Paley's Principles: Mastering Angulation-Translation Deformity Correction
Key Takeaway
Angulation-translation deformities involve bone segments that are both tilted and shifted. Paley's principles provide a systemic approach for correction, utilizing biomechanical analysis, CORA identification, and specific osteotomy rules to restore mechanical axis, joint kinematics, and prevent long-term complications like osteoarthritis.
Introduction to Complex Angulation Translation Deformity Correction
In the specialized realm of orthopedic surgery, correcting bone deformities is rarely as simple as addressing a single-plane bend. Trauma, congenital anomalies, and metabolic bone diseases frequently result in multi-planar deformities that challenge even the most experienced surgeons. Among the most complex and biomechanically demanding of these are angulation translation deformities.
An angulation translation deformity occurs when a bone segment is both tilted and shifted relative to its adjacent segment. These deformities typically arise from fractures that have healed in a displaced and angulated position, resulting in a malunion, or from nonunions where the bone ends have shifted over time due to asymmetric loading and muscular pull. Furthermore, congenital conditions such as fibular hemimelia or acquired conditions like severe Blount disease can present with profound combined deformities.
Understanding the relationship between angulation and translation is not merely an academic exercise. It is an absolute prerequisite for restoring normal biomechanics, joint kinematics, and aesthetic appearance. Uncorrected translation can lead to eccentric joint loading, while uncorrected angulation alters the mechanical axis, inevitably leading to premature osteoarthritis. As an AI Medical Education expert specializing in advanced orthopedics, I will guide you through a highly exhaustive, masterclass-level exploration of the biomechanics, preoperative planning, and surgical strategies required to master these complex corrections. This comprehensive guide is heavily rooted in the foundational principles established by Dr. Dror Paley, whose systemic approach to deformity analysis revolutionized modern orthopedic surgery.
Foundational Biomechanics in Orthopedic Deformity Analysis
Before diving into the surgical strategies for combined deformities, the orthopedic surgeon must establish a rigorous understanding of the foundational concepts of deformity analysis. Paley's principles provide a universal language and a mathematical framework for dissecting any lower extremity deformity, regardless of its complexity.
Understanding Mechanical Axis Deviation
The mechanical axis of the lower extremity is a straight line drawn from the center of the femoral head to the center of the ankle joint at the tibial plafond. In a normally aligned, physiologically sound limb, this line passes slightly medial to the center of the knee joint, typically measuring roughly eight millimeters medial to the exact center of the tibial plateau.
Mechanical Axis Deviation occurs when this weight-bearing line falls outside the normal physiological range. A shift medially indicates a varus deformity, increasing the compressive forces on the medial compartment of the knee and stretching the lateral collateral ligament complex. Conversely, a lateral shift indicates a valgus deformity, overloading the lateral compartment. Correcting Mechanical Axis Deviation is the primary, non-negotiable goal of deformity surgery. Uncorrected deviation leads to asymmetric cartilage wear, subchondral sclerosis, and eventual joint destruction requiring arthroplasty.
Standard Joint Orientation Angles
To determine precisely where a deformity originates within a long bone, surgeons rely on specific joint orientation angles. These angles are measured between the mechanical or anatomical axes of the bones and their respective joint lines. By comparing a patient's measurements to standardized population norms, the surgeon can isolate the deformity to the femur, the tibia, or both.
Key angles evaluated in the coronal plane include the Mechanical Lateral Distal Femoral Angle, the Mechanical Proximal Tibial Angle, and the Lateral Distal Tibial Angle. Accurate measurement of these angles requires high-quality, full-length, weight-bearing standing radiographs with the patellae oriented strictly forward to eliminate rotational artifact.
Table of Normal Joint Orientation Angles
Below is a high-yield reference table summarizing the standard joint orientation angles crucial for preoperative planning based on Paley's normative data.
| Angle Designation | Full Name | Normal Value Range | Clinical Significance |
|---|---|---|---|
| mLDFA | Mechanical Lateral Distal Femoral Angle | 85° - 90° (Avg 87°) | Evaluates distal femoral varus/valgus |
| mLPFA | Mechanical Lateral Proximal Femoral Angle | 85° - 95° (Avg 90°) | Evaluates proximal femoral alignment |
| MPTA | Mechanical Proximal Tibial Angle | 85° - 90° (Avg 87°) | Evaluates proximal tibial varus/valgus |
| LDTA | Lateral Distal Tibial Angle | 86° - 92° (Avg 89°) | Evaluates distal tibia at the ankle joint |
| JLCA | Joint Line Convergence Angle | 0° - 2° | Differentiates intra-articular laxity from bony deformity |
The Center of Rotation of Angulation Concept
The Center of Rotation of Angulation is the fundamental, unifying concept in Paley's deformity analysis. It dictates not only where the deformity is located but also how the surgical correction must be executed to avoid creating secondary deformities.
Defining the CORA in Complex Deformities
The Center of Rotation of Angulation is defined as the point where the proximal mechanical or anatomical axis intersects with the distal mechanical or anatomical axis of a deformed bone.
In a pure angulation deformity, the intersection of these axes lies exactly on the bone at the apex of the deformity. The surgeon can easily identify this point and plan the osteotomy accordingly.
In a pure translation deformity, the proximal and distal axes are perfectly parallel. Because parallel lines never intersect in standard Euclidean geometry, the Center of Rotation of Angulation is theoretically located at infinity.
However, in an angulation translation deformity, the axes do intersect, but the point of intersection may fall completely outside the physical cortex of the bone. This eccentric location creates a unique biomechanical challenge. If the surgeon simply cuts the bone at the level of the fracture or malunion without respecting this eccentric point, the correction will fail to restore the mechanical axis properly.
Paleys Three Osteotomy Rules for Deformity Correction
To correct any skeletal deformity, an osteotomy must be made. The geometric relationship between the osteotomy site, the Center of Rotation of Angulation, and the Axis of Correction of Angulation dictates the physical outcome of the surgery. Paley formalized these relationships into three immutable rules.
Osteotomy Rule One Pure Angulation
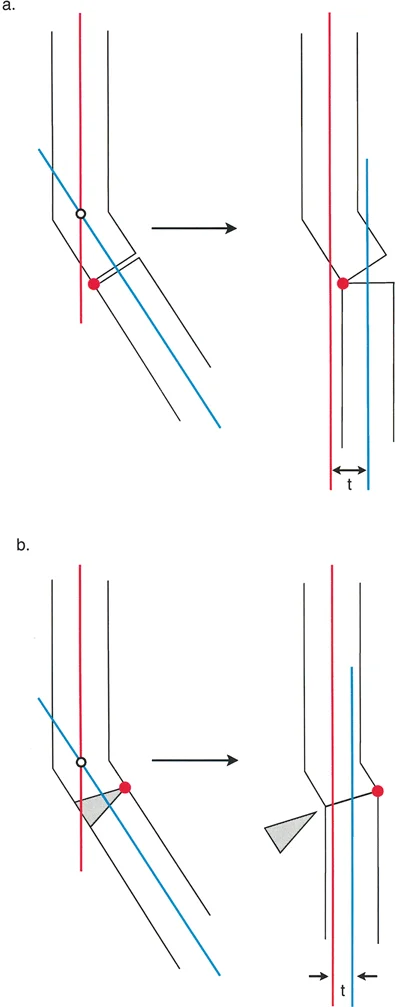
When the osteotomy and the Axis of Correction of Angulation both pass precisely through the Center of Rotation of Angulation, pure angular correction is achieved without introducing any new translation.
In clinical practice, this means the hinge of an external fixator or the pivot point of a closing wedge osteotomy is placed exactly at the apex of the deformity. The bone ends simply rotate around this point. The mechanical axis is restored, and the local bone ends remain in perfect apposition, optimizing the environment for bone healing.
Osteotomy Rule Two Angulation with Induced Translation
When the Axis of Correction of Angulation passes through the Center of Rotation of Angulation, but the actual osteotomy bone cut is performed at a different proximal or distal level, angular correction is achieved, but it simultaneously induces a translation at the osteotomy site.
This rule is the master key for correcting pre-existing angulation translation deformities. If a patient presents with a bone that is both angulated and translated, the surgeon calculates the eccentric Center of Rotation of Angulation. By placing the hinge at this eccentric point and performing the osteotomy at the anatomical axis of the bone, the induced translation perfectly cancels out the pre-existing translation. The result is a straight bone with restored mechanical alignment.
Osteotomy Rule Three Creating Secondary Translation
When the osteotomy and the Axis of Correction of Angulation are both placed away from the Center of Rotation of Angulation, a new, secondary translation deformity is created.
While this sounds like an error, it is occasionally utilized intentionally by advanced deformity surgeons. For example, if the soft tissue envelope at the true apex of the deformity is severely compromised due to previous trauma or infection, the surgeon may elect to perform the osteotomy in healthy tissue away from the apex. By intentionally utilizing Rule Three, the surgeon accepts a local translation at the bone cut to achieve a perfectly straight overall mechanical axis.
Three Dimensional Visualization and Oblique Plane Deformities
Bones exist in three-dimensional space, and deformities rarely respect the neat, orthogonal boundaries of standard two-dimensional anterior-posterior and lateral radiographs. A comprehensive understanding of spatial geometry is required to master these corrections.
Calculating the True Deformity Vector
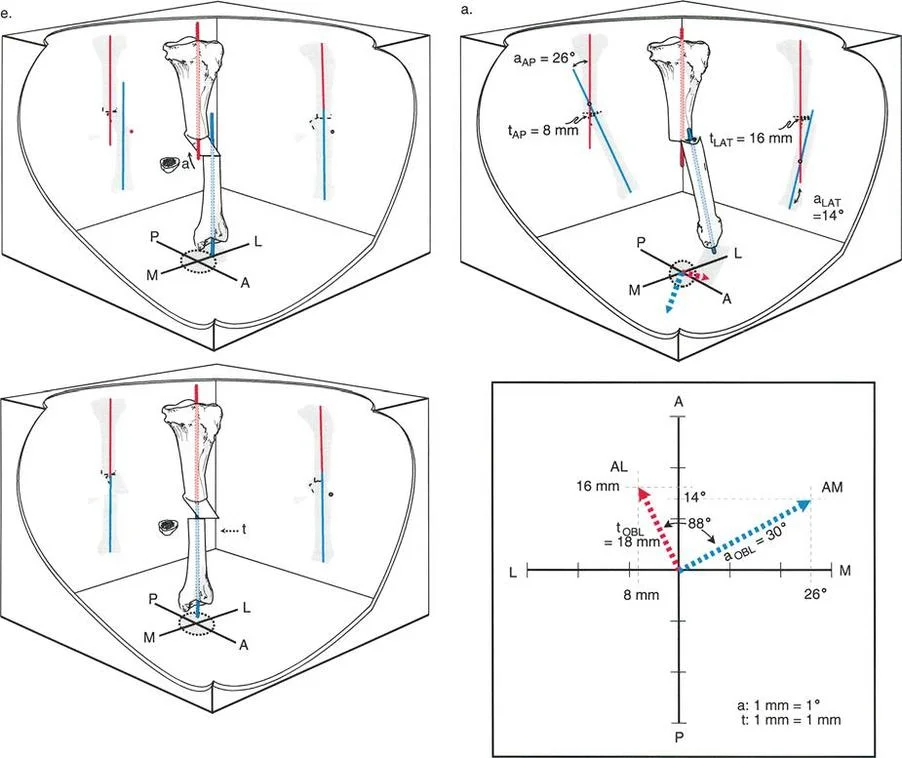
When a bone is angulated in the coronal plane and simultaneously angulated in the sagittal plane, the true deformity does not exist purely in either of those planes. Instead, it exists in an oblique plane rotated somewhere between the two.
To properly plan a surgical correction, the orthopedic surgeon must calculate the true magnitude and the exact direction of the deformity in this oblique plane. This requires vector addition and a solid grasp of trigonometry.
If we define the anterior-posterior angulation as $a_{AP}$ and the lateral angulation as $a_{LAT}$, the true oblique plane angulation magnitude $a_{OBL}$ is calculated using the Pythagorean theorem:
$a_{OBL} = \sqrt{(a_{AP})^2 + (a_{LAT})^2}$
Similarly, the axis of the oblique plane, which dictates the rotational direction of the apex, is found using the tangent function:
$Tan(\theta) = a_{AP} / a_{LAT}$
The exact same mathematical principles apply to translation. If there is translation in the coronal plane defined as $t_{AP}$ and translation in the sagittal plane defined as $t_{LAT}$, the true oblique translation $t_{OBL}$ is the vector sum of both components.
As illustrated in the vector graph above, we see a precise plotting of these forces. The graph meticulously maps the anterior-posterior and medial-lateral axes.
* The lateral translation ($t_{LAT}$) is measured at 16 mm, and the AP translation ($t_{AP}$) is 8 mm.
* The lateral angulation ($a_{LAT}$) is 14°, and the AP angulation ($a_{AP}$) is 26°.
* By plotting these vectors mathematically, the true oblique plane angulation ($a_{OBL}$) is revealed to be exactly 30°, and the true oblique translation ($t_{OBL}$) can be similarly derived.
This vector analysis is the foundation of modern hexapod circular external fixation software, such as the Taylor Spatial Frame, which requires precise input of these orthogonal measurements to generate a six-axis correction schedule.
Trigonometry in Preoperative Planning
Failing to account for the oblique plane leads to incomplete corrections. If a surgeon only corrects the coronal varus deformity using a standard opening wedge high tibial osteotomy but ignores the accompanying sagittal plane recurvatum, the mechanical axis will remain abnormal, and the joint will continue to experience pathological shear forces. By calculating the oblique plane, a single, precise, single-cut osteotomy can be executed that simultaneously corrects both planes of angulation.
Surgical Strategies for Angulation Translation Deformities
Addressing combined deformities surgically requires meticulous execution. The choice of fixation whether internal plating, intramedullary nailing, or circular external fixation depends on the magnitude of the deformity, the quality of the soft tissues, and the presence of any leg length discrepancy.
Translating the Osteotomy Site
When addressing an angulation translation deformity with internal fixation, the surgeon must physically translate the bone fragments at the osteotomy site. For example, if a femur is healed in 15 degrees of varus and 10 millimeters of medial translation, a standard closing wedge osteotomy will correct the varus but leave the translation intact.
To achieve full correction, the surgeon must perform the osteotomy, angulate the distal segment 15 degrees into valgus, and physically slide the distal segment 10 millimeters laterally. This maneuver requires extensive soft tissue release and is often stabilized using a blade plate or a locking compression plate.
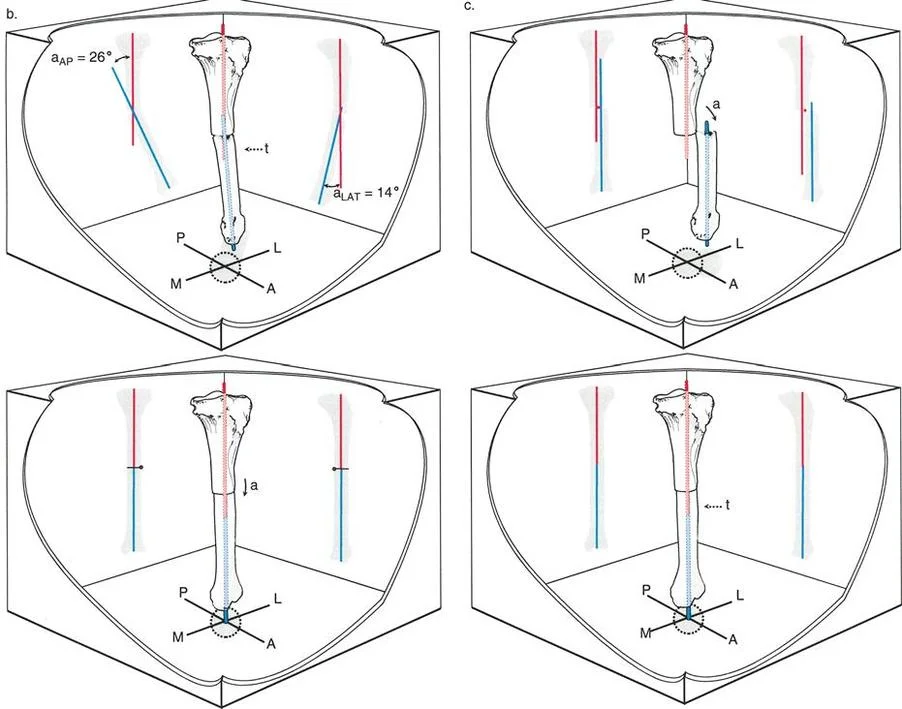
Using Rule Two for Combined Deformities
When utilizing circular external fixation, Osteotomy Rule Two is the most elegant solution for angulation translation deformities. By building the frame so that the mechanical hinges intersect exactly at the eccentric Center of Rotation of Angulation, the surgeon can perform a simple transverse osteotomy through the anatomical axis.
As the hinges are turned postoperatively during the distraction osteogenesis phase, the distal bone segment swings along an arc dictated by the eccentric hinge. This arc simultaneously corrects the angular deformity while inducing a translation that perfectly opposes and neutralizes the pre-existing translation. This technique minimizes acute stretching of neurovascular structures and allows for infinite micro-adjustments during the consolidation phase.
Step by Step Preoperative Planning Protocol
Mastery of deformity correction requires a disciplined, reproducible approach to preoperative planning. The following protocol should be executed for every complex lower extremity deformity.
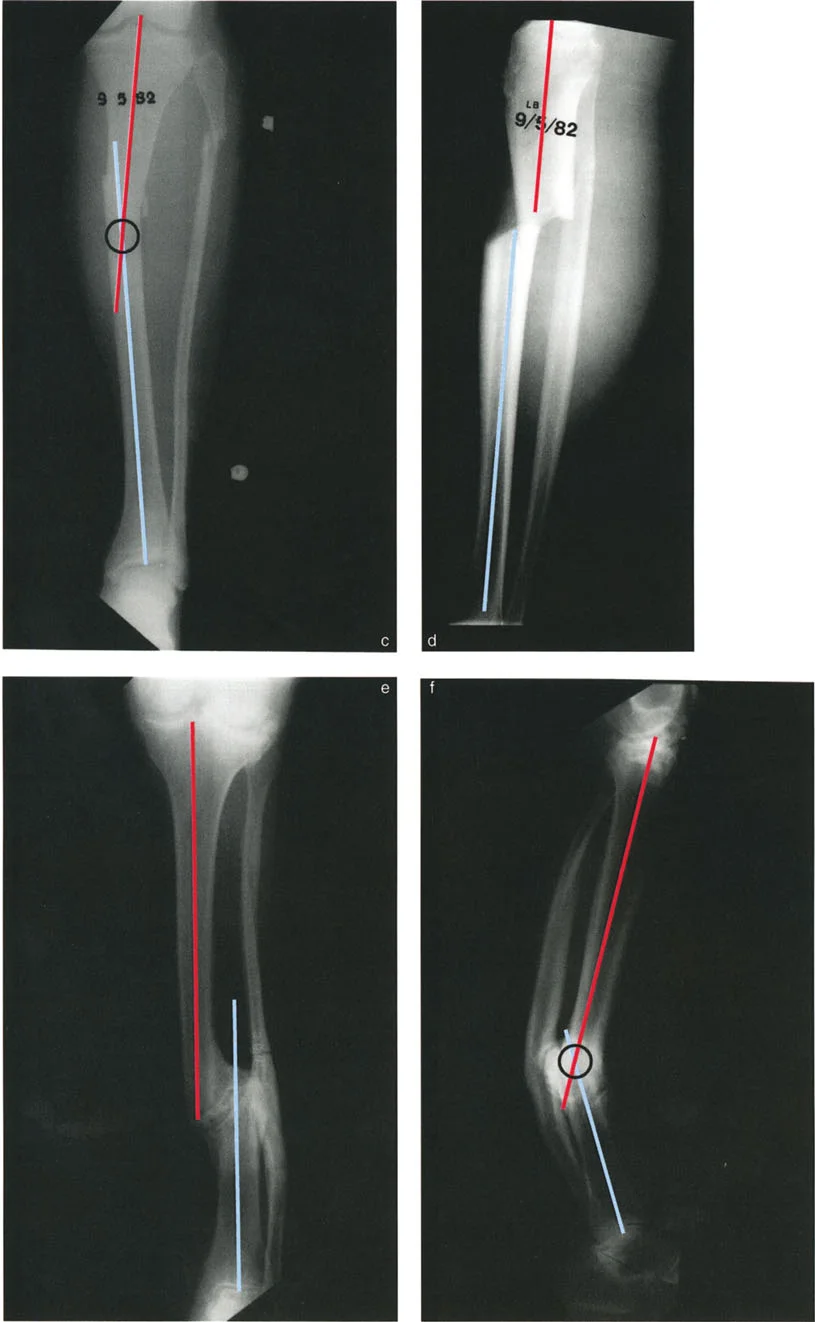
Step One Full Length Radiographic Evaluation
Obtain a 51-inch standing anterior-posterior radiograph of both lower extremities. The patellae must be facing strictly forward. Obtain a dedicated full-length lateral radiograph of the affected extremity. Ensure the magnification marker is visible to allow for accurate digital calibration.
Step Two Joint Orientation Angle Measurement
Draw the mechanical axis of the entire limb to calculate the Mechanical Axis Deviation. Next, draw the mechanical and anatomical axes of the individual femur and tibia. Measure the mLDFA, MPTA, and LDTA. Compare these values to the contralateral normal limb and established population norms to isolate the specific bone and level responsible for the deformity. Evaluate the Joint Line Convergence Angle to rule out ligamentous laxity as the primary cause of the deviation.
Step Three CORA Identification and Rule Selection
Draw the proximal axis line and the distal axis line of the deformed bone. Mark their intersection to identify the Center of Rotation of Angulation. Evaluate if the deformity is purely angular, purely translational, or combined.
If it is an angulation translation deformity, the intersection will lie outside the bone. Decide on the osteotomy level based on bone quality and soft tissue coverage. Select the appropriate Paley Osteotomy Rule to achieve the desired correction. Finally, calculate the oblique plane vectors to ensure all three dimensions are addressed in the surgical plan.
Clinical Pearls for the Orthopedic Surgeon
To elevate your clinical practice and optimize patient outcomes, internalize the following high-yield surgical pearls regarding angulation translation deformities.
High Yield Takeaways for Board Preparation
- Always Check the Sagittal Plane: A deformity that appears as a simple varus bow on an AP radiograph often harbors a hidden procurvatum or recurvatum component. Always calculate the oblique plane vector.
- Beware the Eccentric CORA: In combined angulation translation deformities, the intersection of the proximal and distal axes will rarely lie on the anatomical bone. Cutting the bone at the apex without translating the fragments will result in a persistent mechanical axis deviation.
- Rule Two is the Workhorse: Paley's Rule Two is the most powerful tool for correcting combined deformities without requiring complex, multi-level bone cuts. Master hinge placement at the eccentric Center of Rotation of Angulation.
- Soft Tissue Dictates the Cut: While mathematical planning may dictate an osteotomy at a specific level, severe scarring, poor skin flaps, or active infection may force you to alter your plan. Utilize Rule Three to move the osteotomy into healthy tissue, accepting the induced translation to achieve overall mechanical alignment.
- Account for the Joint Line: The Joint Line Convergence Angle must be factored into your planning. If a patient has a varus deformity driven by a 4-degree JLCA due to lateral ligamentous laxity, overcorrecting the bony anatomy will lead to joint instability.
Conclusion to Advanced Deformity Correction Strategies
Mastering angulation translation deformities represents the pinnacle of orthopedic deformity correction. It requires a seamless integration of biomechanical theory, spatial geometry, and meticulous surgical execution. By rigorously applying Dr. Dror Paley's principles—specifically the rigorous identification of the Center of Rotation of Angulation and the disciplined application of the Three Osteotomy Rules—surgeons can reliably restore the mechanical axis, optimize joint kinematics, and profoundly improve the quality of life for patients suffering from complex multi-planar deformities.
Through exhaustive preoperative planning, precise vector analysis of the oblique plane, and careful selection of fixation modalities, the modern orthopedic surgeon can transform seemingly insurmountable skeletal distortions into predictable, successful clinical outcomes. Continuous study, radiographic templating, and adherence to these foundational biomechanical laws are the hallmarks of a master deformity surgeon.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like