Surgical Management of Group 3 Clasped Thumb Deformity and Brachymetacarpia
Key Takeaway
Group 3 clasped thumb deformity represents a complex congenital anomaly characterized by deficient extensor tendons, severe first web space contracture, and metacarpophalangeal joint instability. Surgical reconstruction requires a multifaceted approach, including extensor indicis proprius transfer, palmaris longus abductorplasty, and joint stabilization. This comprehensive guide details the modified Neviaser technique, alongside advanced lengthening protocols for brachymetacarpia and hypoplastic digits, providing orthopedic surgeons with evidence-based strategies for optimizing functional and aesthetic outcomes.
INTRODUCTION TO CONGENITAL THUMB AND HAND HYPOPLASIA
Congenital anomalies of the hand present a formidable challenge to the reconstructive orthopedic surgeon, requiring a profound understanding of pediatric biomechanics, physeal growth patterns, and soft-tissue envelope management. Among these anomalies, the Group 3 Clasped Thumb Deformity and varying degrees of Brachymetacarpia represent distinct but functionally limiting conditions.
The clasped thumb deformity is characterized by a thumb that is flexed and adducted into the palm. According to the Tsuyuguchi classification, Group 3 is the most severe form, defined by a combination of absent or severely hypoplastic extensor tendons, profound first web space contracture, and collateral ligament laxity leading to metacarpophalangeal (MCP) joint instability.
Conversely, hypoplasia of the hand and digits—ranging from simple brachymetacarpia to severe syndromic manifestations—requires a highly individualized approach. This masterclass delineates the evidence-based surgical protocols for reconstructing the Group 3 clasped thumb using the modified Neviaser technique, as well as contemporary strategies for managing brachymetacarpia and severe digital hypoplasia.
GROUP 3 CLASPED THUMB DEFORMITY: THE MODIFIED NEVIASER TECHNIQUE
The modified Neviaser technique is a comprehensive, multi-stage reconstructive procedure designed to address the triad of deficits in a Group 3 clasped thumb: MCP joint instability, extensor tendon deficiency, and adduction contracture.
Preoperative Planning and Positioning
Surgical intervention is typically delayed until the child is of sufficient size to allow for meticulous tendon transfer and joint reconstruction, often between 2 to 4 years of age, though earlier intervention may be indicated for severe, rigid contractures.
- Anesthesia: General anesthesia with a well-padded pediatric tourniquet applied to the proximal arm.
- Positioning: Supine with the operative extremity extended on a radiolucent hand table.
- Preparation: Standard sterile prep and drape, ensuring the entire forearm and hand are exposed to facilitate tendon harvesting and routing.
Step 1: Metacarpophalangeal Joint Stabilization (Chondrodesis)
In Group 3 deformities, the MCP joint is frequently unstable to both radial and ulnar stresses due to profound collateral ligament incompetence. Arthrodesis in a pediatric patient must be modified to a "chondrodesis" to preserve the proximal phalangeal physis.
- Incision: Make a longitudinal or lazy-S dorsal incision over the thumb MCP and interphalangeal (IP) joints.
- Exposure: Perform a dorsal capsulotomy to expose the articular surfaces of the first metacarpal head and the base of the proximal phalanx.
- Cartilage Resection: Using a fine scalpel (e.g., a #15 blade), meticulously shave the articular cartilage from both surfaces.
> Surgical Warning: It is imperative to shave only the cartilage to expose the underlying epiphyseal bone. Aggressive resection with an oscillating saw or rongeur will irreversibly damage the physis, leading to premature growth arrest. - Fixation: Reduce the MCP joint in approximately 15 degrees of flexion and neutral radioulnar deviation. Pin the joint transarticularly with a smooth 0.035-inch or 0.045-inch Kirschner wire (K-wire), ensuring the wire does not repeatedly traverse the physis to minimize thermal and mechanical trauma.
Step 2: Extensor Indicis Proprius (EIP) Transfer
To restore active extension to the thumb, the Extensor Indicis Proprius (EIP) is harvested and transferred to the distal phalanx.
- Harvesting the EIP: Make a short transverse dorsal incision at the base of the index finger (over the MCP joint) to identify the EIP tendon, which lies ulnar to the Extensor Digitorum Communis (EDC) tendon.
- Proximal Release: Make a second transverse dorsal incision over the wrist, in line with the EIP tendon. Divide the EIP tendon distally at the index MCP joint, repair the extensor hood to prevent extensor lag of the index finger, and deliver the EIP tendon into the proximal wrist wound.
- Rerouting: Create a wide subcutaneous tunnel from the wrist incision to the dorsal thumb incision. Reroute the EIP tendon through this tunnel.
- Insertion: Suture the EIP tendon into the soft tissue and periosteum around the base of the distal phalanx. Alternatively, elevate a small periosteal flap at the base of the distal phalanx, weave the tendon beneath it, and secure it with non-absorbable sutures (e.g., 4-0 Ethibond). Tension the transfer with the wrist in neutral and the thumb in full extension.
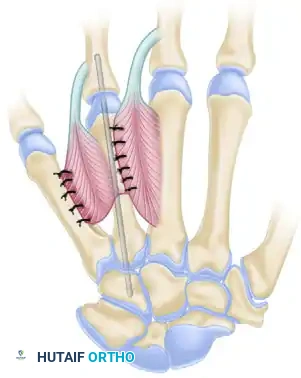
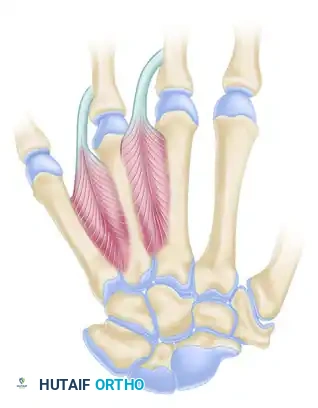
Step 3: Palmaris Longus (PL) Abductorplasty
To counteract the adduction forces and restore palmar abduction, the Palmaris Longus is transferred to the base of the proximal phalanx.
- Harvesting the PL: Make a short transverse palmar incision at the wrist crease over the PL tendon. Divide the tendon at its insertion into the palmar fascia.
- Tunnel Creation: Route the PL tendon subcutaneously toward the radial aspect of the thumb MCP joint.
- Osseous Fixation: Create a small osseous tunnel at the base of the thumb proximal phalanx, strictly distal to the epiphysis to avoid physeal injury.
- Securing the Transfer: Pass the PL tendon through the osseous tunnel and suture it back onto itself. Tension the transfer to maintain the thumb in wide palmar abduction.
Step 4: Web Space Reconstruction and CMC Derotation
A severe first web space contracture is universally present in Group 3 deformities and must be addressed to allow the tendon transfers to function.
- Z-Plasty: Perform a broad 4-flap or standard Z-plasty reconstruction of the first web space. Release the adductor pollicis fascia and the first dorsal interosseous fascia if necessary.
- Opponensplasty: If true opposition is lacking, a formal opponensplasty (e.g., Huber transfer or FDS ring finger transfer) may be performed concurrently.
- CMC Derotation: If the thumb metacarpal remains internally rotated, sharply incise the capsule of the trapeziometacarpal (CMC) joint. Pronate the thumb metacarpal 90 degrees to place it in a functional position, and fix it temporarily with a transarticular K-wire.
Postoperative Protocol
- Immobilization: Close all incisions in a routine fashion. Apply a well-padded, long-arm thumb spica cast or rigid splint with the thumb in the fully corrected position (abducted and extended).
- Pin Removal: The K-wires stabilizing the MCP and CMC joints are removed in the clinic 6 weeks postoperatively.
- Rehabilitation: Progressive active and active-assisted range of motion is initiated at 6 weeks.
- Splinting: The thumb must be protected in a custom-molded thermoplastic night splint for an additional 3 to 4 weeks to prevent recurrence of the flexion-adduction contracture.
THE HYPOPLASTIC HAND AND BRACHYMETACARPIA
Hypoplasia of the hand and digits encompasses a broad spectrum of congenital anomalies, ranging from simple digital shortening (brachydactyly) to a severely hypoplastic hand possessing only soft-tissue nubbins.
Classification and Syndromic Associations
Currently, there is no universally accepted, surgically useful classification for the globally hypoplastic hand. While geneticists utilize detailed groupings to track inheritance patterns, these rarely dictate surgical management.
Brachymetacarpia (shortening of the metacarpals) is typically noted during the teenage growth spurt. It presents clinically as a depression or "dropped knuckle" of one or more metacarpal heads when the patient makes a clenched fist. The ulnar two digits (ring and little fingers) are most frequently affected.
Clinical Pearl: Unilateral shortening is common. However, when brachymetacarpia of the long, ring, and little fingers is observed bilaterally, it is classified as Brachydactyly Type E (Bell's classification), which is strongly associated with pseudohypoparathyroidism. Other syndromic associations include Turner syndrome, Biemond syndrome, and Silver syndrome.
Nonoperative Management
Single-digit shortening, particularly isolated to the little finger, generally requires no surgical intervention. While a single short digit surrounded by normal-length digits may present a cosmetic concern to the patient or parents, the functional limitation is negligible.
Surgical Warning: Attempting to lengthen a single, mildly short digit purely for cosmetic reasons is highly discouraged. The surgical trauma, prolonged immobilization, and altered tendon excursion frequently result in profound digital stiffness, ultimately degrading the function of a previously normal, albeit short, finger.
OPERATIVE TREATMENT OF BRACHYMETACARPIA
Surgical lengthening of the metacarpals is indicated to improve the aesthetic appearance of the metacarpal arch and to optimize grip strength. Shortening of more than 1 cm significantly disrupts the transverse metacarpal arch, leading to altered intrinsic muscle mechanics and decreased grip strength.
Single-Stage Lengthening (The Buck-Gramcko Technique)
For metacarpal shortening of approximately 1 cm or less, a single-stage lengthening procedure utilizing an interpositional bone graft is highly effective. Tajima originally described a V-shaped metacarpal osteotomy, but Buck-Gramcko (1971) refined the technique by emphasizing the critical importance of soft-tissue release.
Step 1: Exposure and Soft Tissue Release
A dorsal longitudinal incision is made over the affected metacarpal. To prevent intrinsic plus deformity and allow for acute lengthening without excessive tension, the interosseous muscles must be carefully elevated, and the deep transverse intermetacarpal ligaments must be detached. A transverse or step-cut osteotomy is then performed at the metacarpal diaphysis.
Step 2: Interposition Grafting and Fixation
Traction is applied to the distal segment to achieve the desired length (maximum ~1 cm). A structural autograft, typically harvested from the iliac crest or distal radius, is contoured to fit the defect. The graft is interposed between the osteotomy ends and rigidly fixed with a longitudinal intramedullary K-wire or a low-profile dorsal plate.
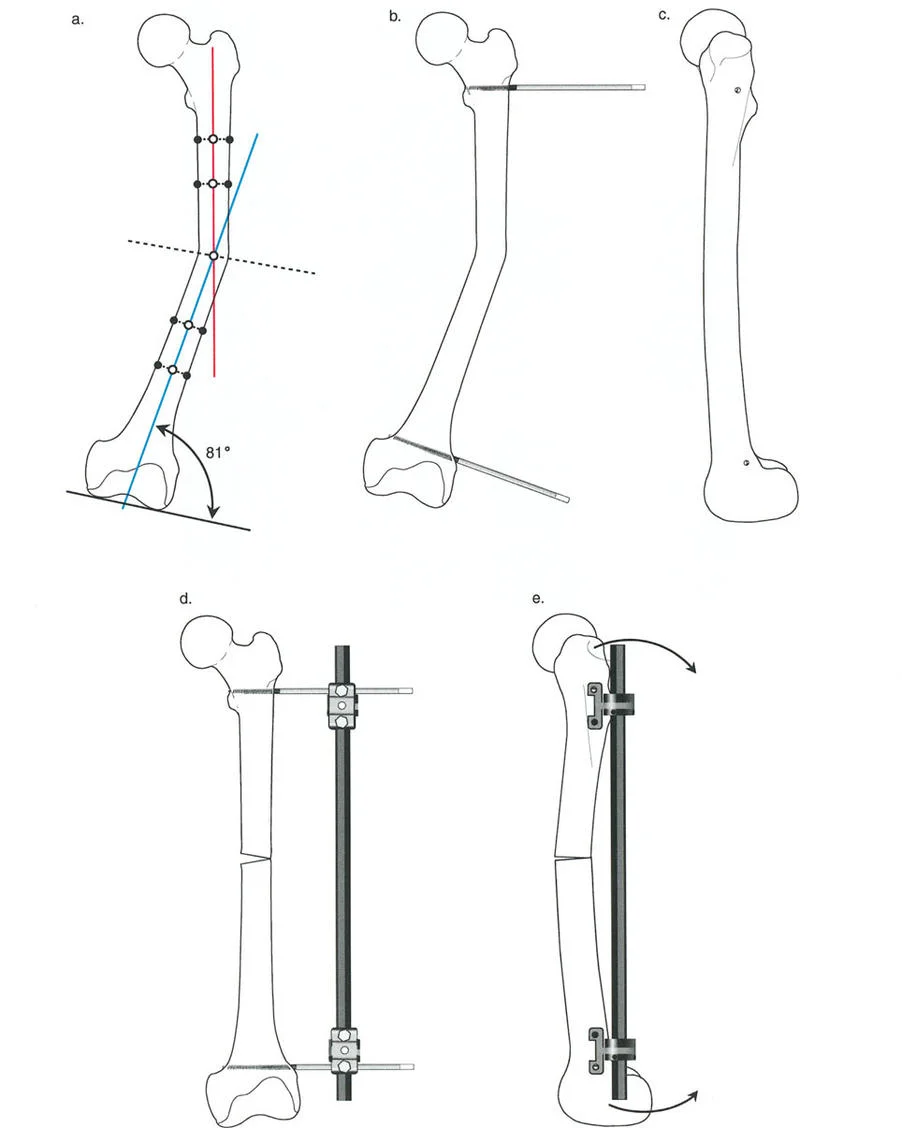
Distraction Osteogenesis (Callotasis)
For shortening exceeding 1 cm, acute lengthening places excessive tension on the neurovascular bundles and extensor tendons. In these cases, gradual callotasis (distraction osteogenesis) is the gold standard.
- Technique: The metacarpal is exposed dorsally, and the periosteum is carefully incised and preserved. An external fixator (e.g., a mini-Ilizarov or monolateral rail) is applied with pins placed proximal and distal to the planned osteotomy site. A low-energy corticotomy is performed.
- Distraction Protocol: After a latency period of 5 to 7 days, distraction is initiated at a rate of approximately 0.5 to 1.0 mm per day, divided into multiple increments.
- Outcomes: Callotasis can reliably achieve 10 to 19 mm (average 15.2 mm) of additional length. Cowen and Loftus reported massive lengthening of the entire palm through the carpometacarpal joints using distal metacarpal and proximal carpal pins, achieving gains of up to 7 cm, though standard gains are 25 to 50 mm.
- Limitations: Lengthening within a single phalangeal segment should be avoided due to the high risk of joint stiffness and pin-tract complications. The shortest bone to which a distraction device can be safely applied is approximately 3 cm.
ADVANCED RECONSTRUCTION FOR SEVERE DIGITAL HYPOPLASIA
Managing a severely hypoplastic hand with no functioning digits, or preservation of only a single digit, is one of the most controversial and technically demanding areas of reconstructive hand surgery.
It is a universally accepted tenet that, excluding non-functional soft-tissue nubbins, any sensate digit, regardless of its size, provides immense functional utility to the patient. However, the musculotendinous structures in these hypoplastic fingers are usually profoundly deficient, exhibiting little to no active excursion.
Nonvascularized Toe-Phalanx Transplantation
For the extremely hypoplastic digit lacking adequate skeletal support, a one-stage, nonvascularized, extraperiosteal toe-phalanx transplantation can be utilized as an interpositional or terminal graft. The primary goal is to provide longitudinal stability and stimulate growth.
Physeal Patency and Growth Potential:
The success of a nonvascularized transfer relies heavily on the survival of the transferred physis. Clinical studies demonstrate a clear age-dependent survival rate for the physis:
* 6 to 18 months of age: 90% physeal patency.
* 18 months to 5 years of age: 67% physeal patency.
* 5 to 13 years of age: 50% physeal patency.
Radiographic measurements indicate that if the physis remains open, the transferred phalanx will achieve an average growth rate of 90% of its expected potential. Radocha et al. reported a mean growth rate of 1 mm per year in 73 children who underwent toe-phalangeal transplantation at or before 1 year of age.
Surgical Approaches:
* Dorsal Approach (Goldberg and Watson): Utilizes a dorsal incision for the insertion of the phalanges, minimizing disruption to the volar flexor apparatus.
* Volar Approach (Toby et al.): Advocates for a volar approach to allow for concurrent identification of the hypoplastic flexor tendon, tenolysis, attachment of the tendon to the phalangeal transfer, and meticulous reconstruction of the volar plate and collateral ligament complex. This approach, while technically more demanding, offers superior restoration of joint kinematics.
Clinical Pearl: If a suitable soft-tissue envelope and adequate proximal bony support are present, phalangeal transfer should be performed before the child reaches 18 months of age. Early intervention maximizes the probability of physeal survival and subsequent longitudinal growth, providing the child with a stable, functional post against which to pinch.
CONCLUSION
The surgical management of congenital hand anomalies requires a delicate balance between aggressive reconstruction and the preservation of existing function. The modified Neviaser technique provides a robust, biomechanically sound solution for the Group 3 clasped thumb, addressing all vectors of the deformity. Similarly, the judicious application of Buck-Gramcko lengthening, distraction osteogenesis, and early toe-phalanx transplantation can dramatically improve the functional capacity and aesthetic appearance of the hypoplastic hand. Mastery of these techniques, coupled with strict adherence to evidence-based indications, is essential for the modern reconstructive orthopedic surgeon.
You Might Also Like