Ulnar Clubhand & Deficiencies: Surgical Management Guide
Key Takeaway
Ulnar clubhand, or paraxial ulnar hemimelia, is a rare congenital longitudinal deficiency of the postaxial upper extremity. Management requires a highly individualized, staged approach. Initial nonoperative serial casting corrects soft tissue contractures, while surgical interventions—such as ulnar anlage excision, syndactyly release, first web space deepening, and metacarpal osteotomies—address progressive radial bowing and optimize prehension. This guide details the biomechanical principles, classifications, and step-by-step operative techniques for managing ulnar deficiencies.
ULNAR CLUBHAND AND LONGITUDINAL ULNAR DEFICIENCIES
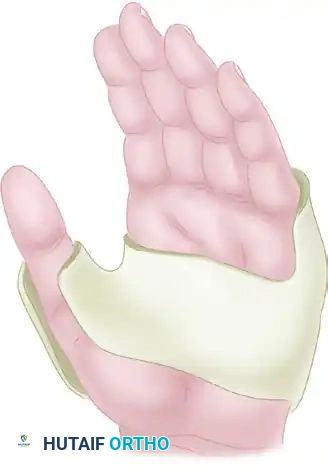
Ulnar deficiencies represent a complex spectrum of malformations characterized by the longitudinal failure of formation along the postaxial (ulnar) border of the upper extremity. The most frequently encountered presentation is a partial deficiency of the ulna combined with the absence of the ulnar two digits, a condition classically referred to as ulnar clubhand. Synonymous nomenclature in the academic literature includes ulnar dysmelia, paraxial ulnar hemimelia, and congenital absence of the ulna.
Epidemiologically, ulnar deficiencies are exceedingly rare congenital hand anomalies. Their relative incidence is estimated to be one-tenth to one-third that of radial deficiencies. The etiology of this rare anomaly remains largely idiopathic, and its occurrence is almost exclusively sporadic. The singular historical report suggesting a familial inheritance pattern was documented by Roberts in 1886, who observed the deformity across three successive generations; however, modern genetic consensus maintains that sporadic mutation is the primary driver.
Pathoanatomy and Associated Anomalies
Varying degrees of deficiency along the ulnar aspect of the hand and forearm are present at birth. The forearm is typically shortened and frequently exhibits pronounced bowing. The small and ring fingers are usually absent, and syndactyly of the remaining digits is a common finding. In approximately two-thirds of patients, the long and index fingers, as well as the thumb, may also be absent.
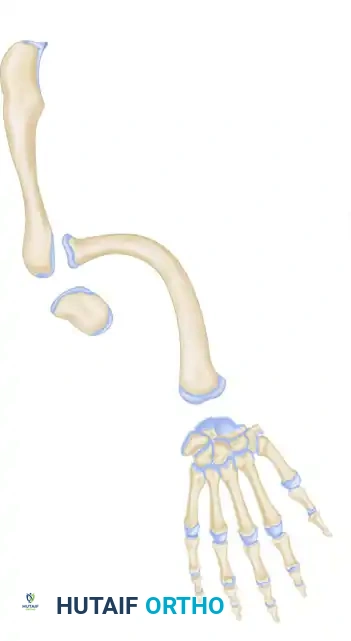
Forearm bowing with radial convexity is primarily driven by the tethering effect of the ulnar anlage—a fibrocartilaginous band representing the undeveloped ulna. Ulnar deviation of the hand strongly correlates with the degree of radial bowing and an increased ulnar slope to the distal radius, which concurrently drives a supination deformity of the forearm. The elbow joint is frequently restricted in its arc of motion and may present with frank humeroradial synostosis.
Clinical Pearl: Anomalies associated with ulnar deficiencies, in stark contrast to radial deficiencies (which frequently present with VACTERL or Holt-Oram syndromes), are almost exclusively limited to the musculoskeletal system. Systemic workups are less likely to yield visceral anomalies, but surgeons must screen for associated musculoskeletal conditions including clubfoot, fibular deficiencies, spina bifida, femoral agenesis, mandibular defects, and congenital absence of the patella.
Carpal bone deformities are ubiquitous due to severe structural deformity and frequent carpal coalition. Digital malformation occurs in up to 89% of patients, and radial head dislocation is a frequent complication of the tethering anlage.
Classification Systems
Accurate classification is paramount for preoperative planning and prognostication. The two most widely utilized systems are the Swanson classification (based on the ulna) and the Cole & Manske classification (based on the thumb and first web space).
Swanson Classification of Ulnar Deficiency
Swanson, Tada, and Yonenobu delineated four primary types of ulnar deficiency based on the morphological absence of the ulna and associated radioulnar joints. A "Type 0" was later proposed by Havenhill et al. to describe a subgroup of patients presenting with an ulnar-deficient ray and carpus but a structurally normal ulna. Notably, partial absence of the ulna is more common than total absence—a direct reversal of the pattern seen in radial deficiencies.
-
Type 1: Hypoplasia or partial defect of the ulna.
-
Type 2: Total defect of the ulna.

-
Type 3: Total or partial defect of the ulna with humeroradial synostosis.

-
Type 4: Total or partial defect of the ulna associated with congenital amputation at the wrist.

Cole & Manske Classification
Cole and Manske classified ulnar-deficient hands based on the functional involvement of the thumb and first web space, recognizing that prehension is the ultimate functional goal. In their seminal series, 73% of ulnar-deficient limbs exhibited thumb and first web abnormalities.
- Type A: Normal first web space and thumb.
- Type B: Mild first web and thumb deficiency.
- Type C: Moderate-to-severe first web and thumb deficiency; potential loss of opposition, malrotation of the thumb into the plane of the other digits, thumb-index syndactyly, and absent extrinsic tendon function.
- Type D: Absent thumb.
Radiographic Evaluation
Standard orthogonal radiographs usually demonstrate a pathognomonic pattern: an absent distal ulna and a bowed radius with an increased ulnar slope along its distal articular surface.

The pisiform and hamate are typically absent, and coalitions of the remaining carpal bones are frequently observed.
Diagnostic Pitfall: It is often difficult to definitively determine the presence or absence of the proximal ulna in neonates, as cartilaginous mineralization may not occur until the child reaches 1 year of age. Serial radiographs or advanced imaging (MRI/Ultrasound) may be required to confirm the presence of a proximal ulnar segment before planning a one-bone forearm reconstruction.
NONOPERATIVE MANAGEMENT
Initial management of ulnar clubhand in infants is strictly nonoperative, focusing on corrective casting and splinting to stretch contracted soft tissues and passively correct the ulnar deviation.
Serial Casting Technique (Riordan Method)
A long-arm cast is applied utilizing the sequential method described by Riordan:
1. Hand Section: Apply the cast to the hand first, molding it carefully to protect the delicate skin.
2. Forearm Integration: Join the hand section to the forearm, holding the wrist in the maximum corrected position (radial deviation and pronation, depending on the deformity).
3. Elbow Integration: Finally, join the forearm to the arm with the elbow flexed at 90 degrees to prevent the cast from slipping and to control forearm rotation.
Frequent cast changes (every 1 to 2 weeks) are necessary to accommodate rapid infant growth and to progressively stretch the soft tissues. Once maximal correction is achieved, custom-fabricated removable thermoplastic splints are utilized to maintain the correction. This nonoperative regimen should be continued diligently until the child is 6 months old, at which point surgical exploration and excision of the ulnar anlage should be considered if significant radial bowing persists.
OPERATIVE MANAGEMENT STRATEGIES
Surgical intervention is highly individualized. Primary indications for surgery include syndactyly, progressive radial bowing secondary to an ulnar anlage, dislocation of the radial head with limited elbow extension, and severe internal rotation deformity of the humerus.
Excision of the Ulnar Anlage
Straub first elucidated the pathophysiology of the fibrocartilage anlage that spans the gap between the proximal ulna, the distal radius, and the ulnar carpus. This anlage lacks growth potential and acts as an unyielding tether. As the radius grows, the anlage forces the radius and carpus into severe ulnar deviation, causing subsequent bowing of the radial shaft and eventual dislocation of the radial head.
Most authorities agree that the ulnar anlage must be excised to prevent irreversible radial bowing and shortening. Resection of the distal end of the fibrocartilaginous mass is recommended before age 2 to 3 years, though some authors advocate for excision as late as age 6. Early excision is strongly indicated if there is progressive ulnar deviation at the radiocarpal joint, rapidly increasing radial bowing, or subluxation of the radial head. If radial bowing is already severe at the time of presentation, a corrective closing-wedge osteotomy of the radius may be performed concomitantly with anlage excision.
Creation of a One-Bone Forearm
If radial head dislocation creates a rigid mechanical block to elbow extension, the creation of a one-bone forearm (radioulnar synostosis) should be considered.
Surgical Warning: If the block in extension is clinically acceptable and functional pronation and supination are preserved, surgical creation of a one-bone forearm is contraindicated, as the loss of forearm rotation will likely decrease overall limb function.
However, if marked shortening and bowing of the radius are accompanied by severe forearm instability and restriction of elbow motion, a one-bone forearm will significantly improve stability and function.
* Prerequisite: For this procedure to be successful, a viable proximal ulna must be present.
* Staging: The proximal radius is usually excised several months prior to the creation of the one-bone forearm. Attempting simultaneous radial head excision and radioulnar synostosis is generally considered too surgically extensive for a single setting and increases the risk of neurovascular compromise and compartment syndrome.
SURGICAL TECHNIQUE: DEEPENING OF WEB AND METACARPAL OSTEOTOMY
To optimize prehension in patients with Cole & Manske Type B or C deficiencies, deepening of the first web space and rotational correction of the metacarpals are frequently required. It is usually safer and more predictable to undertake this correction in two distinct stages to protect the tenuous vascular supply of the dysplastic digits.
Stage 1: Web Space Deepening
- Incision and Flap Design: Deepen the first web space utilizing a broad Z-plasty or a four-flap Z-plasty, depending on the severity of the adduction contracture.
- Resection: Meticulously dissect and remove any redundant bone segments or rudimentary, non-functional digits that impede the web space.
- Soft Tissue Release: Release the adductor pollicis fascia and the first dorsal interosseous muscle origin if they are contributing to the contracture.
Stage 2: Metacarpal Osteotomy
- Approach: Once the soft tissue envelope has healed and matured from Stage 1, approach the targeted metacarpal via a dorsal longitudinal incision.
- Osteotomy: Perform a shortening or rotational osteotomy of the metacarpal. The goal is to rotate one or both border digits to provide an effective, oppositional pinch.
- Fixation: Secure the osteotomy with crossed smooth Kirschner wires (K-wires) to maintain the rotational alignment.
Postoperative Care
- Apply a well-padded, long-arm cast immediately postoperatively to protect the osteotomy and soft tissue reconstruction.
- Skin sutures are removed at 2 weeks.
- The cast and K-wires are typically removed at 4 to 6 weeks, pending radiographic evidence of clinical union.
- Normal activities and intensive occupational therapy for pinch mechanics are resumed gradually over the subsequent 4 to 6 weeks.
SURGICAL TECHNIQUE: TENDON TRANSFER FOR TYPE II DEFORMITIES (FLATT)
In patients with Type II deformities lacking active extrinsic tendon function but possessing supple joints, tendon transfers are indicated to restore active prehension. The Flatt technique utilizes wrist flexors or extensors extended by a tendon graft.
Indications and Prerequisites
- This procedure strictly requires a good, stable, and passive range of motion in the border digits. Tendon transfers will fail if placed across stiff or contracted joints.
Step-by-Step Surgical Approach
- Donor Identification: Identify the donor tendons—either the flexor carpi radialis (FCR), extensor carpi radialis longus (ECRL), or extensor carpi ulnaris (ECU)—through appropriate longitudinal incisions at the wrist.
- Graft Harvesting: Harvest the palmaris longus tendon (if present) or a strip of fascia lata to be used as an interpositional graft for the transfers.
- Proximal Coaptation: Secure the proximal end of the graft to the selected donor tendon utilizing a Pulvertaft weave. The Pulvertaft weave provides superior biomechanical strength by weaving the graft through the donor tendon multiple times, maximizing the surface area for tenocyte migration and healing. Secure the weave with non-absorbable mattress sutures.
- Distal Fixation: Route the graft distally to the border digits. Secure the distal ends of the graft into the terminal phalanges of the border digits utilizing a pull-out wire technique over a dorsal button. Ensure appropriate tensioning is achieved with the wrist in neutral to allow for the tenodesis effect.
Postoperative Protocol
- The wrist and digits are immobilized in a custom splint or cast with the wrist in mild flexion (if a flexor transfer) or mild extension (if an extensor transfer) to remove tension from the repair site.
- Immobilization is maintained strictly for 3 weeks.
- At 3 weeks, the pull-out wire, dorsal button, and skin sutures are removed.
- A protected, active range of motion protocol is initiated under the guidance of a specialized hand therapist.
- Normal activities and strengthening are resumed gradually during the next 4 to 6 weeks.
You Might Also Like