The Paley Multiplier Method: Growth Plate Considerations in Pediatric Deformity Correction
Key Takeaway
The Paley Multiplier Method revolutionizes pediatric deformity correction by predicting leg length discrepancy at maturity using a single radiograph. It integrates growth plate dynamics, CORA, MAD, and Paley's osteotomy rules, providing a precise framework for managing complex skeletal deformities in growing children.
Growth Plate Considerations and the Multiplier Method in Deformity Correction
The management of pediatric orthopedic deformities requires a profound understanding of skeletal maturity, physeal behavior, and precise biomechanical alignment. Unlike adult deformity correction, where the osseous anatomy is static, the pediatric skeleton is a dynamic environment. Any surgical intervention must account for remaining growth, the potential for iatrogenic physeal injury, and the natural evolution of the deformity over time.
Dr Dror Paley revolutionized the approach to these complex challenges by integrating rigorous mathematical modeling with standardized radiographic analysis. By synthesizing the foundational data of Anderson, Green, and Maresh into the elegant Multiplier Method, and combining it with the principles of the Center of Rotation of Angulation (CORA) and Mechanical Axis Deviation (MAD), surgeons can now predict and correct deformities with unprecedented accuracy.
This comprehensive guide explores the intersection of growth plate dynamics, leg length discrepancy predictions, and Paley osteotomy rules, providing a high-yield framework for orthopedic surgeons, residents, and fellows.
The Evolution of Leg Length Discrepancy Prediction
Historically, predicting Leg Length Discrepancy (LLD) at skeletal maturity was a cumbersome process. Surgeons relied heavily on the Amstutz and Moseley straight-line graph systems. While these methods were groundbreaking, they required serial radiographs over several years, plotted on complex logarithmic charts, which often led to plotting errors and delayed surgical decision-making.
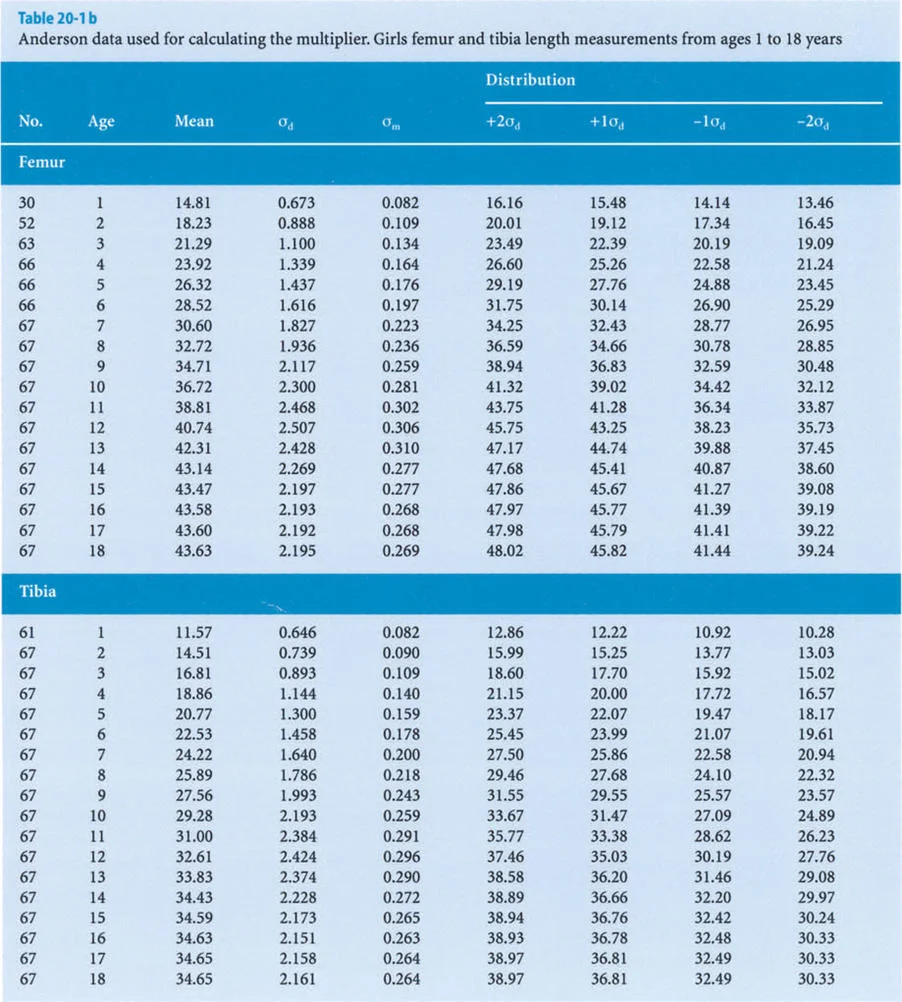
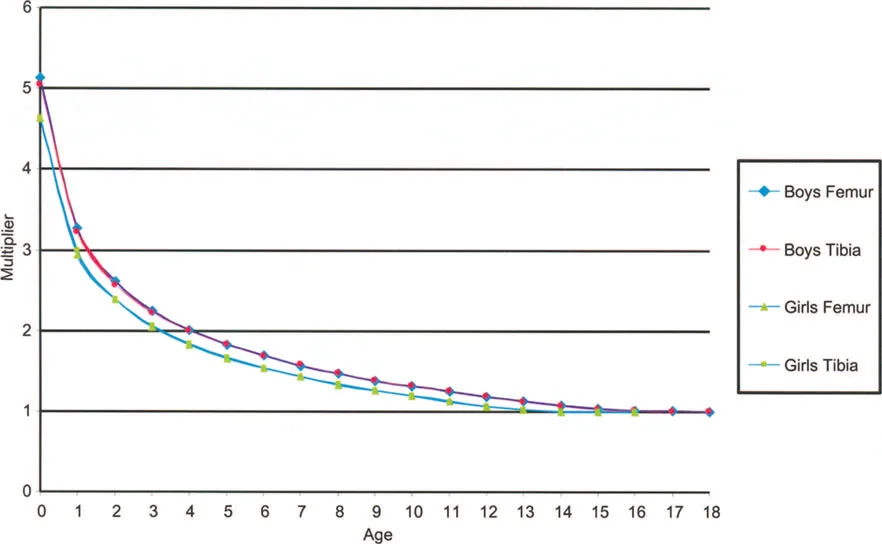
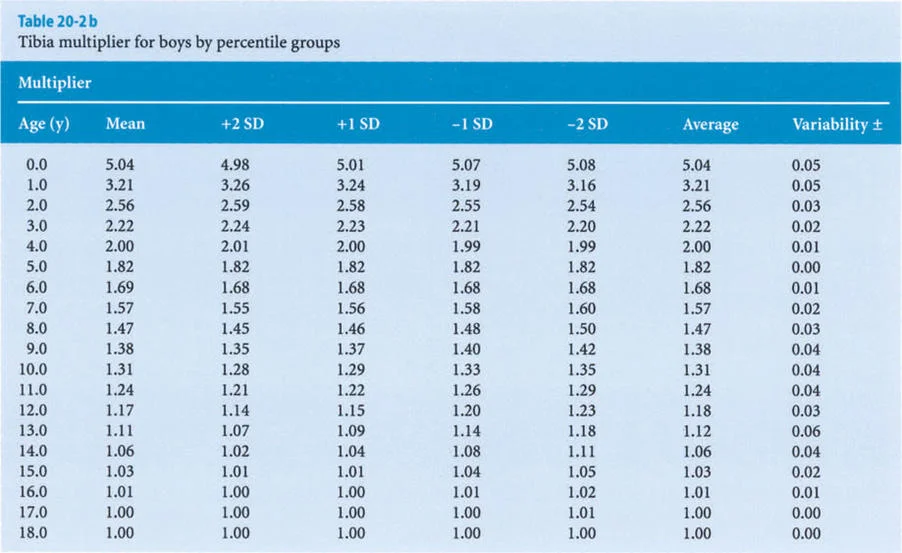
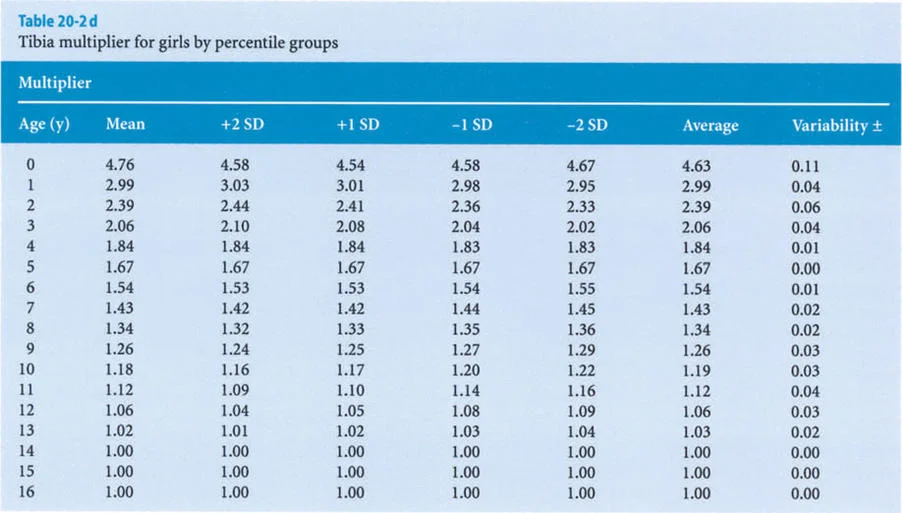
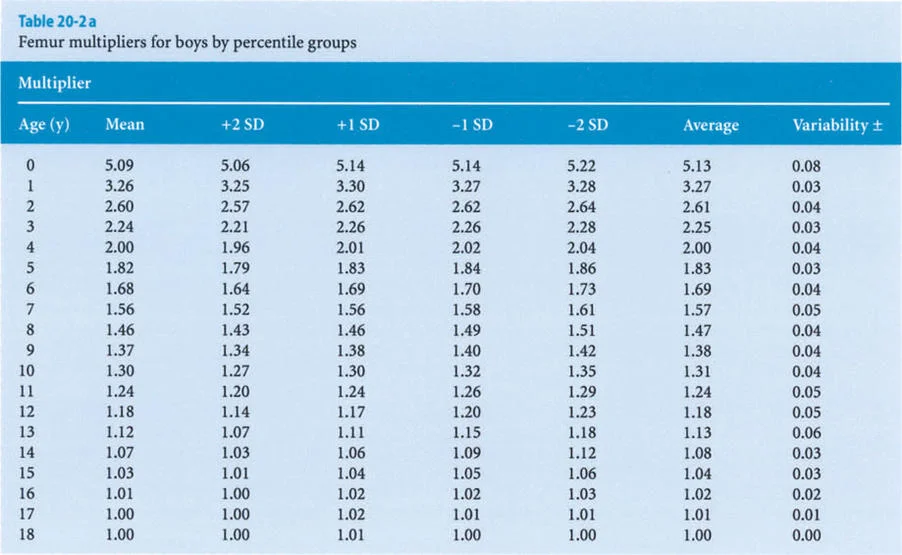
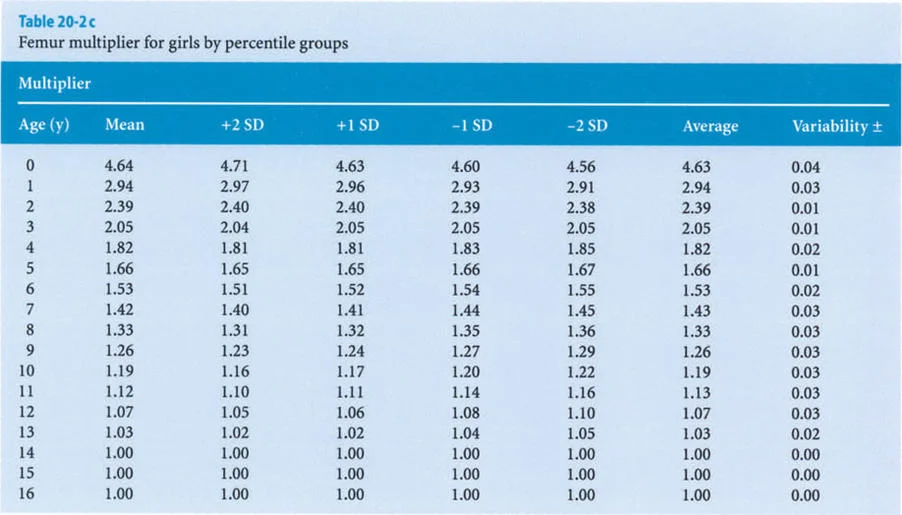
The foundational data for these early methods were derived from the monumental work of Anderson, Green, and Messner (1947, 1957, 1963, 1964). They meticulously recorded the femoral and tibial lengths of boys and girls at different chronological ages, categorizing the data into percentiles (5th, 33rd, 50th, 67th, and 95th) representing the mean, mean plus or minus one standard deviation, and mean plus or minus two standard deviations.
Despite the robustness of the Anderson and Green data, the clinical application remained tedious. Recognizing these limitations, Paley et al. sought to develop an alternative, streamlined method to predict LLD at skeletal maturity without the need for complex graphing or multiple historical data points.
The Paley Multiplier Method
The Multiplier Method distills decades of longitudinal growth data into a single, age-and-sex-specific coefficient. This method allows the surgeon to calculate the length of a bone at skeletal maturity using a single current radiograph.
Mathematical Derivation of the Multiplier
The core concept of the Multiplier Method is based on a simple proportional relationship. For each percentile group in the Anderson and Green database, Paley and colleagues divided the final length of the femur and tibia at skeletal maturity (Lm) by the corresponding length of that bone at each chronological year of age (L).
This calculation converted every single data point from the historical charts into a length-at-maturity multiplier (M). The formula is elegantly simple:
M = Lm / L
Conversely, to predict the final mature length of a bone in a growing child, the surgeon simply measures the current length of the femur or tibia (L) and multiplies it by the age-specific multiplier (M):
Lm = L × M
Expanding the Data to Infancy
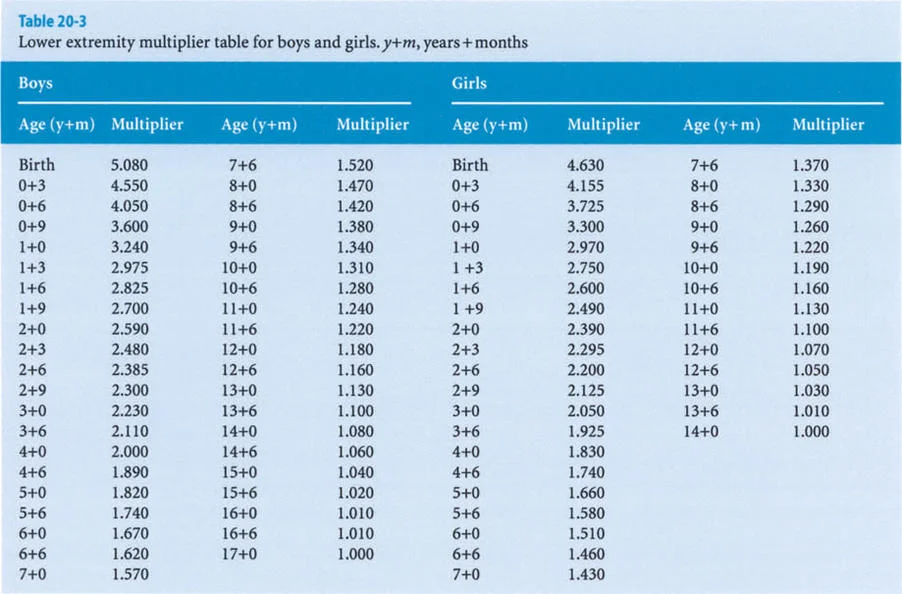
The original Anderson and Green database only began at age one year. To make the Multiplier Method applicable to infants and congenital deformities (such as Congenital Femoral Deficiency or Fibular Hemimelia), Paley applied the same mathematical principle to the dataset presented by Maresh (1955, 1970).
Maresh had reported radiographically measured femoral and tibial lengths from birth to skeletal maturity. Because the multipliers derived from the Maresh data for older children were virtually identical to those derived from the Anderson and Green data, Paley seamlessly integrated the infant multipliers from the Maresh data into the final Multiplier tables, creating a comprehensive predictive tool from birth to maturity.
Clinical Application of the Multiplier Method
To calculate the anticipated Leg Length Discrepancy at skeletal maturity, the surgeon follows these steps:
- Measure the current length of the normal leg (L normal).
- Measure the current length of the discrepant leg (L short).
- Identify the correct Multiplier (M) based on the patient's chronological age (or skeletal age if significantly delayed) and sex.
- Calculate the mature length of both legs:
- Mature Normal Leg = L normal × M
- Mature Short Leg = L short × M
- Subtract the Mature Short Leg from the Mature Normal Leg to find the final predicted LLD.
This calculation dictates whether the patient requires a shoe lift, an epiphysiodesis (growth arrest) of the longer leg, or a surgical lengthening procedure of the shorter leg.
Integrating Growth Plate Dynamics with Paley Principles
Predicting length is only one facet of pediatric deformity correction. Growth plate injuries, congenital anomalies, or metabolic bone diseases rarely present as isolated length discrepancies; they frequently involve angular and translational deformities. To correct these, we must rely on Paley's core biomechanical principles.
Mechanical Axis Deviation MAD
The mechanical axis of the lower extremity is a line drawn from the center of the femoral head to the center of the ankle joint (tibial plafond). In a normally aligned limb, this line passes slightly medial to the center of the knee joint.
Mechanical Axis Deviation (MAD) occurs when this line shifts outside the normal parameters.
- Medial MAD indicates a varus deformity.
- Lateral MAD indicates a valgus deformity.
In the growing skeleton, an asymmetric partial physeal arrest will progressively alter the MAD. For example, a premature closure of the medial distal femoral physis will tether medial growth while the lateral physis continues to expand. This results in progressive varus angulation and an increasing Medial MAD.
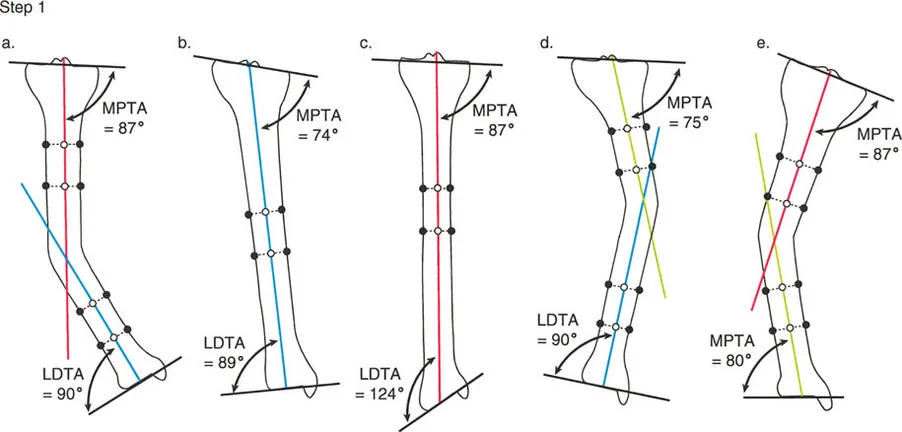
Joint Orientation Angles
To identify the exact anatomic source of the MAD, the surgeon must evaluate the joint orientation angles. These angles define the relationship between the mechanical axis of a specific bone segment and its joint line.
The most critical angles in the lower extremity include:
- mLDFA (Mechanical Lateral Distal Femoral Angle)
- MPTA (Mechanical Proximal Tibial Angle)
- JLCA (Joint Line Convergence Angle)
Normal Values for Joint Orientation Angles
| Angle | Normal Mean | Normal Range | Clinical Significance |
|---|---|---|---|
| mLDFA | 87.5 degrees | 85 to 90 degrees | Determines distal femoral varus or valgus. |
| MPTA | 87.5 degrees | 85 to 90 degrees | Determines proximal tibial varus or valgus. |
| JLCA | 0 to 2 degrees | 0 to 2 degrees | Indicates intra-articular deformity or ligamentous laxity. |
When a pediatric patient presents with an abnormal MAD, measuring the mLDFA and MPTA allows the surgeon to pinpoint whether the deformity originates in the femur, the tibia, or both.
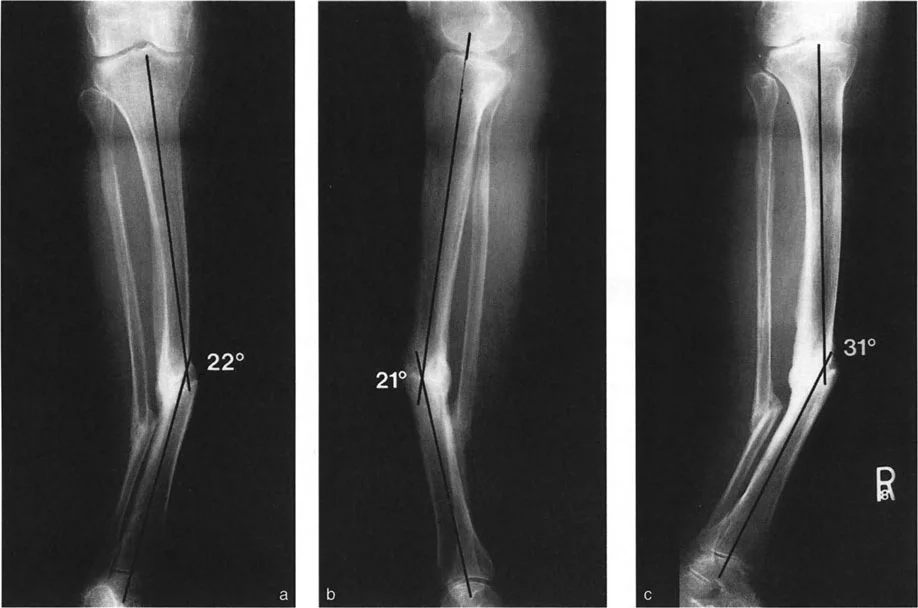
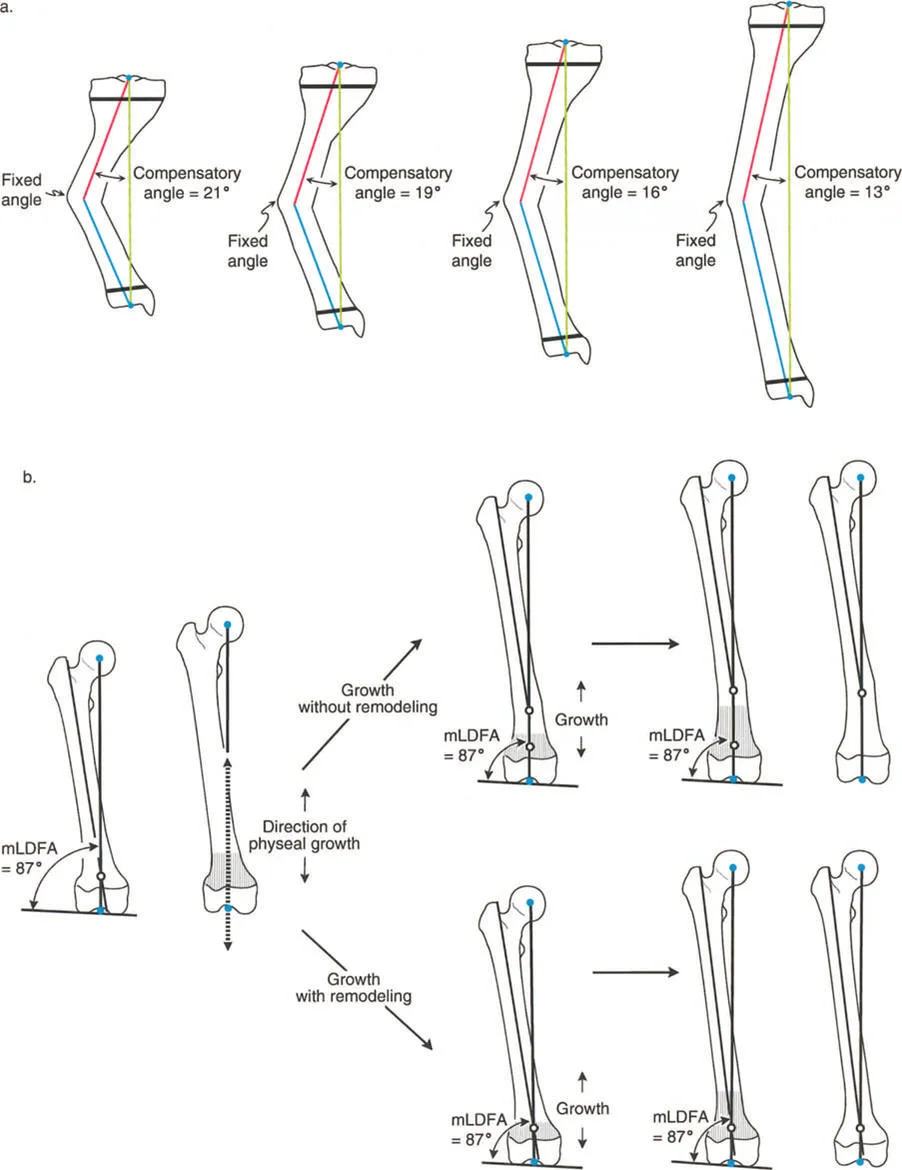
Center of Rotation of Angulation CORA in the Growing Skeleton
Once the deformed bone is identified via abnormal joint orientation angles, the surgeon must locate the apex of the deformity, known as the Center of Rotation of Angulation (CORA).
The CORA is found by drawing the proximal mechanical axis line and the distal mechanical axis line of the deformed bone segment. The point where these two lines intersect is the CORA.
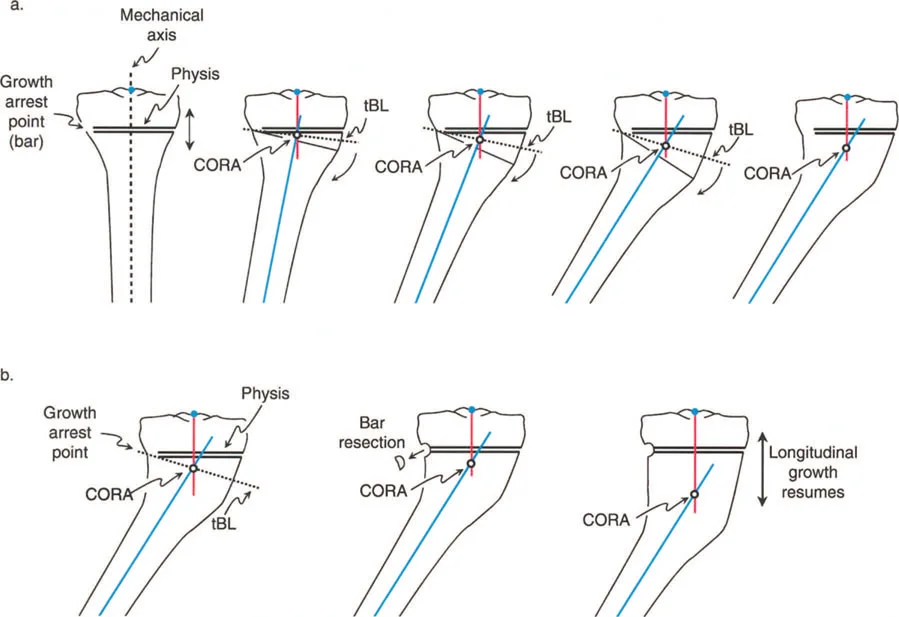
Juxta Articular CORAs and the Physis
In adult deformities (often secondary to malunited diaphyseal fractures), the CORA is typically located in the diaphysis or metaphysis. However, in pediatric deformities caused by growth plate arrest or dysplasia, the CORA is almost always juxta-articular—located exactly at or immediately adjacent to the physis.
This presents a unique surgical challenge. You cannot simply cut through an open growth plate to correct an angle without causing permanent, complete physeal arrest. Therefore, standard osteotomy techniques must be modified using Paley's Osteotomy Rules.

Paley Osteotomy Rules Applied to Growth Plate Deformities
Dr Paley established three fundamental rules for osteotomy placement relative to the CORA. Understanding how to apply these rules when the CORA is located at an open physis is the hallmark of advanced pediatric deformity correction.
Osteotomy Rule 1
The Rule: When the osteotomy and the mechanical hinge (axis of correction) are both placed exactly at the CORA, the bone will undergo pure angular correction without any translation. The mechanical axis will be perfectly realigned.
Application in Pediatrics: If the CORA is at the physis, applying Rule 1 means cutting through the growth plate. This is strictly contraindicated in a growing child unless the surgeon intends to perform a complete epiphysiodesis. Therefore, Rule 1 is rarely used for juxta-articular pediatric deformities unless the patient has reached skeletal maturity.
Osteotomy Rule 2
The Rule: When the mechanical hinge is placed at the CORA, but the osteotomy is performed at a different level (away from the CORA), the mechanical axis will be realigned, but the bone ends at the osteotomy site will translate relative to one another.
Application in Pediatrics: This is the workhorse rule for pediatric deformity correction. Because the CORA is at the physis, the surgeon places the hinge at the CORA (the joint line/physis) but performs the actual bone cut (osteotomy) safely in the metaphysis or diaphysis. As the angular correction is made, the bone ends will translate. The surgeon must anticipate this translation and ensure adequate bony contact is maintained for healing.
Osteotomy Rule 3
The Rule: When both the osteotomy and the mechanical hinge are placed away from the CORA, the mechanical axis will remain parallel to the desired axis but will be translated. This results in a new, iatrogenic translation deformity.
Application in Pediatrics: Rule 3 is generally avoided unless the surgeon is intentionally trying to create translation to compensate for an existing multi-apical deformity. If a surgeon mistakenly places the hinge away from a physeal CORA, the resulting mechanical axis will be shifted, leading to persistent MAD despite the bone appearing straight.
Guided Growth Hemiepiphysiodesis
While acute osteotomies are powerful, the gold standard for correcting angular deformities in the growing skeleton is guided growth (hemiepiphysiodesis). This technique harnesses the child's remaining growth to correct the deformity over time, avoiding the morbidity of an osteotomy.
Mechanism of Action
Guided growth involves placing a tension band (such as an eight-Plate or similar construct) across one side of the physis.
- For a valgus deformity (lateral MAD, abnormal mLDFA), the plate is placed on the medial side of the distal femur or proximal tibia. This tethers medial growth while lateral growth continues, gradually swinging the mechanical axis back to neutral.
- For a varus deformity (medial MAD), the plate is placed on the lateral side.
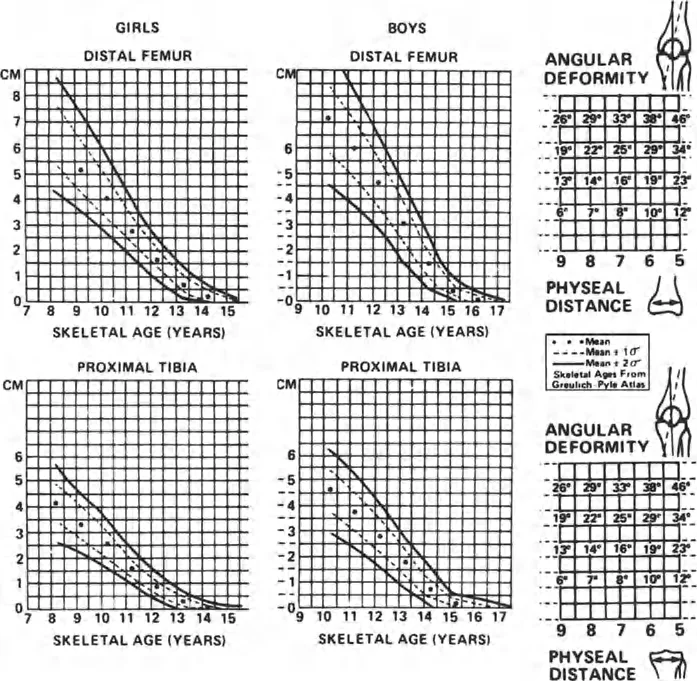
Timing and the Multiplier Method
The success of guided growth depends entirely on the patient having sufficient remaining growth. This is where the Multiplier Method becomes invaluable. By calculating the patient's skeletal age and utilizing the multiplier, the surgeon can estimate how much growth remains in the distal femur (which contributes 70 percent of femoral growth) or the proximal tibia (which contributes 55 percent of tibial growth).
If a patient is too close to skeletal maturity (Multiplier approaches 1.0), guided growth will fail, and an acute osteotomy (applying Rule 2) is indicated.
Step by Step Preoperative Planning for Pediatric Deformities
Meticulous preoperative planning is mandatory to achieve optimal outcomes. Surgeons should follow a standardized protocol for every pediatric patient presenting with LLD or angular deformity.
Clinical Evaluation and Imaging
- Physical Examination: Assess rotational profile, joint range of motion, ligamentous stability, and perform the Galeazzi test to isolate the segment of shortening.
- Standardized Radiographs: Obtain a standing, full-length, weight-bearing anteroposterior (AP) radiograph of both lower extremities with the patellae oriented strictly forward.
- Bone Age Assessment: Obtain a left hand/wrist radiograph to determine skeletal age (Greulich and Pyle atlas), which is critical for accurate Multiplier Method calculations.
Radiographic Analysis
- Calculate MAD: Draw the mechanical axis from the center of the femoral head to the center of the ankle. Measure the deviation (in millimeters) from the center of the knee.
- Measure Joint Orientation Angles: Calculate the mLDFA, MPTA, and JLCA. Compare these to normative data to isolate the deformity to the femur, tibia, or joint space.
- Locate the CORA: Draw the proximal and distal mechanical axes of the deformed bone. Identify the intersection point.
- Calculate LLD: Measure the current lengths of the femur and tibia. Apply the appropriate Paley Multiplier based on skeletal age and sex to predict the final LLD at maturity.

Surgical Decision Making
- Select the Intervention:
- If significant growth remains and the deformity is purely angular: Plan for guided growth (hemiepiphysiodesis).
- If the patient is near skeletal maturity or the deformity is severe/multi-planar: Plan for an acute osteotomy.
- If significant LLD is predicted (>2-3 cm): Plan for a lengthening procedure (external fixation or internal lengthening nail) or a contralateral epiphysiodesis, depending on the projected final height.
- Apply Osteotomy Rules: If performing an osteotomy, recognize that the CORA is likely near the physis. Plan a metaphyseal osteotomy with the hinge at the CORA (Rule 2) to ensure proper mechanical axis realignment with anticipated translation.
Surgical Pearls for Pediatric Deformity Correction
To maximize outcomes and minimize complications, keep these high-yield clinical pearls in mind:
- Respect the Physis: Never perform a Rule 1 osteotomy through an open growth plate unless a complete epiphysiodesis is the explicit goal. Always use Rule 2 for juxta-articular CORAs in growing children.
- Account for the JLCA: A widened Joint Line Convergence Angle can mimic a bony deformity. Always assess for ligamentous laxity. If the JLCA is abnormal, your bony correction must account for the soft tissue imbalance, or the MAD will remain uncorrected.
- Skeletal Age is King: Chronological age is often misleading. Always base your Multiplier Method calculations on skeletal age to avoid over- or under-correcting LLD.
- Anticipate Rebound: When using guided growth, overcorrect the mechanical axis slightly into the opposite quadrant (e.g., slight varus for a valgus correction). Rebound growth frequently occurs after plate removal, and this slight overcorrection prevents recurrent deformity.
- Monitor Fixator Hardware: If using external fixation for lengthening, ensure pins and wires are placed meticulously to avoid tethering the IT band or traversing the open physis.
- Translation is Normal in Rule 2: Do not be alarmed by the translation that occurs during a Rule 2 osteotomy. As long as the mechanical axis is restored and there is greater than 50 percent bony apposition, the metaphyseal bone will remodel beautifully in a child.

Conclusion
Mastering growth plate considerations is essential for any orthopedic surgeon treating pediatric limb deformities. By moving away from archaic graphing methods and embracing the Paley Multiplier Method, surgeons can accurately predict Leg Length Discrepancy with a simple calculation.
Furthermore, by strictly adhering to the principles of Mechanical Axis Deviation, Joint Orientation Angles, and the Center of Rotation of Angulation, surgeons can safely navigate the complexities of the open physis. Whether employing guided growth or executing a meticulously planned Rule 2 osteotomy, the integration of these biomechanical and mathematical principles ensures predictable, reproducible, and excellent clinical outcomes for the growing patient.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like