Paley Principles: Advanced Gait Biomechanics & Sagittal Deformity Correction
Key Takeaway
Paley Principles are crucial for advanced orthopedic deformity correction. This guide optimizes gait biomechanics and addresses sagittal plane deformities, like fixed knee flexion. It covers static analysis (mechanical axis, joint angles) and dynamic gait pathology (rockers, ground reaction vector) to restore efficient function.
Mastering Gait Biomechanics and Sagittal Plane Deformities
In the realm of advanced orthopedic deformity correction, achieving a visually straight limb on a static non weight bearing radiograph is only a fraction of the ultimate clinical goal. The true definitive measure of surgical success lies in the restoration of dynamic function specifically the optimization of the patient gait cycle and energy expenditure. Rooted deeply in the foundational principles established by Dr Dror Paley, understanding the intricate and unforgiving relationship between mechanical axis deviation, joint orientation angles, and dynamic ground reaction forces is paramount for any reconstructive surgeon.
While coronal plane deformities frequently dominate clinical discussions due to their role in asymmetric joint loading and premature osteoarthritis, it is the sagittal plane deformities that immediately and catastrophically disrupt the energy efficiency of walking. Specifically the fixed flexion deformity of the knee and rigid ankle stiffness create a debilitating cascade of biomechanical compensations. These compensations exhaust musculature, critically alter the ground reaction vector, and ultimately degrade the patient quality of life.
This comprehensive guide will exhaustively expand upon these biomechanical concepts, transforming basic textbook principles into highly actionable clinical insights for the advanced orthopedic surgeon and surgeon in training.
Foundational Paley Principles in Lower Extremity Reconstruction
Before analyzing dynamic gait pathology, the reconstructive surgeon must possess absolute mastery over static deformity analysis. Dr Dror Paley revolutionized orthopedic surgery by systematizing deformity analysis through geometric and anatomical principles. These principles allow surgeons to quantify the exact location, magnitude, and plane of any skeletal deformity, ensuring that surgical correction restores normal biomechanics rather than creating secondary iatrogenic deformities.
Mechanical Axis Deviation and Joint Orientation Angles
The mechanical axis of the lower extremity is defined by a line drawn from the center of the femoral head to the center of the ankle joint (tibial plafond). In a normal limb, this line passes through or just medial to the center of the knee joint. The distance from the center of the knee to this line is the Mechanical Axis Deviation.
To determine the source of the Mechanical Axis Deviation, surgeons rely on Joint Orientation Angles. These angles define the relationship between the mechanical or anatomic axes of the long bones and their respective joint lines. While coronal angles are widely known, sagittal plane angles are equally critical for addressing gait abnormalities.
| Angle Designation | Full Name | Normal Value Range | Plane |
|---|---|---|---|
| mLDFA | Mechanical Lateral Distal Femoral Angle | 85 to 90 degrees (avg 87) | Coronal |
| MPTA | Mechanical Proximal Tibial Angle | 85 to 90 degrees (avg 87) | Coronal |
| JLCA | Joint Line Convergence Angle | 0 to 2 degrees | Coronal |
| mPDFA | Mechanical Posterior Distal Femoral Angle | 79 to 87 degrees (avg 83) | Sagittal |
| mPPTA | Mechanical Posterior Proximal Tibial Angle | 77 to 84 degrees (avg 81) | Sagittal |
| ADTA | Anterior Distal Tibial Angle | 78 to 82 degrees (avg 80) | Sagittal |
The Center of Rotation of Angulation Methodology
The Center of Rotation of Angulation is the cornerstone of Paley deformity planning. It is the geometric point where the proximal mechanical axis line and the distal mechanical axis line intersect. Identifying the precise Center of Rotation of Angulation is non negotiable for accurate surgical correction.
When planning an osteotomy to correct a deformity, the relationship between the osteotomy site, the mechanical hinge, and the Center of Rotation of Angulation dictates the final geometric outcome. This relationship is defined by the Three Osteotomy Rules.
The Three Paley Osteotomy Rules
- Rule One states that if the osteotomy and the hinge are both placed exactly at the Center of Rotation of Angulation, the bones will undergo pure angulation. The mechanical axis will be completely realigned without any translation. This is the ideal scenario for most diaphyseal and metaphyseal deformities.
- Rule Two states that if the osteotomy is placed away from the Center of Rotation of Angulation, but the hinge remains at the Center of Rotation of Angulation, the bone will undergo both angulation and translation. The mechanical axis will be successfully realigned. This is frequently utilized when bone quality at the Center of Rotation of Angulation is poor, or when the Center of Rotation of Angulation lies within a joint space (requiring a metaphyseal osteotomy).
- Rule Three states that if the osteotomy and the hinge are both placed away from the Center of Rotation of Angulation, the bone will undergo angulation, but a secondary translation deformity will be created. The mechanical axis will remain deviated. Rule Three is generally considered a surgical error unless intentionally used to compensate for a parallel translation deformity.
Deconstructing the Normal Gait Cycle and Ground Reaction Vector
To accurately diagnose and surgically correct pathologic gait, one must first possess a granular biomechanical understanding of normal human locomotion. The human gait cycle is broadly divided into the stance phase constituting approximately sixty percent of the cycle and the swing phase constituting approximately forty percent. During the stance phase, the weight bearing limb must successfully navigate three distinct mechanical rockers to ensure smooth energy efficient forward progression of the body center of mass.
The Three Rockers of the Stance Phase
- First Rocker or Heel Rocker occurs from initial contact to foot flat. The posterior calcaneus acts as the mechanical fulcrum. During this brief window, eccentric contraction of the anterior tibialis and other dorsiflexors gently lowers the forefoot to the ground, absorbing shock and preventing a foot slap.
- Second Rocker or Ankle Rocker occurs during mid stance and is the powerhouse of forward progression. The tibia advances over the plantigrade foot. The ankle joint itself serves as the fulcrum, mechanically requiring a minimum of ten degrees of passive dorsiflexion to function correctly. Eccentric contraction of the gastrocnemius soleus complex meticulously controls the rate of anterior tibial advancement, stabilizing the knee.
- Third Rocker or Forefoot Rocker occurs from terminal stance to pre swing. The metatarsophalangeal joints act as the fulcrum. Concentric contraction of the powerful plantar flexors propels the body center of mass forward and upward into the swing phase.
Dynamics of the Ground Reaction Vector
The Ground Reaction Vector represents the three dimensional magnitude and direction of the force exerted by the ground on the body in response to gravity and momentum. During a normal stance phase, the Ground Reaction Vector constantly shifts its position relative to the anatomic joint centers of the hip, knee, and ankle, creating dynamic moments that must be balanced by muscles or ligaments.
At the hip, the Ground Reaction Vector generally passes posterior to the joint center during early stance creating an extension moment and anterior during late stance creating a flexion moment.
At the knee, this is the most critical joint for sagittal plane energy efficiency. During initial contact, the Ground Reaction Vector passes slightly anterior to the knee, creating a brief stabilizing extension moment. As the knee flexes slightly for shock absorption during the loading response, the Ground Reaction Vector moves posterior to the knee center, creating a flexion moment controlled by eccentric quadriceps firing. In mid to terminal stance, as the knee extends, the Ground Reaction Vector moves anteriorly again. This anterior shift is crucial because it creates a passive extension moment, allowing the massive quadriceps muscle to completely relax while the posterior capsule and ligaments provide passive energy free stability.
At the ankle, the Ground Reaction Vector passes anterior to the joint for the majority of the stance phase, creating a dorsiflexion moment that is continuously resisted by the Achilles tendon and calf musculature.
Any skeletal deformity whether bony procurvatum or soft tissue contracture that permanently alters the position of these joint centers relative to the Ground Reaction Vector will necessitate relentless muscular compensation, leading to rapid fatigue, joint pain, and pathologic gait patterns.
Sagittal Plane Deformities and Biomechanical Disruption
When the sagittal joint orientation angles deviate from the normative values established by Paley, the dynamic relationship between the joint centers and the Ground Reaction Vector is destroyed. Sagittal deformities are particularly punishing because they eliminate the passive locking mechanisms of the lower extremity, forcing active muscular contraction throughout the entire stance phase.
Fixed Flexion Deformity of the Knee
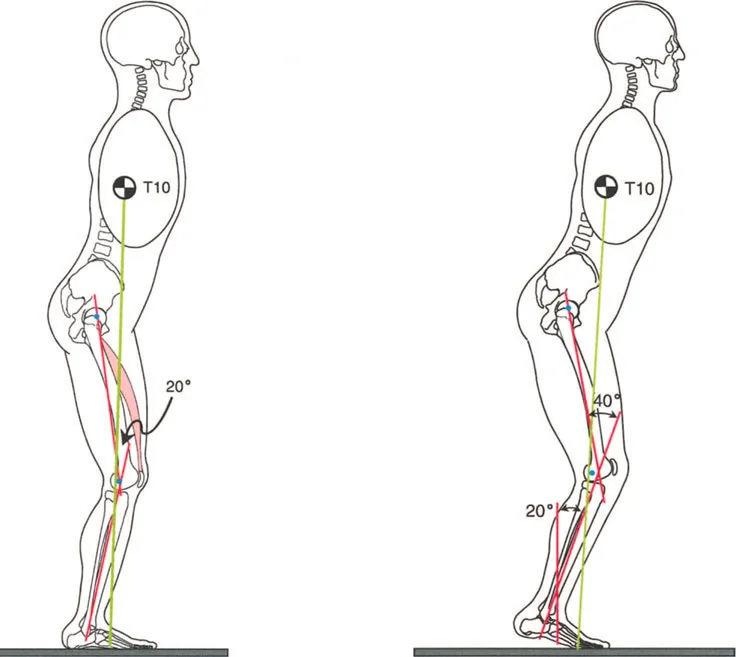
A Fixed Flexion Deformity of the knee is one of the most metabolically expensive deformities a patient can endure. Whether caused by bony malunion, posterior capsular contracture, or hamstring spasticity, a Fixed Flexion Deformity prevents the knee from achieving full extension during terminal stance.
Because the knee remains flexed, the Ground Reaction Vector is trapped posterior to the knee center of rotation. The normal passive extension moment is never achieved. Consequently, the quadriceps must fire continuously concentrically and eccentrically throughout the entire stance phase to prevent the knee from collapsing under the weight of the body. This relentless muscular demand leads to rapid lactic acid accumulation, profound fatigue, and dramatically reduced walking endurance. Furthermore, the constant anterior translation force of the tibia against the femur drastically increases patellofemoral joint reaction forces, leading to accelerated anterior compartment osteoarthritis.
Procurvatum and Recurvatum Skeletal Deformities
Bony deformities in the sagittal plane similarly alter the lever arms of the lower extremity.
Procurvatum deformities apex anterior angulation of the distal femur or proximal tibia artificially shift the mechanical joint center posteriorly. This exacerbates the flexion moment at the knee, mimicking the biomechanical effects of a soft tissue Fixed Flexion Deformity. Patients will often present with a crouch gait and complain of anterior knee pain due to quadriceps overactivity.
Recurvatum deformities apex posterior angulation shift the mechanical joint center anteriorly. This places the Ground Reaction Vector excessively anterior to the knee, creating a massive extension moment. While this allows the quadriceps to relax, it places catastrophic stress on the posterior capsule, the anterior cruciate ligament, and the posterolateral corner. Over time, this leads to progressive ligamentous stretching, posterior knee pain, and dynamic hyperextension instability.
Equinus and Calcaneus Contractures
At the level of the ankle, sagittal deformities directly obliterate the rocker mechanisms. An equinus deformity plantarflexion contracture forces the patient to make initial contact with the forefoot rather than the heel, completely eliminating the first rocker. During mid stance, the inability of the tibia to advance over the foot destroys the second rocker. To compensate, the knee is forced into hyperextension recurvatum to allow the center of mass to progress forward.
Conversely, a calcaneus deformity excessive dorsiflexion eliminates the third rocker. The calf musculature is mechanically disadvantaged, resulting in an inability to generate plantarflexion power for toe off. The patient exhibits a weak shuffling gait with severely diminished walking velocity.
Pathologic Gait Analysis and Pedobarography
When assessing complex gait abnormalities, pedobarography provides invaluable objective data regarding force distribution and the temporal phases of the stance cycle. Dynamic pressure mapping allows the surgeon to visualize exactly how a skeletal deformity translates into foot ground interaction.
A stiff ankle often resulting from post traumatic arthrofibrosis, severe equinus contractures, or surgical arthrodesis completely abolishes the normal second rocker mechanism. Because the tibia cannot smoothly advance over a plantigrade foot via ankle dorsiflexion, the entire foot ankle complex is forced to act as a single rigid lever.
Kinematic Findings in Ankle Stiffness
As noted in foundational deformity texts, a pedobarograph of a patient with a stiff ankle reveals several distinct quantifiable pathologic markers. Without the ability to dorsiflex, the center of pressure rapidly shifts anteriorly during the early stance phase. The normal gradual progression of force from the hindfoot to the midfoot and finally to the forefoot is lost.
Because the tibia cannot advance over the foot, the patient exhibits an early heel off, forcing a premature transition into the third rocker. This results in a shortened stride length on the contralateral side and increased vertical excursion of the center of mass. The body must vault over the rigid ankle lever, which drastically increases energy expenditure and oxygen consumption.
Compensatory Mechanisms in Sagittal Plane Pathology
Patients with sagittal plane deformities rarely present with isolated joint symptoms. The human body will instinctively sacrifice proximal or distal joints to maintain forward gaze and forward progression. Surgeons must be hyper vigilant in identifying these compensatory mechanisms during clinical evaluation.
- Pelvic Tilt and Lumbar Lordosis Patients with fixed hip flexion deformities or severe knee fixed flexion deformities will frequently hyperlordose their lumbar spine to maintain an upright posture. Correcting the knee deformity often spontaneously resolves the chronic lower back pain.
- Vaulting A patient with a functionally long limb due to a stiff ankle in equinus will plantarflex the contralateral normal ankle during mid stance to clear the pathologic limb during its swing phase.
- Circumduction Alternatively, to clear a functionally long limb, the patient will swing the leg outward in a semi circular arc, driven by the hip abductors.
Step by Step Preoperative Planning for Sagittal Deformities
Successful execution of Paley principles requires meticulous preoperative planning. The margin for error in sagittal plane deformity correction is exceptionally narrow, as even minor residual procurvatum or recurvatum can perpetuate gait dysfunction.
Clinical and Radiographic Assessment Protocol
- Obtain Full Length Standing Radiographs Standardized weight bearing orthogonal views are mandatory. For sagittal plane analysis, a true lateral radiograph of the entire limb from hip to ankle must be obtained. The patella must be facing strictly forward during the capture.
- Identify the Mechanical Axes Draw the mechanical axis of the femur connecting the center of the femoral head to the center of the knee. Draw the mechanical axis of the tibia connecting the center of the knee to the center of the ankle.
- Measure Joint Orientation Angles Calculate the mechanical Posterior Distal Femoral Angle and the mechanical Posterior Proximal Tibial Angle. Compare these to the normative data to isolate the exact location of the deformity.
- Locate the Center of Rotation of Angulation Extend the proximal and distal mechanical axes of the deformed bone until they intersect. This intersection point is the Center of Rotation of Angulation.
- Determine the Magnitude of Deformity The angle formed by the intersection of the proximal and distal mechanical axes represents the true magnitude of the angular deformity.
- Plan the Osteotomy Level Select the optimal site for bone division based on soft tissue envelope, bone quality, and desired fixation method.
- Apply the Osteotomy Rules Determine if the planned osteotomy will follow Rule One, Rule Two, or Rule Three. If Rule Two is utilized, calculate the exact amount of translation required to restore the mechanical axis.
High Yield Clinical Pearls for Deformity Planning
- Always assess the contralateral normal limb. Normative population data is a guide, but the patient contralateral limb provides the most accurate target for patient specific reconstruction.
- Beware of apparent deformities caused by rotation. A severe external tibial torsion can project as a valgus deformity on a coronal radiograph and a recurvatum deformity on a lateral radiograph. Always perform a rigorous clinical rotational profile.
- Soft tissue contractures must be differentiated from bony deformities. An examination under anesthesia or diagnostic nerve blocks can help isolate the source of a joint contracture before committing to a bony osteotomy.
Surgical Execution and Osteotomy Strategies
Once the preoperative plan is solidified, the surgeon must select the appropriate surgical technique and fixation construct to execute the correction. The choice of osteotomy and fixation is dictated by the magnitude of the deformity, the presence of limb length discrepancy, and the quality of the soft tissue envelope.
Osteotomy Geometry
The geometric shape of the osteotomy dictates the stability and healing potential of the correction.
Opening Wedge Osteotomies are technically straightforward and provide excellent correction of angular deformities while simultaneously adding length to the limb. However, they create a bony void that may require structural bone grafting and take longer to consolidate. In the sagittal plane, an anterior opening wedge of the proximal tibia is frequently used to correct severe recurvatum.
Closing Wedge Osteotomies provide excellent bony apposition and rapid healing due to the compressive forces across the osteotomy site. However, they inherently shorten the limb and require the sacrifice of healthy bone stock.
Focal Dome Osteotomies are highly versatile cylindrical cuts that allow for pure rotation around a central axis. When the center of the dome cut is perfectly aligned with the Center of Rotation of Angulation, massive angular corrections can be achieved without creating secondary translation or altering limb length. This is the preferred technique for severe periarticular deformities where translation cannot be tolerated.
Fixation Modalities
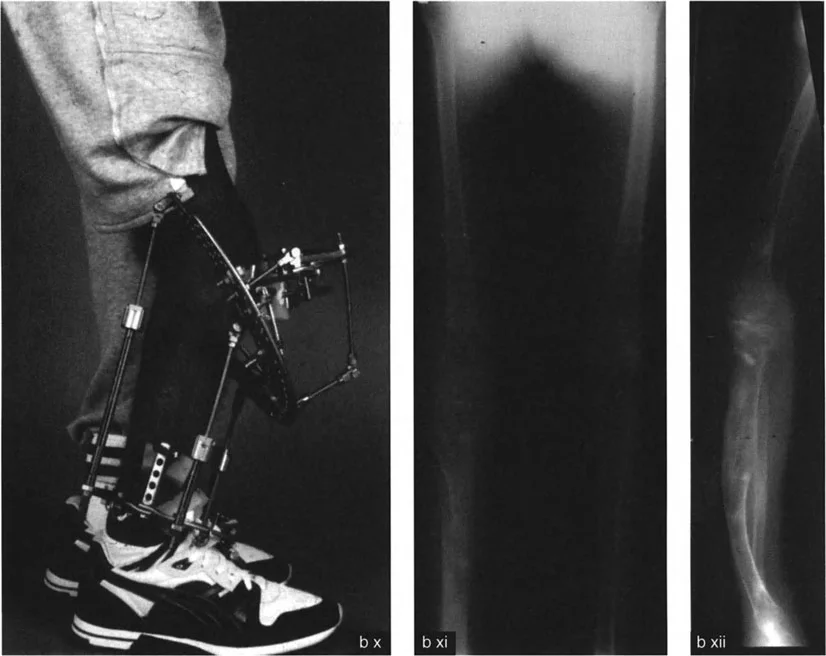
Internal Fixation utilizing rigid locking plates or intramedullary nails is preferred for acute corrections of mild to moderate deformities. Intramedullary nails offer load sharing biomechanics, allowing for early weight bearing, which is critical for restoring the normal gait cycle and preventing osteopenia.
External Fixation utilizing circular frames such as the Ilizarov apparatus or modern hexapod spatial frames is the gold standard for complex multi planar deformities, severe limb length discrepancies, and cases with compromised soft tissue. Hexapod frames utilize a virtual hinge, allowing the surgeon to place the hardware anywhere on the limb while the computer software calculates the strut adjustments necessary to rotate the bone fragments precisely around the true Center of Rotation of Angulation. This provides unparalleled precision and the ability to adjust the correction postoperatively.
Mastering these advanced biomechanical concepts and surgical techniques allows the reconstructive orthopedic surgeon to move beyond simply straightening bones. By meticulously restoring the mechanical axis, optimizing joint orientation angles, and respecting the dynamic forces of the ground reaction vector, the surgeon can profoundly restore the patient gait efficiency, eliminate pain, and return them to a life of unrestricted mobility.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like