehabilitation protocols necessary to achieve optimal functional outcomes.
CONGENITAL TRIGGER DIGITS
Congenital trigger digit occurs when the normal, frictionless gliding movement of the flexor tendon is mechanically impeded within the digital flexor sheath.
Pathophysiology and Biomechanics
In stark contrast to adult stenosing tenovaginitis—which is characterized by active "triggering" or snapping—the congenitally involved pediatric digit typically presents with a persistent, fixed flexion deformity.
This is a relatively rare condition, accounting for approximately 2.3% of congenital hand anomalies. It exhibits a overwhelming predilection for the thumb (congenital trigger thumb) and presents bilaterally in about 25% of patients. The condition occurs sporadically and is generally not considered an inherited trait, though isolated reports have noted associations with trisomy 13 and mucopolysaccharidosis (as described by Van Heest).
The pathological anatomy responsible for congenital trigger digits includes:
1. Sheath Hypertrophy: Narrowing and fibrotic thickening of the A1 pulley.
2. Notta's Nodule: An intratendinous nodule (often palpable) located within the flexor pollicis longus (FPL) or flexor digitorum profundus (FDP) tendon, just proximal to the first annular pulley.
3. Cystic Formation: Occasional formation of an adventitial ganglion cyst.
4. Chronic Inflammation: Histological evidence of chronic tenosynovitis.
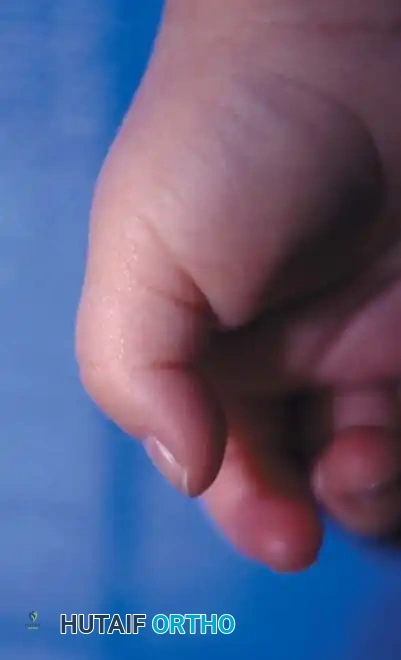
Clinical presentation of a congenital trigger thumb in a 2-year-old child, demonstrating the characteristic fixed flexion posture of the interphalangeal (IP) joint.
Clinical Evaluation and Natural History
Prospective studies of over 5,765 newborns have failed to reveal a single case of congenital trigger thumb at birth, supporting the consensus that the condition is more accurately described as acquired in infancy. It is frequently unnoticed until the child reaches 1 to 2 years of age, presenting as a relatively fixed flexion posture of the interphalangeal (IP) joint.
CLINICAL PEARL:
Congenital trigger thumb must be meticulously differentiated from a clasped thumb deformity. In a clasped thumb, the primary pathology is metacarpophalangeal (MCP) flexion due to extensor hypoplasia or absence, whereas a trigger thumb presents with isolated IP joint flexion and a palpable volar nodule.
Even with passive force, full extension of the IP joint may be impossible. The abnormal clicking or snapping that is the hallmark of adult trigger digits is rarely the presenting complaint in children.
Natural History:
Spontaneous resolution is well-documented. It occurs in approximately 30% of children whose condition appears within the first year of life, and in about 12% of children presenting between 6 months and 2 years of age. Fixed joint contractures are highly unlikely if the condition resolves spontaneously or is surgically corrected before the child reaches 3 years of age.
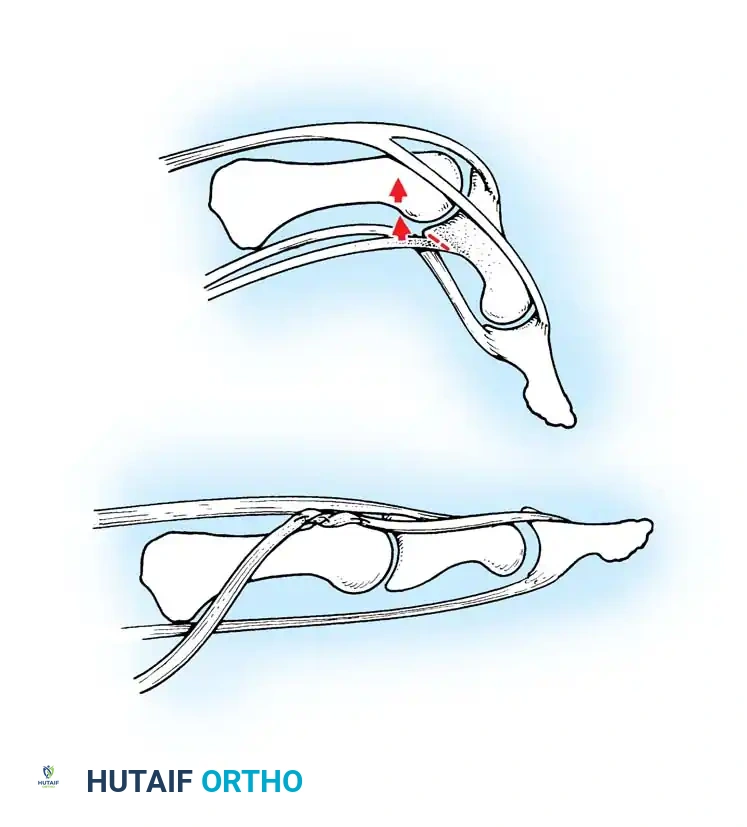
Anatomical diagram illustrating the mismatch between the hypertrophied intratendinous nodule and the stenotic A1 pulley.
Trigger Finger vs. Trigger Thumb
A critical distinction must be made between congenital trigger fingers and trigger thumbs. Trigger fingers are less likely to present with a fixed flexion deformity. More importantly, they frequently do not respond to a simple A1 pulley release.
When surgical intervention for a trigger finger is undertaken, the surgeon must be prepared for a comprehensive exploration of the flexor mechanism. The pathology often extends beyond the A1 pulley, involving abnormal decussations of the flexor digitorum superficialis (FDS) or stenosis at the A3 pulley.

Intraoperative visualization of the flexor tendon sheath, highlighting the critical relationship between the A1 and A2 pulleys.
Indications for Treatment
Because spontaneous resolution can be expected in nearly a third of infants presenting before age 1, initial management should consist of observation and gentle passive manipulation. Splinting in extension has been reported to yield a success rate of up to 66% in compliant patients.
Surgical Indications:
* Failure of spontaneous resolution or conservative management by age 2 to 3 years.
* Multiple trigger digits fixed in extension that prevent the child from making a fist (warrants earlier intervention, around 1 year of age).
* Progressive fixed flexion contracture of the IP joint.
SURGICAL WARNING:
Percutaneous trigger thumb release in children has been reported; however, due to the extreme proximity of the radial digital nerve (which crosses obliquely over the flexor sheath in the thumb), percutaneous release is strictly not recommended in pediatric patients. Open release under direct vision is the gold standard.
TECHNIQUE 76-51: Release of a Congenital Trigger Thumb
This procedure aims to restore normal FPL excursion while meticulously protecting the neurovascular bundles.
- Positioning and Preparation: Place the patient supine with the arm extended on a hand table. Apply a pediatric pneumatic tourniquet to the upper arm. Use loupe magnification.
- Incision: Make a transverse incision (approximately 1.5 cm) directly within the volar flexion crease of the metacarpophalangeal (MCP) joint of the thumb.
- Dissection: Perform blunt dissection through the subcutaneous fat. The flexor sheath is usually quite prominent and superficial in toddlers.
- Nerve Protection: Identify and carefully retract the radial and ulnar digital nerves. The radial digital nerve is particularly vulnerable as it courses obliquely across the operative field.
- Pulley Release: Identify the proximal edge of the first annular (A1) pulley. Using a scalpel or fine tenotomy scissors, completely incise the A1 pulley longitudinally under direct vision.
- Verification: Passively flex and extend the IP joint. Ensure the Notta's nodule glides smoothly without impingement.
- Note: Shaving the intratendinous nodule or excising a segment of the A1 pulley is unnecessary and contraindicated, as it risks tendon rupture or bowstringing.
- Closure: Deflate the tourniquet, achieve hemostasis, and close the skin with absorbable sutures (e.g., 5-0 chromic gut). Apply a soft, bulky hand dressing. No rigid immobilization is required.

Postoperative clinical appearance following successful A1 pulley release, demonstrating full, unrestricted extension of the thumb IP joint.
Diagrammatic representation of the A1 pulley release, ensuring the A2 pulley remains intact to prevent bowstringing.
TECHNIQUE 76-52: Release of a Congenital Trigger Finger
Surgical management of a trigger finger requires a more extensile approach due to the high likelihood of complex FDS/FDP interactions.
- Incision: Make a volar zigzag (Bruner) incision centered over the A1 pulley to allow for both proximal and distal exposure of the flexor tendon sheath and its contents.
- Exposure: Elevate the skin flaps, taking care to identify and protect the digital neurovascular bundles bilaterally.
- A1 Pulley Release: Incise the A1 pulley completely from its proximal to distal extent.
- Dynamic Assessment: Passively flex and extend the digit. Inspect the motion of the flexor tendons. If normal gliding of the FDS and FDP is present and triggering has resolved, proceed to closure.
- Extended Exploration (If Triggering Persists):
- Inspect the FDS tendon for a more proximal-than-normal decussation (chiasm of Camper) or an abnormal insertion into the FDP tendon.
- If an abnormal FDS slip is tethering the FDP, excise one or both slips of the FDS tendon to decompress the sheath.
- Inspect the A3 pulley. If triggering occurs at this level, carefully release the A3 pulley, ensuring the A2 and A4 pulleys remain strictly intact.
- Final Verification: Apply proximal traction to both flexor tendons together and individually in the palm, and passively extend the finger to verify complete resolution of triggering.
- Closure: Close the skin with absorbable sutures and apply a soft hand dressing.

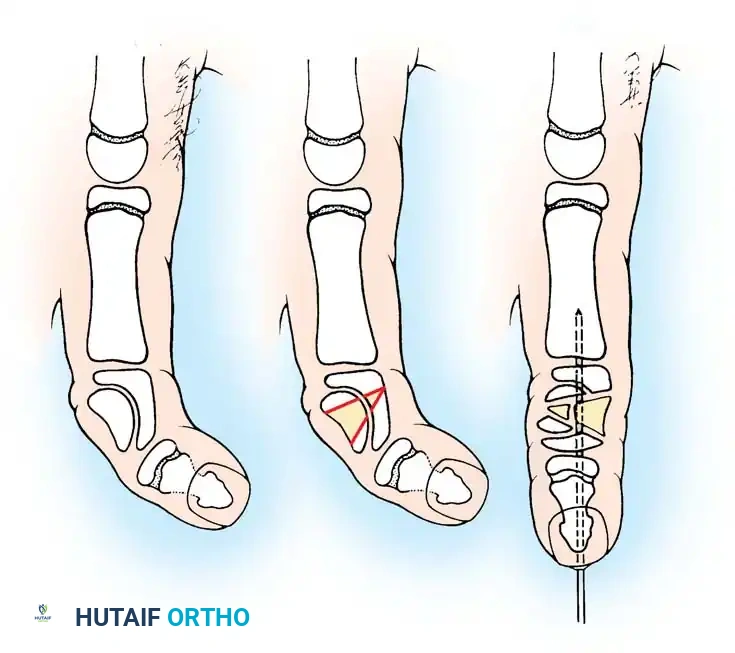
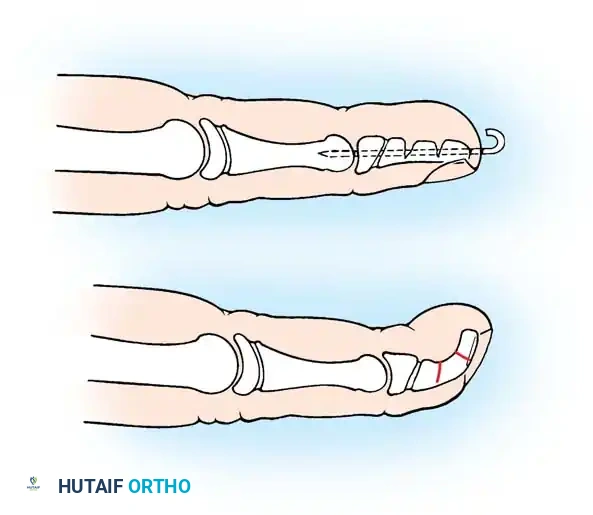
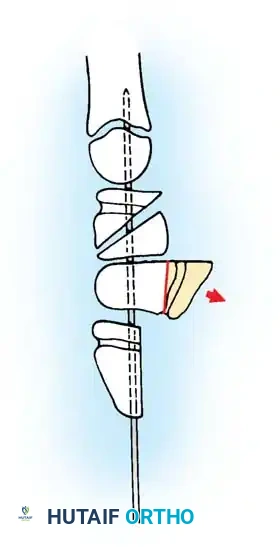
Intraoperative view demonstrating the excision of an abnormal FDS slip to relieve persistent triggering after A1 release.
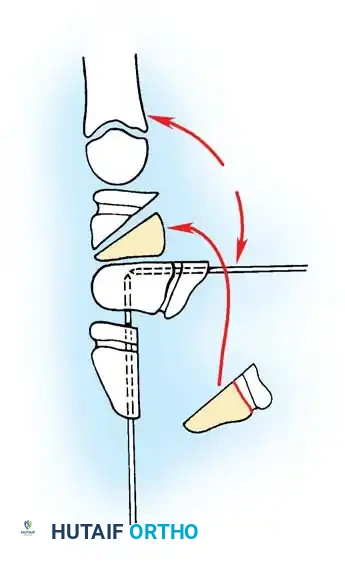
Biomechanical illustration showing the relationship of the FDS and FDP tendons within the digital sheath.
CAMPTODACTYLY
Camptodactyly (from the Greek kamptos meaning bent, and daktylos meaning finger) is a non-traumatic, progressive flexion deformity of the proximal interphalangeal (PIP) joint. It predominantly involves the little finger.
Pathoanatomy and Etiology
This condition must be distinguished from clinodactyly, which is a radioulnar deviation of the digit (usually at the distal interphalangeal joint). Camptodactyly occurs in less than 1% of the general population but accounts for nearly 6.9% of congenital hand anomalies.
The etiology is multifactorial, and virtually every anatomical structure crossing the volar aspect of the PIP joint has been implicated:
* Fascial Bands: Kilgore and Graham identified stout, abnormal fascial bands associated with the Landsmeer (retinacular) ligament.
* Lumbrical Anomalies: McFarlane, Curry, and Evans found abnormal insertions of the lumbrical tendon into the FDS tendon, the MCP joint capsule, or the adjacent extensor expansion in 100% of their operative cases.
* Flexor/Extensor Imbalance: Millesi proposed that the deformity arises from a relative dynamic imbalance between the flexors and extensors.
* FDS Shortening: Smith and Kaplan suggested a relative shortening of the FDS muscle-tendon unit. This is supported clinically when the PIP flexion deformity corrects upon simultaneous flexion of the wrist.
* Other Factors: Contractures of the volar plate, accessory collateral ligaments, and insufficient palmar skin.

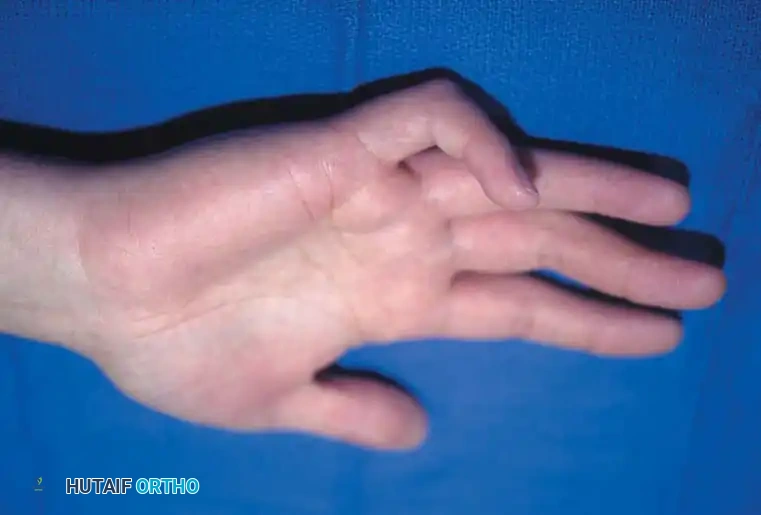
Clinical photograph of classic camptodactyly, demonstrating an isolated flexion deformity of the proximal interphalangeal joint of the little finger.
Classification and Syndromic Associations
Camptodactyly is generally divided into two distinct demographic types:
1. Type I (Infantile): Occurs in infancy, affects both sexes equally, and constitutes about 80% of cases.
2. Type II (Adolescent): Presents during the adolescent growth spurt and predominantly affects females.
A severe subgroup described by Koman, Toby, and Poehling involves severe PIP flexion deformities present at birth, often affecting multiple digits without a predilection for the small finger. This subtype is heavily driven by extensor mechanism pathology (attenuation of the central slip, palmar subluxation of lateral bands).
Camptodactyly is also frequently associated with systemic syndromes, including Trisomy 13, Oculodentodigital syndrome, Orofaciodigital syndrome, Aarskog syndrome, and Cerebrohepatorenal syndrome.
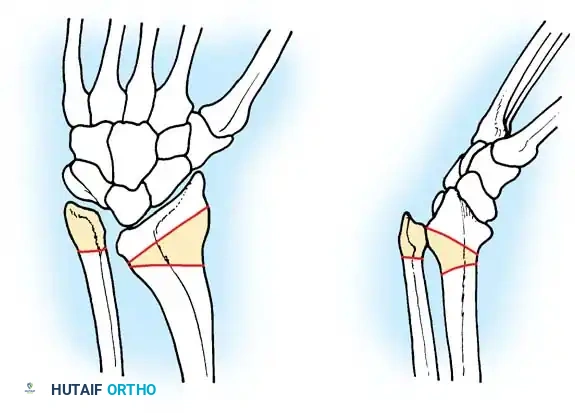
Radiographic evaluation of camptodactyly. Note the absence of primary osseous dysplasia in early stages, though secondary joint remodeling may occur in long-standing cases.
Clinical Evaluation
Most patients present during the first year of life. Approximately two-thirds have bilateral involvement, though severity is often asymmetrical.
The classic posture includes PIP joint flexion with compensatory MCP joint hyperextension. Rotational deformities may cause mild overlapping of the fingers.
DIAGNOSTIC PEARL (The Wrist Flexion Test):
Evaluate the PIP joint while passively flexing and extending the wrist. In young children with a shortened FDS, the PIP deformity will disappear or significantly improve when the wrist is flexed. In older children, the deformity usually becomes fixed due to secondary volar plate and collateral ligament contractures.
If left untreated, 80% of cases worsen, particularly during periods of rapid skeletal growth. Progression typically halts after skeletal maturity (age 18 to 20 years).
Camptodactyly with a severe flexion deformity of 80 degrees when the wrist is held in extension.

The same patient demonstrating improvement of the deformity to 40 degrees upon passive wrist flexion, indicating a tight FDS unit.
Management Strategy
Treatment of camptodactyly is notoriously unpredictable. Engber and Flatt reported that only 20% of patients improved with nonoperative treatment, and only 35% improved with operative treatment.
Nonoperative Management:
For mild, non-progressive deformities (<30 degrees), observation is appropriate. Dynamic extension splinting can be highly effective if initiated early. Miura reported excellent results with full-time dynamic splinting until full extension was achieved, followed by nighttime splinting. However, rebound contractures are common upon discontinuation.
Operative Indications:
* Progressive deformity >40 degrees interfering with function.
* Young children whose deformity corrects with wrist flexion (indicates isolated FDS tightness amenable to simple release).
* Older children with fixed deformities requiring complex structural release.
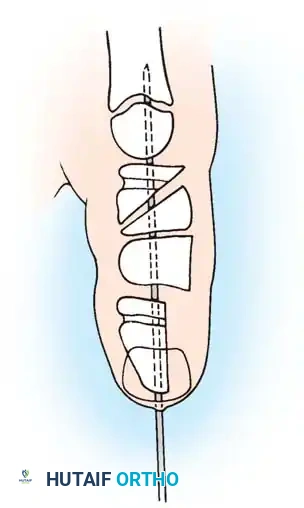
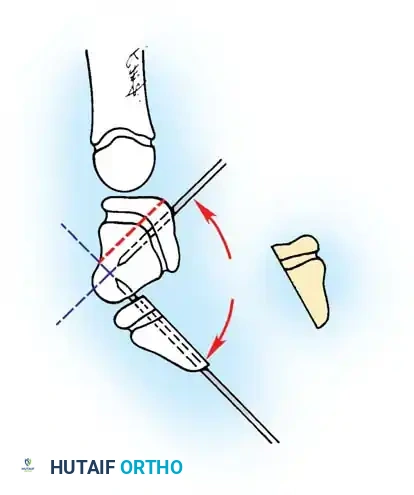
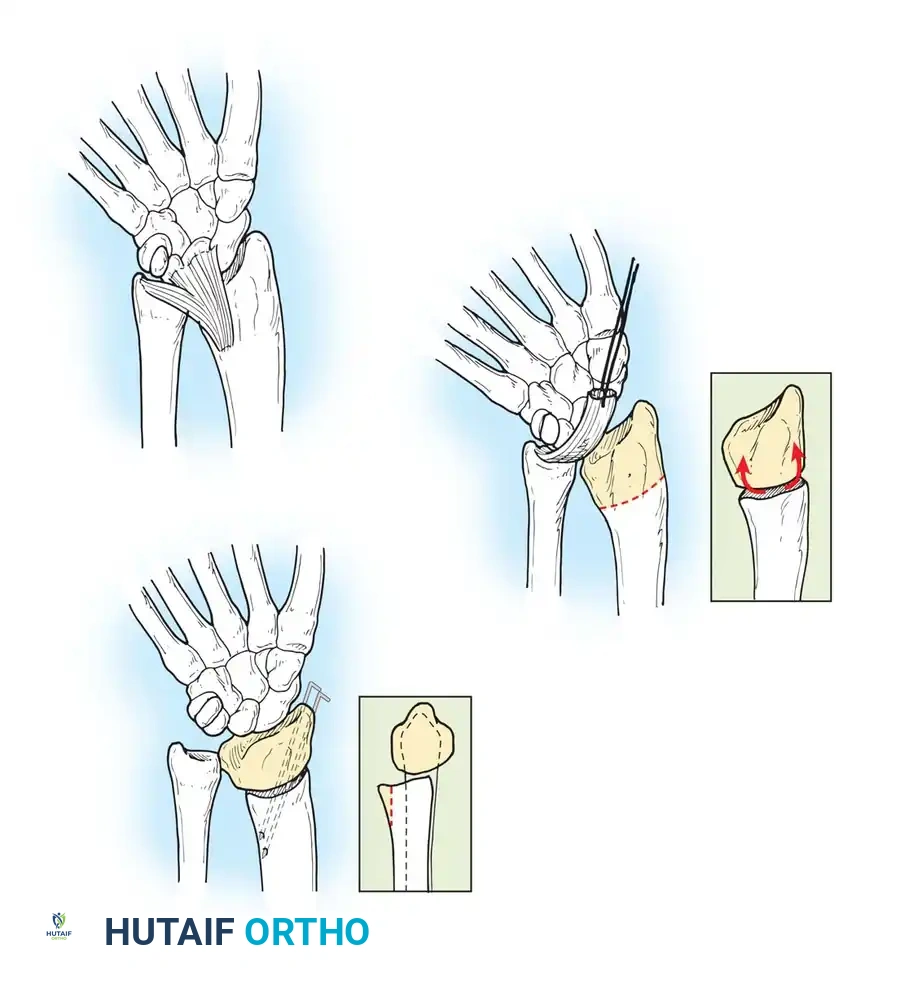
Preoperative planning diagram for a comprehensive volar release, highlighting the structures contributing to the flexion contracture.
TECHNIQUE 76-53: Comprehensive Tendon Release (Smith's Approach)
Smith emphasized a "unifying theory" of camptodactyly, advocating that all abnormal structures must be systematically addressed. The frequency of involvement includes skin (100%), FDS (66%), retinaculum cutis (55%), and lumbricals (22%).
- Incision and Skin Lengthening:
Make a volar linear incision over the affected digit and convert it to multiple Z-plasties. Ensure the central limbs of the Z-plasties are placed precisely over the flexion creases of the joints to prevent secondary scar contracture.






You Might Also Like