Mastering Knee Joint Line Deformity: Advanced Diagnosis & Precision Correction

Key Takeaway
Knee joint line deformity refers to angular malalignment originating within the knee articulation, often due to asymmetric cartilage loss or bone depression. Accurate diagnosis requires stress radiographs to differentiate true bone/cartilage loss from ligamentous laxity, ensuring precise intra-articular correction using Paley principles.
Introduction to Knee Joint Line Deformity
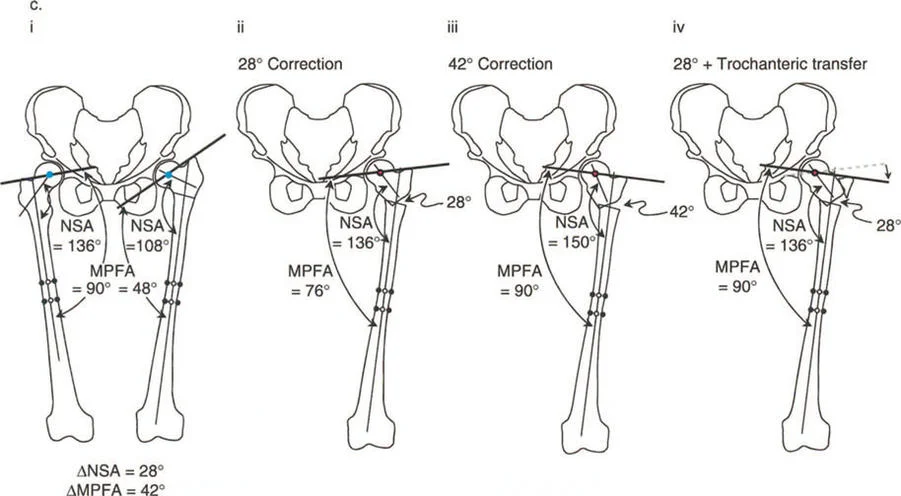
Welcome to the definitive masterclass on one of the most complex and nuanced topics in orthopedic deformity correction. In the comprehensive study of lower extremity realignment, orthopedic surgeons in training often focus heavily, and sometimes exclusively, on diaphyseal and metaphyseal sources of mechanical axis deviation. Surgical training meticulously emphasizes calculating the mechanical lateral distal femoral angle and the mechanical medial proximal tibial angle to locate the Center of Rotation of Angulation.
However, a critical and frequently misunderstood component of lower limb alignment lies directly within the articulation itself. This component is knee joint line deformity.
Historically in the Paley principles of deformity correction, malalignment is typically attributed to femoral and tibial shaft or metaphyseal deformities, or to joint laxity and subluxation between the femur and tibia. But what happens when the joint surfaces themselves are the primary source of the angular deformity? What happens when the preoperative map used to correct the bone leads directly into the joint space?
The remaining sources of malalignment stem from bone and cartilage loss, or congenital and developmental dysplasia of the knee joint surfaces. The most common culprit in the adult population is asymmetric cartilage loss from the medial or lateral knee compartments, typical of advanced osteoarthritis or post traumatic degeneration. In the pediatric population, conditions like Blounts disease or physeal arrests dominate the landscape.
This masterclass dives deep into the biomechanics, preoperative planning, and surgical execution required to correct intra articular knee joint line deformities. By integrating foundational Paley principles with advanced intra articular osteotomy techniques, this guide provides the framework required for mastering joint preservation and complex realignment.
Fundamentals of Mechanical Axis Deviation
Before addressing the joint line directly, the surgeon must master the standard parameters of lower extremity alignment. The mechanical axis of the lower extremity is defined by a line drawn from the center of the femoral head to the center of the ankle joint. In a normal, neutrally aligned limb, this line passes slightly medial to the center of the knee joint.

Mechanical Axis Deviation occurs when this line shifts outside the normal parameters, falling excessively into the medial compartment (varus deformity) or the lateral compartment (valgus deformity). To determine the source of the Mechanical Axis Deviation, surgeons rely on specific joint orientation angles.
Key Joint Orientation Angles
Understanding the normal values of these angles is non negotiable for accurate preoperative planning.
| Parameter | Definition | Normal Range | Average |
|---|---|---|---|
| mLDFA | Mechanical Lateral Distal Femoral Angle | 85 to 90 degrees | 87.5 degrees |
| mMPTA | Mechanical Medial Proximal Tibial Angle | 85 to 90 degrees | 87.5 degrees |
| JLCA | Joint Line Congruency Angle | 0 to 2 degrees | 1 degree |
| MAD | Mechanical Axis Deviation | 0 to 15 mm medial | 8 mm medial |
When the mLDFA and mMPTA are within normal limits, yet a Mechanical Axis Deviation is still present, the surgeon must immediately turn their attention to the joint line itself.
Biomechanics of the Joint Line Congruency Angle
To truly understand knee joint line deformity, we must first master the biomechanics of the Joint Line Congruency Angle. The JLCA is the absolute cornerstone of intra articular deformity analysis.
In a normal, healthy knee, the joint line of the distal femur (drawn across the most distal points of the medial and lateral femoral condyles) and the joint line of the proximal tibia (drawn across the medial and lateral tibial plateaus) are virtually parallel. This parallel relationship results in a perfectly congruent joint space that distributes load evenly across the articular cartilage during the gait cycle.
When cartilage is lost asymmetrically, such as in classic medial compartment osteoarthritis, or when a tibial plateau is physically depressed due to high energy trauma or developmental disease, these two joint lines lose their parallel relationship. The biomechanical effect is a pathological increase in the JLCA.
As the JLCA increases, shear forces across the joint multiply. The knee begins to act as a mechanical wedge rather than a congruent hinge. This accelerates further cartilage degradation and exacerbates the Mechanical Axis Deviation, creating a vicious cycle of deformity and joint destruction.
Etiology of Intra Articular Knee Deformity
Intra articular deformities do not arise spontaneously. They are the result of specific pathological processes that alter the bony or cartilaginous anatomy of the distal femur or proximal tibia.
Degenerative Cartilage Loss
The most frequent cause of an abnormal JLCA in adults is osteoarthritis. Asymmetric wear, typically in the medial compartment, leads to a loss of joint space height. This effectively shortens the medial column of the knee, driving the limb into varus and increasing the JLCA.
Post Traumatic Deformity
Intra articular fractures, such as Schatzker type tibial plateau fractures or distal femoral coronal shear fractures, frequently heal with residual depression. If a lateral tibial plateau remains depressed by 10 millimeters following a fracture, the tibial joint line is permanently altered, creating a valgus intra articular deformity.
Developmental and Congenital Dysplasia
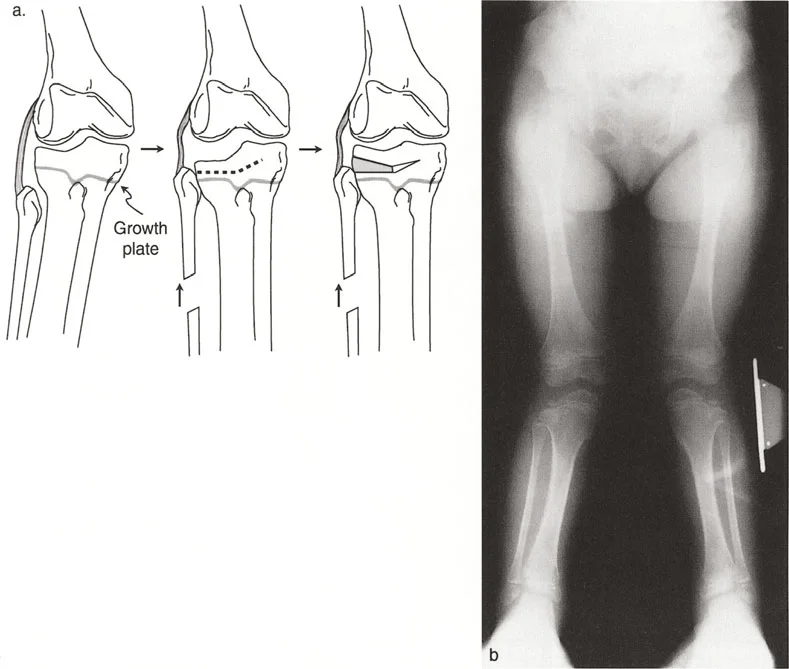
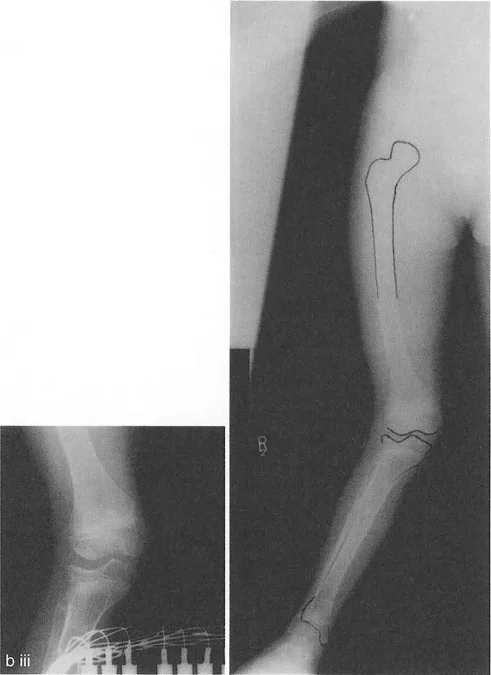
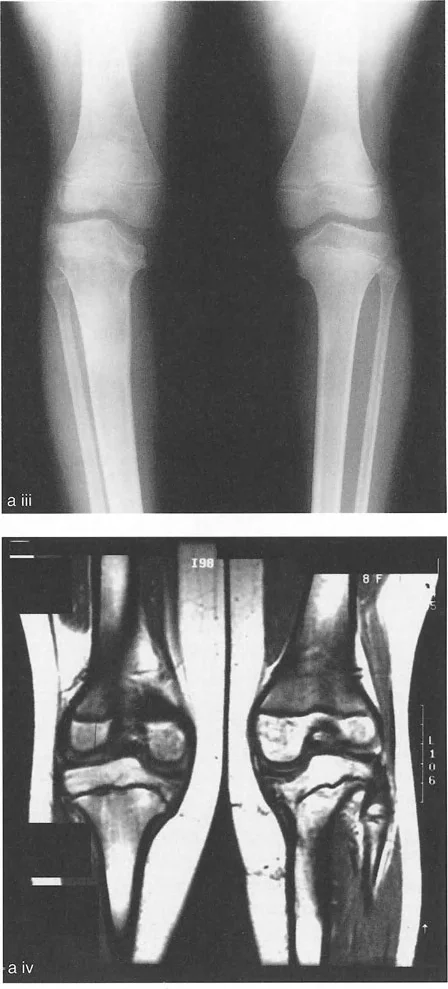
In pediatric orthopedics, conditions like infantile or adolescent Blounts disease cause a distinct depression of the posteromedial tibial plateau due to disordered physeal growth. This creates a severe intra articular varus deformity that cannot be fully corrected with a standard extra articular metaphyseal osteotomy alone.
Diagnostic Evaluation of Knee Joint Line Deformity
An increased JLCA on a standard weight bearing anteroposterior radiograph presents a profound diagnostic challenge for the orthopedic surgeon.
The Diagnostic Dilemma Cartilage Loss Versus Ligamentous Laxity
When evaluating a radiograph showing joint space narrowing on one side and an angular deviation, the surgeon must ask a critical question. Is this joint space narrowing due to true physical loss of cartilage and bone, or is the joint simply opening up on the contralateral side due to collateral ligament laxity?
Although cartilage loss and ligamentous laxity are frequently found together, they must be strictly distinguished from one another during the preoperative planning phase. For example, a severe varus knee will often present with medial cartilage loss and simultaneous lateral collateral ligament stretching.
If a surgeon assumes the entire deformity is osseous and plans a massive bone wedge correction, they will overcorrect the bone. The patient will be left with a straight bone but a persistently unstable, floppy joint.
Executing Stress Radiographs for Accurate Assessment
The gold standard for assessing an abnormal JLCA is the use of stress radiographs. Standard weight bearing films are highly insufficient for differentiating between bone loss and ligamentous laxity. Both sources of an increased JLCA must be assessed by means of varus and valgus stress radiographs, ideally performed under live fluoroscopy.
Surgeons must measure two distinct parameters during stress testing.
- Minimum Cartilage Space This is measured on the side of the deformity under compression stress. For example, applying valgus stress to a varus knee compresses the lateral side, while varus stress compresses the medial side. This reveals the true remaining cartilage height and bone congruency.
- Maximum Cartilage Space This is measured under tension stress to evaluate ligamentous competence. If the joint space opens excessively under tension compared to the contralateral normal knee, ligamentous laxity is a definitive contributing factor to the Mechanical Axis Deviation.
| Diagnostic Finding | Compression Stress Result | Tension Stress Result | Clinical Interpretation |
|---|---|---|---|
| Pure Cartilage Loss | Joint space remains narrow | Joint space opens to normal height | Deformity is osseous or cartilaginous; incorporate into bony correction. |
| Pure Ligamentous Laxity | Joint space compresses to normal height | Joint space opens excessively | Deformity is soft tissue driven; consider ligamentous reconstruction. |
| Mixed Deformity | Joint space remains narrow | Joint space opens excessively | Combined approach required; correct bone for cartilage loss, address ligaments for laxity. |
If an increased JLCA is definitively identified as being due to the loss of cartilage height or actual bone depression, this specific component of angulation must be incorporated into the total magnitude of angular correction. Failing to account for this intra articular angulation will result in under correction of the mechanical axis during a standard extra articular metaphyseal osteotomy.
Paleys Rule of Joint Line Substitution
When planning a realignment of the tibia or femur in cases with an increased JLCA due to joint space narrowing, standard mMPTA and mLDFA calculations become highly skewed if the surgeon relies solely on the deformed articular surface. A reliable horizontal reference line is required to calculate the true Center of Rotation of Angulation.
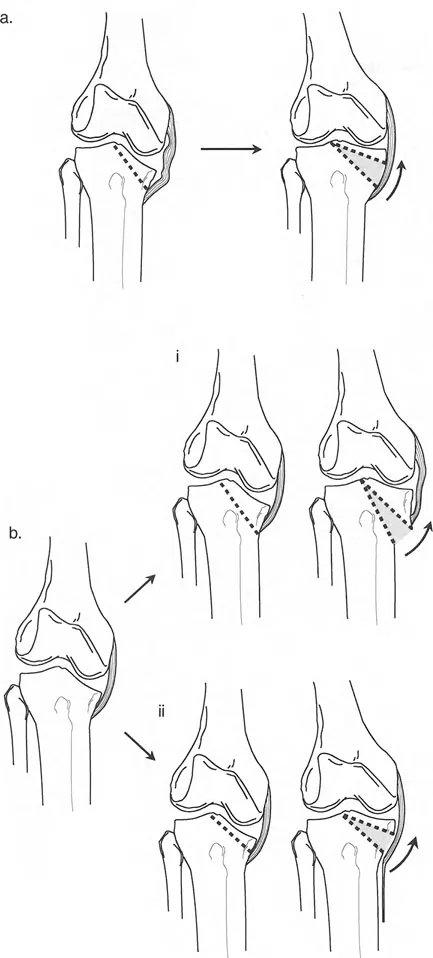
To solve this, Dr. Dror Paley introduced the Rule of Joint Line Substitution. This principle allows the surgeon to bypass the destroyed joint line and utilize the healthy opposing joint line as a template.
Step by Step Joint Line Substitution
- Identify the Deformed Surface Determine whether the primary deformity lies on the femoral side (e.g., condylar hypoplasia) or the tibial side (e.g., plateau depression).
- Verify the Healthy Surface Ensure the opposing articular surface is anatomically normal. If the tibia is deformed, verify the distal femur has a normal mLDFA.
- Transpose the Joint Line Draw a line parallel to the healthy joint surface and transpose it across the joint space onto the deformed bone.
- Establish the New Reference Use this transposed, substituted line as the new joint orientation line for the deformed bone.
- Calculate the CORA Draw the mechanical axis lines based on this substituted joint line to find the true Center of Rotation of Angulation.
By utilizing the Rule of Joint Line Substitution, the surgeon ensures that the planned osteotomy will not only correct the diaphyseal alignment but will also perfectly compensate for the intra articular wedge effect caused by the abnormal JLCA.
Locating the Center of Rotation of Angulation
The Center of Rotation of Angulation is the foundational concept in the Paley method of deformity correction. The CORA is defined as the intersection point of the proximal mechanical axis line and the distal mechanical axis line of a deformed bone.
In standard diaphyseal deformities, the CORA is located in the shaft of the bone. However, in cases of severe knee joint line deformity, the mechanical axis lines often intersect directly at the joint line, or even within the joint space itself. This indicates an intra articular CORA.
Applying Paleys Osteotomy Rules to the Knee
When the CORA is located within the knee joint, the surgeon must decide how to execute the correction. Cutting directly through the joint (intra articular osteotomy) is biomechanically ideal but technically demanding and carries risks of joint stiffness. Cutting outside the joint (extra articular osteotomy) is safer but requires specific geometric compensations.
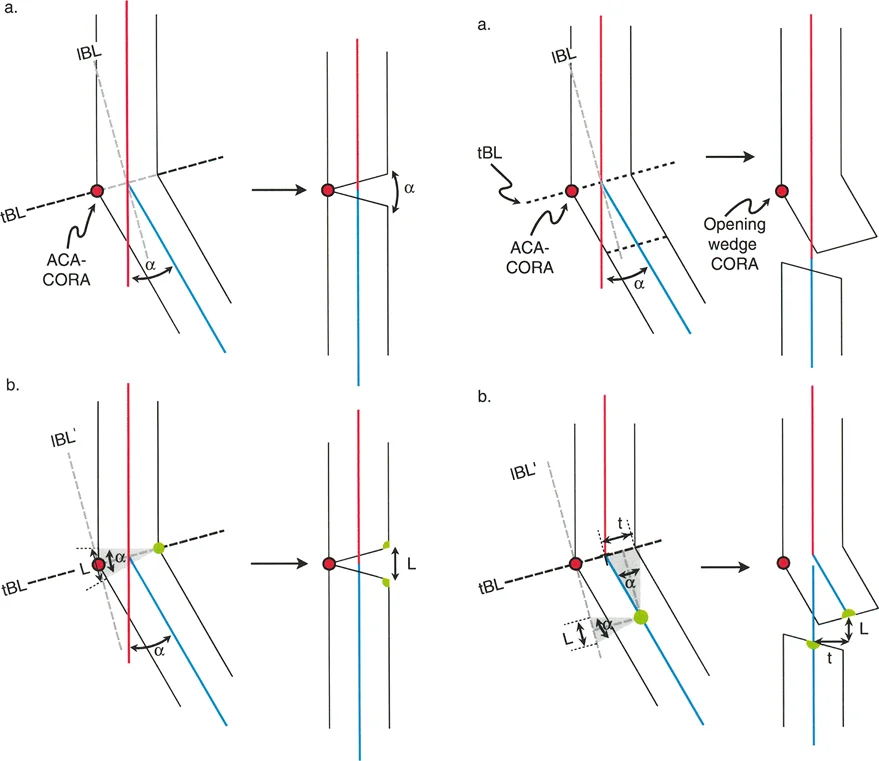
Dr. Paley outlined three fundamental osteotomy rules that dictate how a bone will behave based on where the cut is made relative to the CORA.
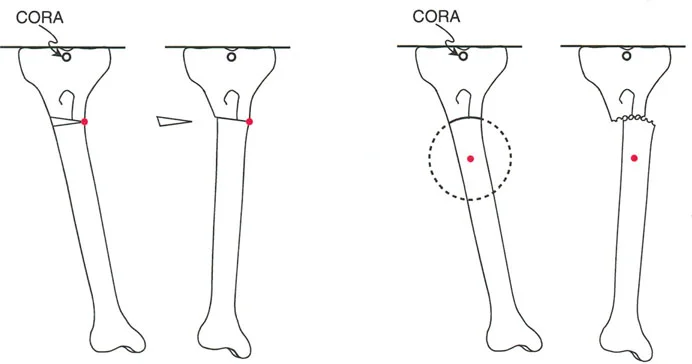
Osteotomy Rule 1
When the osteotomy line passes directly through the CORA, the bone can be angulated to correct the deformity without any translation. The mechanical axis will be perfectly realigned. In the context of knee joint line deformity, this requires an intra articular osteotomy, such as elevating a depressed tibial plateau directly at the site of the defect.

Osteotomy Rule 2
When the osteotomy line is placed away from the CORA (e.g., a metaphyseal High Tibial Osteotomy for an intra articular deformity), the bone must be both angulated and translated to realign the mechanical axis. If the surgeon only angulates the bone without translating it, the mechanical axis will remain deviated.
Osteotomy Rule 3
When the osteotomy line is placed away from the CORA, and the bone is angulated without translation, a secondary translation deformity is created. This results in a zig zag deformity of the bone. While the overall mechanical axis of the limb might appear straight from hip to ankle, the local joint mechanics are severely compromised, leading to abnormal shear forces.
Surgical Execution and Osteotomy Techniques
Once the preoperative planning is complete, the CORA is identified, and the JLCA is accounted for, the surgeon must select the appropriate surgical technique. The choice between an intra articular and an extra articular approach depends on the magnitude of the joint line deformity, the quality of the remaining cartilage, and the patient demographic.
Intra Articular Osteotomy for Plateau Depression
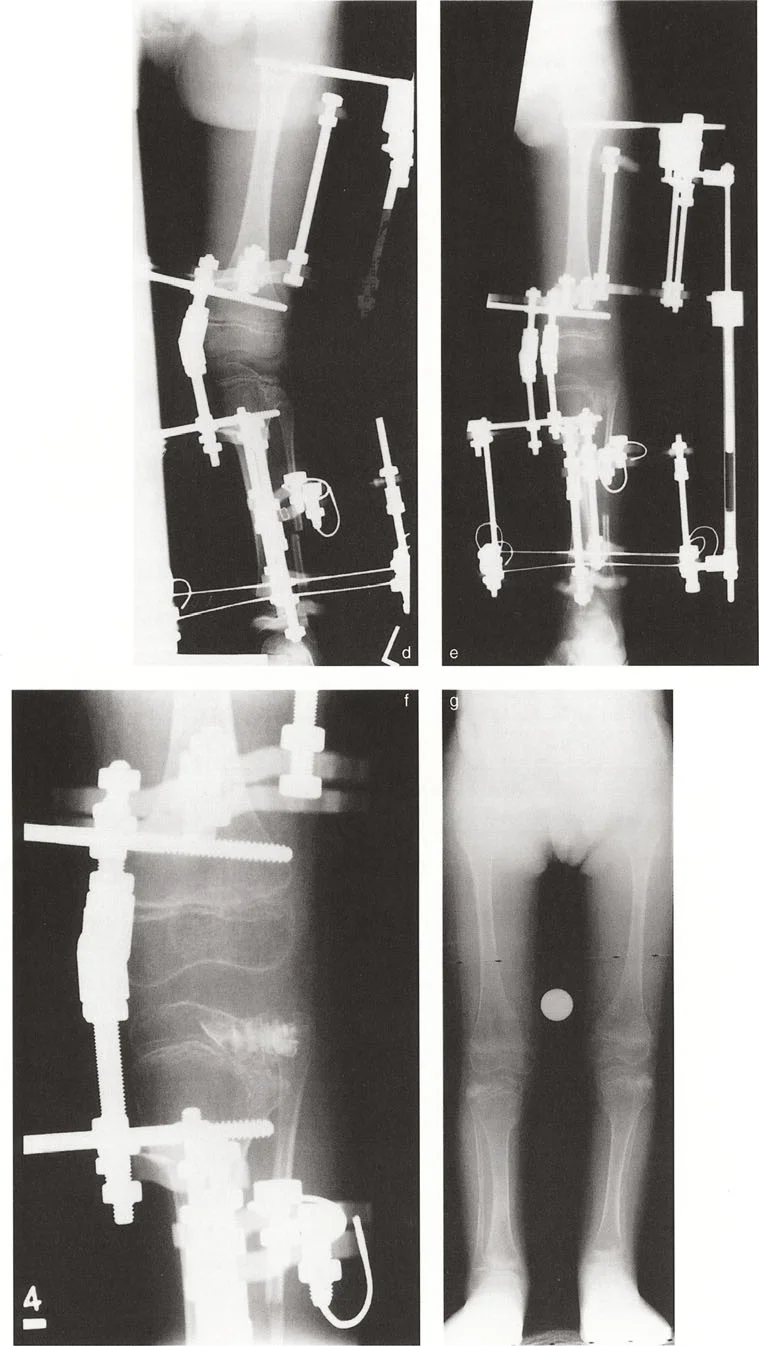
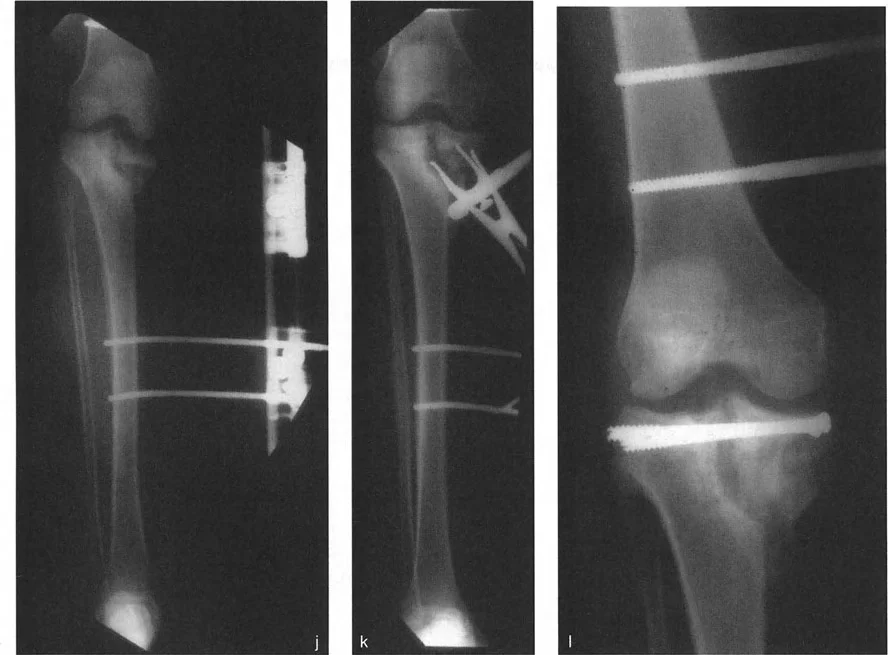
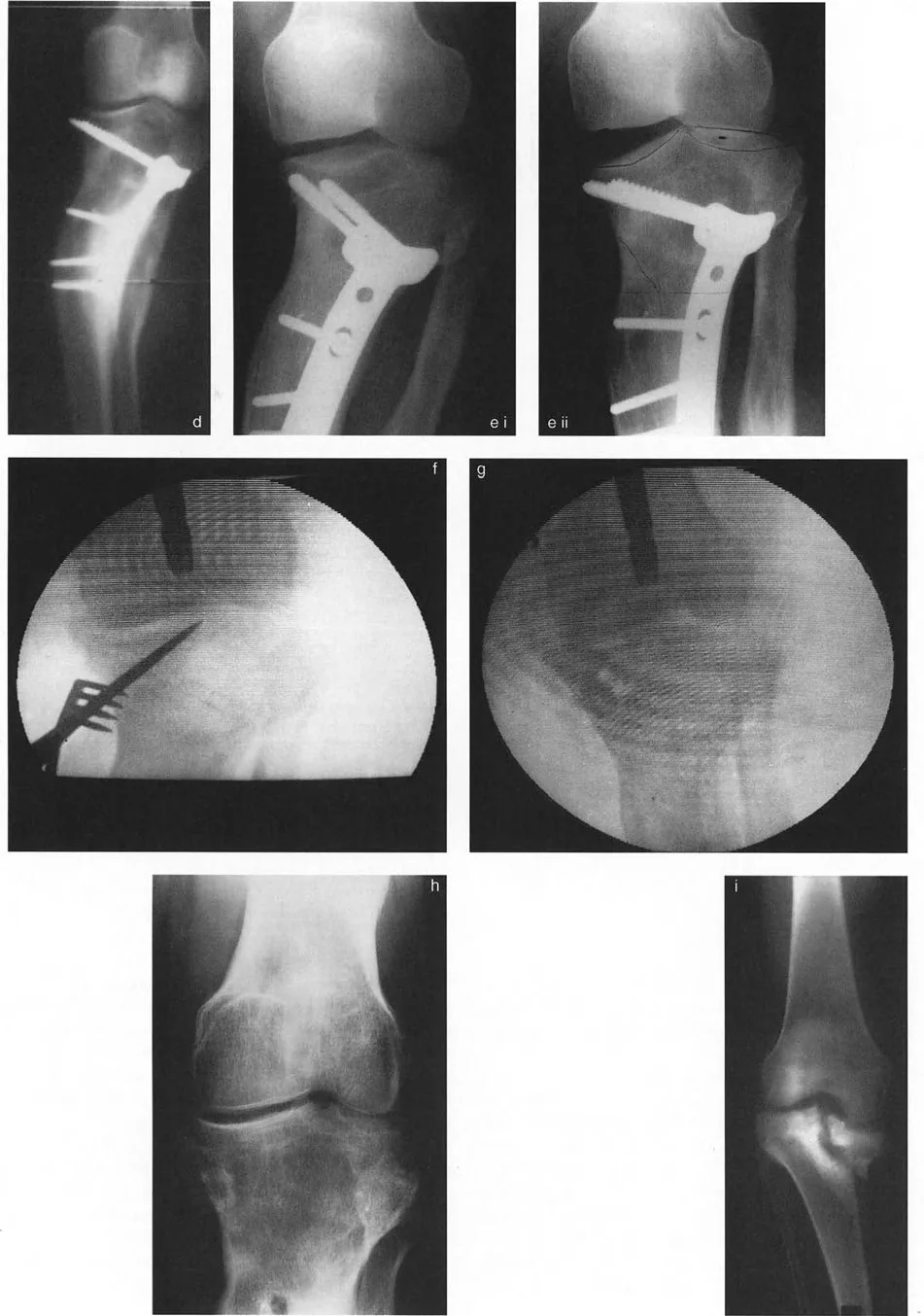
When the joint line deformity is strictly due to a localized bony depression, such as a malunited Schatzker IV tibial plateau fracture or severe Blounts disease, an intra articular osteotomy is the most anatomical solution.
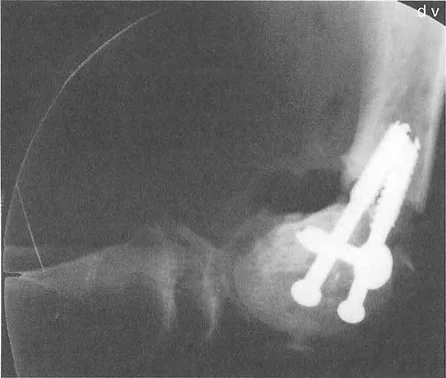
This technique adheres to Paley Osteotomy Rule 1. The surgeon approaches the joint, performs an osteotomy directly beneath the depressed articular segment, and elevates the cartilage and subchondral bone back to a congruent level. The resulting void is filled with structural bone graft or orthobiologics, and the segment is stabilized with rigid internal fixation.
By correcting the deformity directly at the CORA, the JLCA is restored to normal, and the mechanical axis is corrected without requiring metaphyseal translation.
Extra Articular Metaphyseal Osteotomy Compensations
In cases where an intra articular osteotomy is not feasible, such as diffuse asymmetric cartilage loss from advanced osteoarthritis, surgeons rely on extra articular metaphyseal osteotomies. The most common procedures are the High Tibial Osteotomy and the Distal Femoral Osteotomy.

Because the CORA is located in the joint space, but the osteotomy is performed in the metaphysis, the surgeon is operating under Paley Osteotomy Rule 2.
To execute this correctly, the surgeon must overcorrect the metaphyseal angle to compensate for the intra articular wedge caused by the abnormal JLCA. For example, if a patient has 5 degrees of varus from a metaphyseal deformity and an additional 3 degrees of varus from medial cartilage loss (an abnormal JLCA), a standard High Tibial Osteotomy must correct a total of 8 degrees.
Furthermore, because the cut is away from the CORA, the distal bone segment must be translated slightly to ensure the mechanical axis line falls precisely through the desired coordinate of the knee joint (typically the Fujisawa point for medial compartment osteoarthritis).
Clinical Pearls for Deformity Correction Surgeons
Mastering knee joint line deformity requires a synthesis of advanced biomechanics and meticulous surgical execution. Below are high yield clinical pearls for the deformity correction surgeon.
- Never Trust a Standing AP Radiograph Alone: Standard weight bearing films will mask the difference between cartilage loss and ligamentous laxity. Always obtain stress radiographs under fluoroscopy.
- Account for the JLCA: Failing to incorporate an abnormal JLCA into the total angular correction is the most common cause of under correction in High Tibial Osteotomies.
- Master Joint Line Substitution: When a joint surface is unreadable due to severe destruction, immediately look to the opposing healthy joint line and transpose it. This is your most reliable reference.
- Respect the Rules of Osteotomy: If you are cutting away from the CORA, you must plan for translation. Angulation alone away from the CORA guarantees a secondary translation deformity.
- Assess the Sagittal Plane: While this masterclass focuses on the coronal plane, knee joint line deformities often possess a sagittal component, such as an abnormal posterior tibial slope. Always evaluate orthogonal planes.
- Protect the Hinge: During an opening wedge metaphyseal osteotomy, the location of the hinge pin dictates the trajectory of the correction. Ensure the hinge is positioned accurately to prevent unwanted alterations in joint line obliquity.
Conclusion and Future Directions in Joint Preservation
Mastering knee joint line deformity is a testament to an orthopedic surgeons dedication to precise, biomechanically sound joint preservation. By moving beyond simple diaphyseal measurements and truly understanding the nuances of the Joint Line Congruency Angle, surgeons can execute corrections that not only straighten the limb but restore congruent, frictionless joint mechanics.
The application of Dr. Dror Paleys principles, specifically the Rule of Joint Line Substitution and the strict adherence to the Center of Rotation of Angulation, provides a foolproof algorithmic approach to even the most daunting intra articular deformities.
As the field of orthopedic surgery advances, the integration of three dimensional preoperative planning software, patient specific cutting guides, and robotic assistance will further refine our ability to execute these complex corrections. However, technology is only as effective as the surgeons understanding of the underlying biomechanics. By internalizing the concepts detailed in this masterclass, surgeons will be fully equipped to tackle complex knee joint line deformities, ultimately preserving native joints and profoundly improving patient outcomes.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like