Mastering Complex Arthroplasty: Deformity Correction in TKR & THR
Key Takeaway
Deformity correction in total knee and hip replacement integrates Paley principles with arthroplasty. It requires understanding biomechanics, meticulous preoperative planning, and precise intraoperative techniques to restore mechanical axis, optimize soft tissue balance, and ensure long-term implant survivorship.
Introduction to Arthroplasty in the Deformed Limb
Total Knee Replacement and Total Hip Replacement are highly successful procedures in patients with standard anatomy. However, when degenerative joint disease is accompanied by severe extraarticular or intraarticular malalignment, the surgical complexity increases exponentially. These deformities frequently arise from developmental dysplasia, prior trauma, metabolic bone disease, or malunited osteotomies. Standard arthroplasty techniques applied to severely deformed bones inevitably lead to altered biomechanics, premature implant wear, instability, and catastrophic failure.
To achieve long term survivorship and optimal functional outcomes, the reconstructive surgeon must seamlessly merge the principles of joint arthroplasty with Paley principles of deformity correction. This requires a profound understanding of the Center of Rotation of Angulation, Mechanical Axis Deviation, and the intricate balance between bone deformity correction and soft tissue tensioning.
This comprehensive masterclass explores the advanced preoperative planning, biomechanical considerations, and intraoperative techniques required to successfully execute Total Knee Replacement and Total Hip Replacement in the setting of severe malalignment.
Core Principles of Deformity Correction in Joint Reconstruction
Before cutting bone or releasing soft tissue, the surgeon must deeply understand the foundational concepts introduced by Dr Dror Paley. These principles dictate how angular, translational, and rotational deformities alter the mechanical environment of the lower extremity and provide a mathematical framework for surgical correction.
Understanding Mechanical Axis Deviation
The mechanical axis of the lower extremity is a line drawn from the center of the femoral head to the center of the ankle plafond. In a normally aligned limb, this line passes slightly medial to the center of the knee joint. Deformities in the femur or tibia shift this axis, creating Mechanical Axis Deviation.
When performing a joint replacement in a deformed limb, the goal is not merely to replace the articular surface but to restore the Mechanical Axis Deviation to neutral. Failing to correct the mechanical axis results in asymmetric loading of the polyethylene bearing, leading to accelerated wear, osteolysis, and early aseptic loosening.
Center of Rotation of Angulation and Osteotomy Rules
The Center of Rotation of Angulation is the intersection point of the proximal and distal mechanical or anatomic axes of a deformed bone. Identifying the Center of Rotation of Angulation is the most critical step in preoperative planning for a concurrent osteotomy and arthroplasty. Dr Paley defined three fundamental osteotomy rules that dictate the outcome of deformity correction.
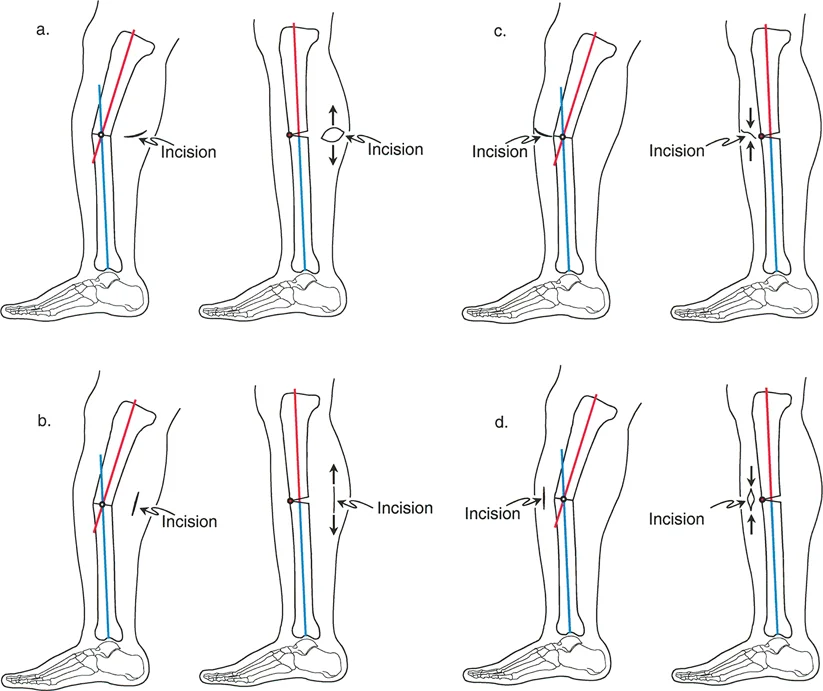
- Paley Rule One: When the osteotomy and the hinge axis of correction are both located at the Center of Rotation of Angulation, angulation is corrected without creating translation. This is the ideal scenario for restoring normal bone anatomy prior to implant insertion.
- Paley Rule Two: When the osteotomy is performed away from the Center of Rotation of Angulation, but the hinge axis of correction remains at the Center of Rotation of Angulation, the angulation is corrected, but translation of the bone ends occurs. This is frequently utilized when the Center of Rotation of Angulation is located too close to the joint line to allow for adequate implant fixation.
- Paley Rule Three: When the osteotomy and the hinge axis are both located away from the Center of Rotation of Angulation, a new deformity is created (typically a translation deformity) that alters the mechanical axis. This rule is generally avoided unless intentionally used to compensate for a multiapical deformity.
Normal Joint Orientation Angles
Reestablishing normal joint orientation angles is mandatory for symmetric gap kinematics in joint replacement. The surgeon must evaluate these angles on full length standing radiographs to determine the magnitude and apex of the deformity.
| Joint Orientation Angle | Abbreviation | Normal Value | Clinical Significance in Arthroplasty |
|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 87 Degrees | Dictates the distal femoral cut in Total Knee Replacement. |
| Medial Proximal Tibial Angle | MPTA | 87 Degrees | Dictates the proximal tibial cut in Total Knee Replacement. |
| Joint Line Convergence Angle | JLCA | 0 to 2 Degrees | Indicates intraarticular deformity or ligamentous laxity. |
| Mechanical Lateral Proximal Femoral Angle | mLPFA | 90 Degrees | Evaluates proximal femoral varus or valgus deformity. |
| Femoral Anteversion | None | 15 Degrees | Critical for hip stability and abductor lever arm mechanics. |
Biomechanics of Malalignment in Joint Replacement
Understanding how deformities alter the mechanical environment is essential for selecting the appropriate implant and surgical technique.
Altered Knee Kinematics and Implant Survivorship
In the knee, extraarticular deformities alter the tension of the collateral ligaments. A diaphyseal varus deformity of the femur, for example, will increase tension on the lateral collateral ligament and create laxity in the medial collateral ligament. If a surgeon attempts to correct a severe extraarticular deformity solely through intraarticular bone cuts during a Total Knee Replacement, they will inevitably violate the collateral ligament attachments.
Compensatory intraarticular resections often require cutting into the femoral epicondyles or the fibular head, destroying the origins and insertions of the primary stabilizing ligaments. This mandates the use of highly constrained, hinged prostheses, which have significantly lower long term survivorship compared to unconstrained implants. Therefore, Paley principles dictate that extraarticular deformities exceeding certain thresholds must be managed with an extraarticular osteotomy to preserve the joint line and ligamentous envelope.
Impact of Rotational Deformity on Hip Abductor Mechanics
In the hip, rotational deformities devastate the abductor mechanism. Excessive anteversion is frequently seen in developmental dysplasia of the hip, post traumatic malunions, or prior pediatric osteotomies.
When a femur exhibits marked anteversion, the greater trochanter is displaced to an extreme posterior location. This posterior displacement dramatically shortens the abductor lever arm. According to biomechanical principles, the hip abductors must generate a force significantly greater than body weight to maintain a level pelvis during the single leg stance phase of gait.
When the lever arm is lost, the abductors become mechanically disadvantaged. This leads to profound abductor dysfunction, a persistent Trendelenburg gait, and massively increased joint reaction forces. These elevated forces will rapidly degrade a standard Total Hip Replacement prosthesis. Furthermore, the normal medial to lateral dimensions of the proximal femur become oriented anteroposteriorly. This makes the insertion of a standard straight stem prosthesis exceptionally difficult, if not impossible, without cortical perforation or iatrogenic fracture.
Preoperative Planning for the Severely Deformed Limb
Meticulous preoperative planning is the cornerstone of successful arthroplasty in the deformed limb. The surgeon must transition from standard templating to advanced deformity mapping.
Clinical Evaluation and Imaging Protocols
The clinical evaluation must include a thorough assessment of gait, leg length discrepancy, and rotational profile. The surgeon must document the patient footprint progression angle, internal and external hip rotation in both flexion and extension, and the thigh foot axis.
Standard short arthroplasty radiographs are entirely inadequate. The imaging protocol must include:
* Full length, weight bearing anteroposterior radiographs of both lower extremities.
* Dedicated anteroposterior and lateral views of the affected joints.
* Computed Tomography scans to evaluate the rotational profile of the femur and tibia, specifically measuring femoral anteversion and tibial torsion.
Mapping the Deformity and Calculating Correction
Using the full length radiographs, the surgeon applies the Paley method to map the deformity.
Surgical Pearls for Deformity Mapping
* Draw the mechanical axis of the normal limb to establish a baseline.
* On the deformed limb, draw the proximal and distal mechanical axes of the affected bone.
* Identify the Center of Rotation of Angulation at the intersection of these axes.
* Measure the magnitude of the angular deformity.
* Determine the distance from the Center of Rotation of Angulation to the joint line. If this distance is extremely short, an intraarticular correction may be possible. If it is long, an extraarticular osteotomy is required.
Total Knee Replacement in Severe Malalignment
Managing severe malalignment during a Total Knee Replacement requires deciding between an intraarticular compensatory cut and an extraarticular corrective osteotomy.
Intraarticular Correction Versus Extraarticular Osteotomy
The general rule in orthopedic reconstruction is that an extraarticular deformity should be corrected with an extraarticular osteotomy. However, minor diaphyseal deformities can sometimes be accommodated within the joint capsule.
The threshold for concurrent osteotomy depends on the distance of the Center of Rotation of Angulation from the joint and the magnitude of the deformity. Generally, a femoral deformity greater than 20 degrees in the coronal plane, or a tibial deformity greater than 15 degrees, cannot be managed with intraarticular cuts alone without compromising the collateral ligament origins.
If the surgeon attempts to correct a 25 degree femoral varus deformity by altering the distal femoral resection angle, the medial condyle cut will be excessively deep, potentially resecting the medial epicondyle and the origin of the medial collateral ligament. In these scenarios, a concurrent or staged extraarticular osteotomy is mandatory.
Soft Tissue Balancing in the Deformed Knee
Soft tissue contractures inevitably accompany long standing bony deformities. The concave side of the deformity will feature contracted ligaments and capsule, while the convex side will be stretched and attenuated.
When performing an extraarticular osteotomy, the bony correction often resolves a significant portion of the soft tissue imbalance. However, residual contractures must be addressed through sequential releases. The surgeon must meticulously balance the flexion and extension gaps. In the setting of severe deformity, the use of computer navigation or robotic assistance can provide real time feedback on gap kinematics and mechanical axis restoration, ensuring that the soft tissue envelope is perfectly tensioned after the bone is realigned.
Step by Step Guide to TKR with Concurrent Osteotomy
When a concurrent osteotomy is indicated, the procedure must be carefully staged to ensure stability and alignment.
- Surgical Exposure: Standard midline incision and medial parapatellar arthrotomy.
- Osteotomy Execution: The extraarticular osteotomy is performed at the preplanned Center of Rotation of Angulation. A closing wedge or opening wedge technique is utilized based on leg length considerations.
- Intramedullary Canal Preparation: The medullary canal is reamed to accept a stemmed tibial or femoral component. The stem must bypass the osteotomy site by at least two cortical diameters to provide adequate biomechanical stability.
- Joint Preparation: Standard intraarticular bone cuts are made perpendicular to the newly corrected mechanical axis.
- Trialing and Alignment Check: Trial components are inserted. The mechanical axis is verified using a drop rod or computer navigation.
- Implant Fixation: The definitive stemmed components are cemented into place, bridging and stabilizing the osteotomy site.
- Supplemental Fixation: If rotational stability at the osteotomy site is a concern, supplemental plates or cables may be applied.
Total Hip Replacement in the Dysplastic and Deformed Femur
Managing severe proximal femoral deformity during Total Hip Replacement presents a unique set of challenges. The surgeon faces a critical decision regarding how to handle the abnormal anatomy. Should the deformity be accommodated using specialized implants, or should the bone be surgically corrected to fit a standard implant?
Implant Modification Versus Bone Correction
For mild to moderate rotational deformities, modular stems are highly effective. These implants feature separate metaphyseal and diaphyseal components. This modularity allows the surgeon to adjust the anteversion of the neck independently of the metaphyseal filling component. The surgeon can achieve a stable press fit in the distorted diaphysis while dialing in the necessary 15 degrees of anteversion for the articulation.
However, for severe deformities, particularly when proximal femoral anteversion exceeds 45 degrees, modular implants are often insufficient. In these extreme cases, Holtgrewe and Hungerford, along with Paley principles, strongly advocate for a corrective proximal femoral osteotomy performed concurrently with the placement of a standard hip replacement.
Advantages and Disadvantages of Concurrent Osteotomy
Choosing to perform a concurrent subtrochanteric osteotomy is a major surgical decision with distinct benefits and drawbacks.
Advantages of Concurrent Osteotomy
* Cost Effectiveness: Eliminates the need for highly expensive, custom machined prostheses or complex modular systems.
* Biomechanical Restoration: Corrects the deformity at its source, restoring the normal proximal femoral dimensions and allowing for the use of a standard, proven implant design.
* Abductor Mechanics: Repositions the greater trochanter laterally, instantly restoring the abductor lever arm. This cures the mechanical Trendelenburg gait and normalizes joint reaction forces, protecting the new bearing surfaces.
* Intraoperative Flexibility: The surgeon can dial in the exact degree of derotation, angular correction, and shortening needed before fixing the stem.
Disadvantages of Concurrent Osteotomy
* Prolonged Healing: Obligatory longer healing time, typically three to four months, for the osteotomy to achieve solid radiographic union.
* Postoperative Morbidity: Increased thigh pain and delayed weight bearing until the bone is fully healed.
* Technical Complexity: Requires advanced surgical skills to ensure the stem bypasses the osteotomy by at least two cortical diameters to provide adequate stability, while simultaneously managing the rotational alignment.
Surgical Technique for Subtrochanteric Derotational Osteotomy
When performing a Total Hip Replacement with a concurrent subtrochanteric derotational osteotomy, the procedure is meticulously staged intraoperatively to ensure absolute control over the bone segments.
Key Surgical Steps
- Exposure and Dislocation: The hip is exposed using the surgeon preferred approach. The deformed, dysplastic femoral head is resected, and the acetabulum is prepared and implanted with the definitive cup.
- Preparation of the Proximal Segment: The proximal femur is broached to accept the trial stem. Because of the severe anteversion, the broach is inserted in whatever rotation allows it to fit within the deformed metaphysis.
- Marking the Osteotomy: Before cutting the bone, longitudinal alignment marks are made on the anterior cortex of the femur across the planned osteotomy site. These marks are crucial for judging the degree of derotation.
- Executing the Osteotomy: A transverse or step cut osteotomy is performed in the subtrochanteric region. If the limb requires shortening to safely reduce the hip without stretching the sciatic nerve, a cylindrical segment of bone is resected.
- Preparation of the Distal Segment: The distal femoral canal is reamed to accept the diaphyseal portion of the fully porous coated or fluted tapered stem.
- Derotation and Trialing: The trial stem is inserted through the proximal segment and into the distal segment. The distal segment is externally rotated relative to the proximal segment to correct the excessive anteversion. The alignment marks are used to verify the exact degree of correction.
- Definitive Implantation: Once the rotation, leg length, and stability are confirmed, the definitive stem is impacted. The stem acts as an intramedullary nail, providing rigid internal fixation for the osteotomy.
- Bone Grafting: The resected femoral head or the cylindrical bone segment is milled into autograft and packed meticulously around the osteotomy site to promote rapid union.
Postoperative Management and Complication Avoidance
The postoperative care of a patient who has undergone arthroplasty with concurrent deformity correction is significantly more complex than standard joint replacement protocols.
Rehabilitation Protocols Following Concurrent Osteotomy
When a subtrochanteric or extraarticular osteotomy is performed, the rehabilitation protocol must protect the bone healing process while preventing joint stiffness.
- Weight Bearing Restrictions: Patients are typically restricted to toe touch or partial weight bearing for the first six to eight weeks. Full weight bearing is only permitted once radiographic evidence of bridging callus is observed.
- Range of Motion: Early, protected range of motion is encouraged to prevent arthrofibrosis, particularly in the knee. Continuous Passive Motion machines may be utilized.
- Abductor Strengthening: For hip patients, active abduction exercises are delayed until the osteotomy is stable to prevent excessive torque on the proximal femur.
Recognizing and Managing Nonunions and Hardware Failure
The most significant risks associated with concurrent osteotomy are nonunion and implant subsidence.
Surgeons must monitor serial radiographs at two, six, twelve, and twenty four weeks postoperatively. Signs of delayed union include persistent radiolucent lines at the osteotomy site, lack of callus formation, and increasing thigh pain. If a nonunion occurs, it may lead to fatigue fracture of the arthroplasty stem due to cyclical loading.
Management of a nonunion requires a thorough evaluation for infection. If aseptic nonunion is confirmed, intervention may include bone grafting, application of a supplemental compression plate, or revision to a larger diameter, longer stem to increase biomechanical stability.
By adhering strictly to Paley principles of deformity correction, ensuring robust implant fixation, and respecting the soft tissue envelope, reconstructive surgeons can successfully restore function and longevity to the most severely deformed and arthritic joints.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like