Paley's Principles: Mastering Angulation-Translation Deformity Correction
Key Takeaway
Angulation-translation deformities involve bone segments that are both angulated and shifted, posing multiplanar challenges. Paley's principles offer a systematic, geometric approach to accurately analyze and correct these complex deformities. This method ensures precise measurement, restores the mechanical axis, and prevents iatrogenic complications, leading to superior clinical outcomes.
Introduction to Complex Deformity Correction
In the realm of advanced orthopedic surgery and limb reconstruction, isolated angular deformities or pure translation deformities are relatively straightforward to conceptualize and correct. However, clinical reality rarely presents itself in such simple terms. When dealing with post traumatic malunions, complex nonunions, and severe congenital anomalies, surgeons are most frequently confronted with Angulation Translation Deformities. In these complex scenarios, the bone segments are both angulated and shifted out of their normal anatomical axes, creating a multiplanar challenge that defies basic osteotomy techniques.
Understanding the spatial and special interrelationships between angulation and translation is the absolute cornerstone of modern deformity correction. Pioneered by Dr Dror Paley, the systematic analysis of these combined deformities relies on strict geometric principles. Without a rigorous, mathematically sound approach to radiographic analysis, surgeons risk performing osteotomies at the incorrect level. This surgical error inevitably leads to secondary iatrogenic translation, worsening of the mechanical axis, altered joint contact forces, and ultimately, poor clinical outcomes such as early onset osteoarthritis.
When angulation and translation occur simultaneously, they can easily mimic other types of deformities. For example, a diaphyseal malunion with a combined angulation translation deformity might look radiographically identical to a pure angular deformity that has a completely different apex. If the surgeon simply targets the apparent apex without mapping the true axes, the resulting correction will fail to restore the mechanical axis of the limb.
This comprehensive masterclass deconstructs the advanced principles of deformity analysis, transforming foundational biomechanical concepts into a high yield, clinically applicable guide for orthopedic surgeons. We will explore how to accurately measure these complex deformities, how they interact to affect the mechanical axis, and how to graphically analyze same plane deformities to execute flawless surgical corrections.
Foundational Principles of Paley Deformity Analysis
To master complex limb reconstruction, the surgeon must first internalize the geometric language of deformity. The Paley method removes the guesswork from orthopedic surgery by replacing subjective visual estimation with objective mathematical modeling.
Center of Rotation of Angulation
The Center of Rotation of Angulation represents the exact point where the proximal and distal anatomical or mechanical axes of a deformed bone intersect. Identifying the Center of Rotation of Angulation is the first and most critical step in preoperative planning. In a pure angular deformity, this point typically lies directly on the bone at the apex of the deformity.
However, in an Angulation Translation Deformity, the presence of translation shifts the intersection of these axes. The true Center of Rotation of Angulation may lie completely outside the bone profile. Recognizing this spatial shift is essential because the location of the osteotomy relative to the Center of Rotation of Angulation dictates the final alignment of the bone segments.
Mechanical Axis Deviation and Joint Orientation
The ultimate goal of lower extremity deformity correction is the precise restoration of the normal mechanical axis and joint kinematics. The mechanical axis of the lower limb is defined as a straight line drawn from the center of the femoral head to the center of the ankle joint. In a normal, well aligned limb, this line passes just medial to the center of the knee joint, specifically through the medial tibial spine.
Mechanical Axis Deviation is defined as the perpendicular distance from the center of the knee joint to this mechanical axis line. Any deviation alters the load bearing mechanics of the knee, predisposing the patient to compartmental overload and cartilage degradation.
To ensure the mechanical axis is restored properly, surgeons must evaluate the Joint Orientation Angles. These angles define the relationship between the anatomical or mechanical axes of the bones and the articular surfaces of the joints.
| Joint Orientation Angle | Abbreviation | Normal Range | Average Value |
|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85 to 90 degrees | 87 degrees |
| Mechanical Medial Proximal Tibial Angle | MPTA | 85 to 90 degrees | 87 degrees |
| Mechanical Lateral Distal Tibial Angle | mLDTA | 86 to 92 degrees | 89 degrees |
| Joint Line Convergence Angle | JLCA | 0 to 2 degrees | 1 degree |
Surgical Pearls for Joint Orientation
* Always assess the Joint Line Convergence Angle before planning a femoral or tibial osteotomy. A widened Joint Line Convergence Angle indicates ligamentous laxity or cartilage loss, which will affect your final mechanical axis even if the bone deformity is perfectly corrected.
* When bilateral deformities are present, do not use the contralateral limb as a template. Rely strictly on the established population norms for Joint Orientation Angles.
* The anatomical axis of the femur is typically 7 degrees valgus relative to the mechanical axis, whereas the anatomical and mechanical axes of the tibia are essentially parallel.
Radiographic Evaluation for Angulation Translation Deformities
Accurate preoperative planning is entirely dependent on the quality of the radiographic imaging. Standard short cassette radiographs are insufficient for complex deformity analysis.
Surgeons must obtain 51 inch full length standing anteroposterior radiographs of both lower extremities. The patellae must be positioned strictly forward to control for rotation, as rotational malalignment will project as a false deformity in the coronal and sagittal planes. Additionally, full length lateral radiographs are required to assess the sagittal plane, as most Angulation Translation Deformities are oblique plane deformities requiring multiplanar correction.
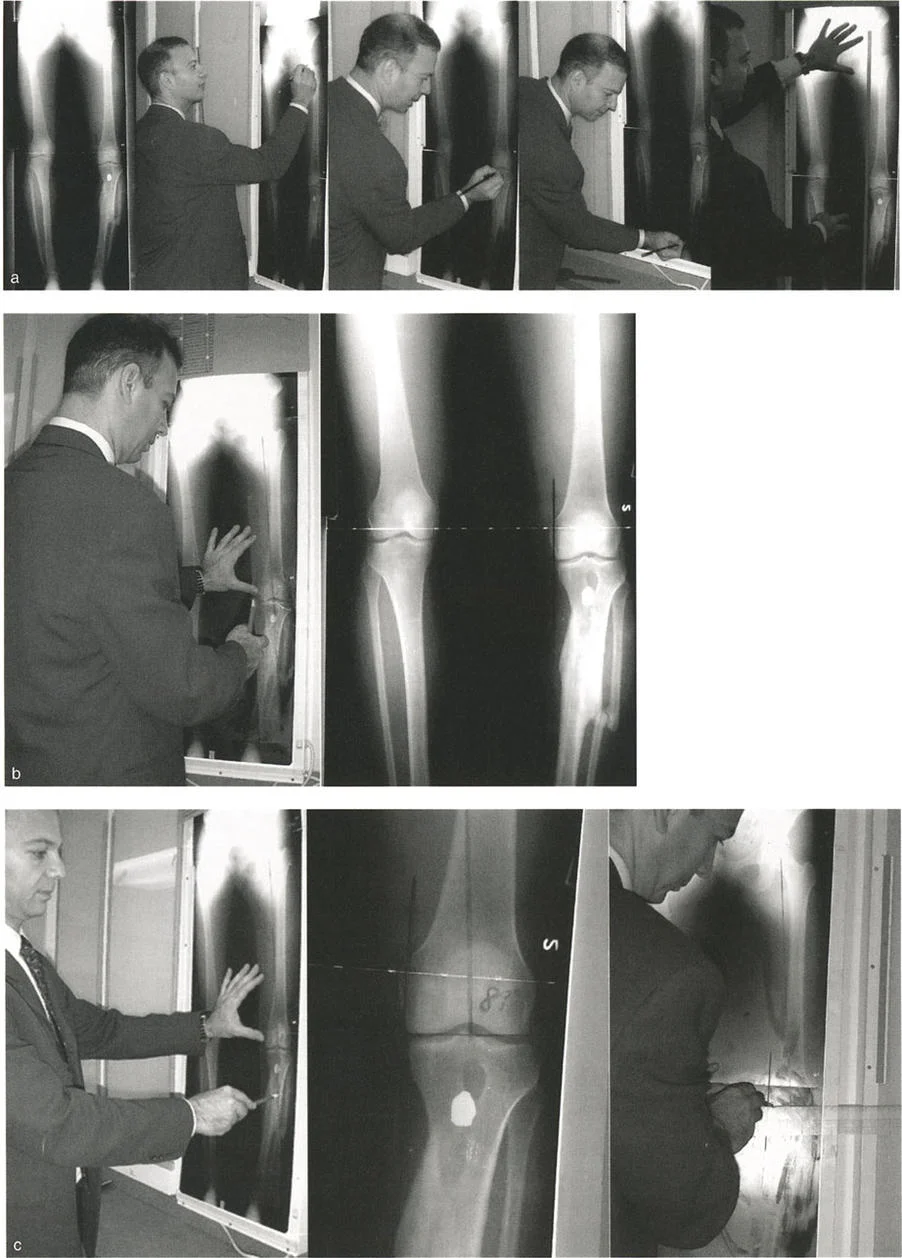
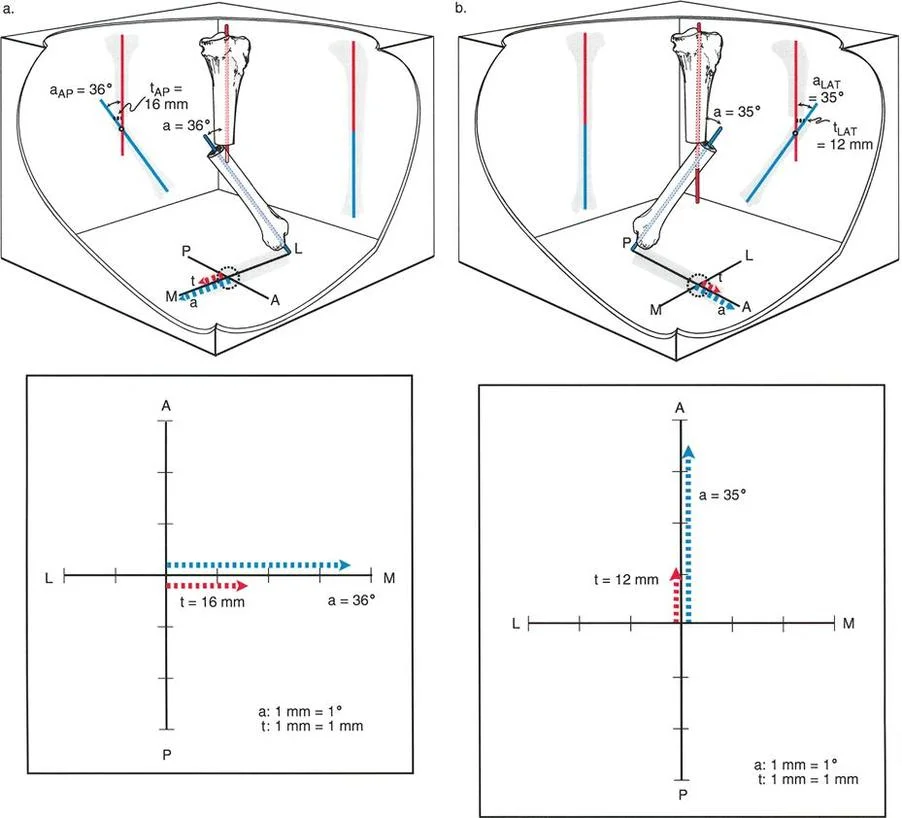
Measuring Translation in the Presence of Angulation
Before a surgeon can correct a combined deformity, they must be able to accurately quantify both the angular and translational components. Measuring pure translation is simple; it is the perpendicular distance between two parallel axis lines. However, when an angular deformity is superimposed on a translation deformity, the axis lines are no longer parallel. They intersect at the Center of Rotation of Angulation.
How do we measure the exact magnitude of translation when the bone segments are angulated? According to Paley principles, there are two primary geometric methods for measuring translation magnitude in the presence of angular deformity. Both methods require drawing the mid diaphyseal axis lines of the proximal and distal bone segments.
The Proximal Reference Method
In this highly reliable approach, the translation is measured as the perpendicular distance from the proximal axis line to the distal axis line. Crucially, this measurement is taken specifically at the level of the proximal end of the distal segment, which typically correlates to the fracture or osteotomy site.
This method is heavily favored in clinical practice, especially when limb shortening is present alongside the deformity. The mathematical advantage of the Proximal Reference Method is that if the shortening is referenced to the proximal axis line, the measured amount of translation remains constant regardless of how much the limb is shortened or lengthened.
By utilizing the proximal segment as a fixed coordinate system, this method proves to be mathematically robust during preoperative planning for distraction osteogenesis or acute lengthening. The surgeon can plan the longitudinal pull without having to constantly recalculate the translational offset.
The Distal Reference Method
Alternatively, translation can be measured using the Distal Reference Method. Here, translation is calculated as the perpendicular distance from the distal axis line to the proximal axis line, measured at the level of the distal end of the proximal bone segment.
While geometrically valid in a static two dimensional drawing, this method introduces a significant confounding variable in clinical practice: limb length. If there is axial shortening, and the surgeon uses the distal axis as the reference point, the measured magnitude of translation will change dynamically depending on the degree of shortening.
This fluctuation occurs because the distal axis is angulated relative to the proximal axis. As you theoretically slide the distal segment proximally to account for shortening, the perpendicular distance between the axes at the fracture site changes. Therefore, the Distal Reference Method is generally discouraged when planning complex reconstructions involving limb lengthening.
Surgical Pearls for Deformity Measurement
* Always default to the Proximal Reference Method when calculating translation in the presence of shortening. It provides a stable, reproducible metric that will not fluctuate as you plan your longitudinal corrections.
* Ensure your axis lines are drawn over a sufficient length of the diaphysis. Drawing short axis lines near the deformity apex will amplify minor drafting errors, leading to massive miscalculations of translation.
* Use digital templating software whenever possible, but maintain the ability to manually draw and calculate these parameters to truly understand the geometry of the deformity.
Mechanical Axis Deviation and Combined Deformities
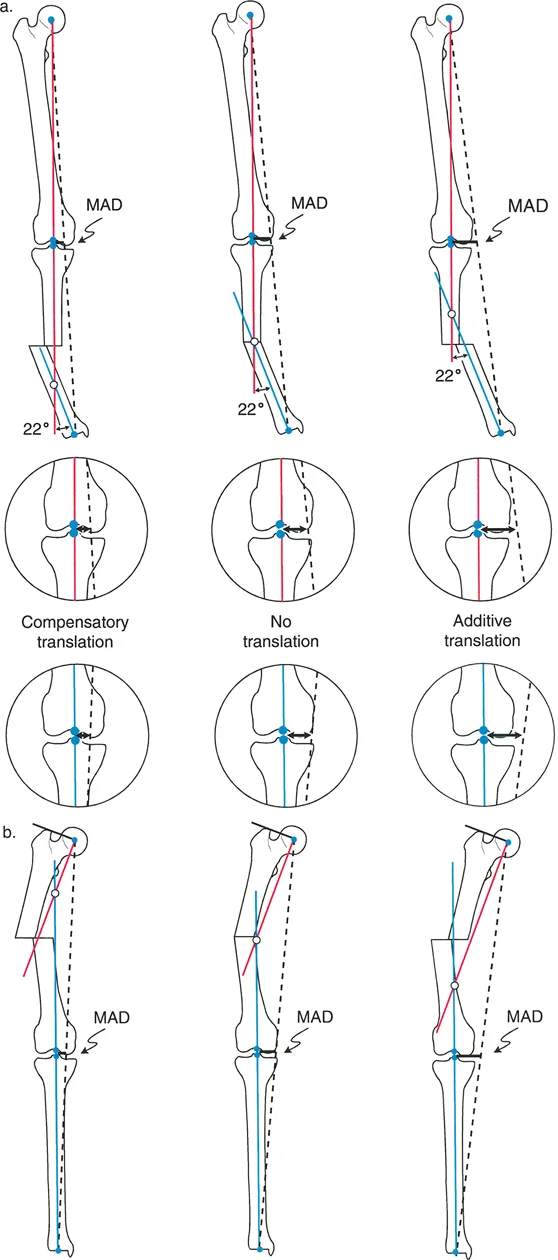
Both angulation and translation independently affect Mechanical Axis Deviation. When they occur together in an Angulation Translation Deformity, their effects on the mechanical axis are not simply additive in a linear sense. Depending on their relative directions, they can either cancel each other out or compound to create a severe, limb threatening deviation. This dynamic interaction is categorized into compensatory translation and additive translation.
Compensatory Translation Biomechanics
Translation is considered compensatory when its anatomical direction counteracts the Mechanical Axis Deviation caused by the angular deformity. In these specific cases, the translation acts as a biomechanical safeguard, pulling the mechanical axis back toward the center of the knee joint.
For example, consider a distal femoral fracture that heals in severe varus angulation. This angulation alone would drive the mechanical axis far medial to the knee joint. However, if the distal femoral segment also translates laterally during the healing process, this lateral translation will shift the knee joint laterally, bringing the center of the knee closer to the mechanical axis line.
In compensatory scenarios, the overall Mechanical Axis Deviation is significantly less than what it would be if the angular deformity existed in isolation. While the bone itself looks highly deformed on a radiograph, the joint kinematics may be surprisingly well preserved. Surgeons must be cautious when correcting compensatory deformities; correcting only the angulation without addressing the translation will unmask a massive mechanical axis deviation.
Additive Translation Biomechanics
Translation is considered additive when its anatomical direction exacerbates the Mechanical Axis Deviation caused by the angular deformity. In these dangerous scenarios, both the angulation and the translation are pushing the mechanical axis in the exact same direction.
Using the previous example of a distal femur in varus, if the distal segment translates medially instead of laterally, the medial translation compounds the varus angulation. Both forces drive the mechanical axis violently medial to the knee joint. This additive effect creates severe varus overload, leading to rapid destruction of the medial compartment articular cartilage, stretching of the lateral collateral ligament, and a pronounced varus thrust during the gait cycle.
Additive translation deformities require urgent surgical intervention, as the exponential increase in joint contact forces will lead to early and irreversible osteoarthritis.
| Deformity Interaction | Effect on Mechanical Axis | Clinical Consequence | Surgical Priority |
|---|---|---|---|
| Compensatory Translation | Reduces expected MAD | Preserved joint mechanics, delayed arthritis | Must correct both components simultaneously to prevent iatrogenic MAD |
| Additive Translation | Exponentially increases MAD | Rapid cartilage wear, severe ligamentous strain | High priority for early intervention to salvage the joint |
Paley Osteotomy Rules for Deformity Correction
The execution of a successful deformity correction relies entirely on where the osteotomy is placed relative to the Center of Rotation of Angulation, and where the Axis of Correction of Angulation is positioned. Dr Paley codified these relationships into three fundamental osteotomy rules. Understanding these rules is mandatory for treating Angulation Translation Deformities.
Paley Osteotomy Rule One
Rule One states that when the osteotomy and the Axis of Correction of Angulation both pass through the exact Center of Rotation of Angulation, the deformity will be corrected by pure angulation. The proximal and distal bone axes will perfectly realign without any secondary translation.
In a pure angular deformity, this is the ideal scenario. However, in an Angulation Translation Deformity, the true Center of Rotation of Angulation is often located outside the bone. You cannot physically perform an osteotomy in empty space. Therefore, Rule One is often impossible to apply directly to the apex of an Angulation Translation Deformity.
Paley Osteotomy Rule Two
Rule Two states that when the osteotomy is performed at a level different from the Center of Rotation of Angulation, but the Axis of Correction of Angulation remains at the Center of Rotation of Angulation, the axes will fully realign. However, the bone ends at the osteotomy site will translate relative to one another.
This is the most critical rule for correcting Angulation Translation Deformities. Because the true Center of Rotation of Angulation is often outside the bone, the surgeon must make the bone cut at a convenient anatomical location (the osteotomy site). By placing the hinge of the external fixator (the Axis of Correction of Angulation) at the true Center of Rotation of Angulation in space, the frame will automatically angulate and translate the bone ends. The axes will perfectly align, but the surgeon must be prepared for the resulting translation at the osteotomy site, ensuring adequate bone contact is maintained for healing.
Paley Osteotomy Rule Three
Rule Three states that when the osteotomy and the Axis of Correction of Angulation are both placed at a level different from the Center of Rotation of Angulation, the deformity will be corrected into a state of parallelism, but the axes will remain translated.
This rule is generally avoided in primary deformity correction because it intentionally creates an iatrogenic translation deformity. However, it is occasionally used deliberately in complex joint realignment surgeries where the surgeon wishes to shift the mechanical axis without altering the joint orientation angles.
Step by Step Preoperative Planning Guide
Mastering the correction of Angulation Translation Deformities requires meticulous preoperative planning. The following step by step algorithm ensures a mathematically sound surgical plan.
- Obtain Quality Imaging: Secure 51 inch standing anteroposterior and full length lateral radiographs. Calibrate the images using a known radiographic marker.
- Draw the Mechanical Axis: Draw a line from the center of the femoral head to the center of the ankle joint. Measure the Mechanical Axis Deviation to quantify the global limb malalignment.
- Perform the Malalignment Test: Identify whether the deviation is originating from the femur, the tibia, or the knee joint itself by evaluating the mechanical axis line relative to the center of the knee.
- Perform the Malorientation Test: Draw the joint reference lines for the proximal femur, distal femur, proximal tibia, and distal tibia. Calculate the mLDFA, MPTA, and mLDTA. Compare these to normal population values to isolate the deformed segment.
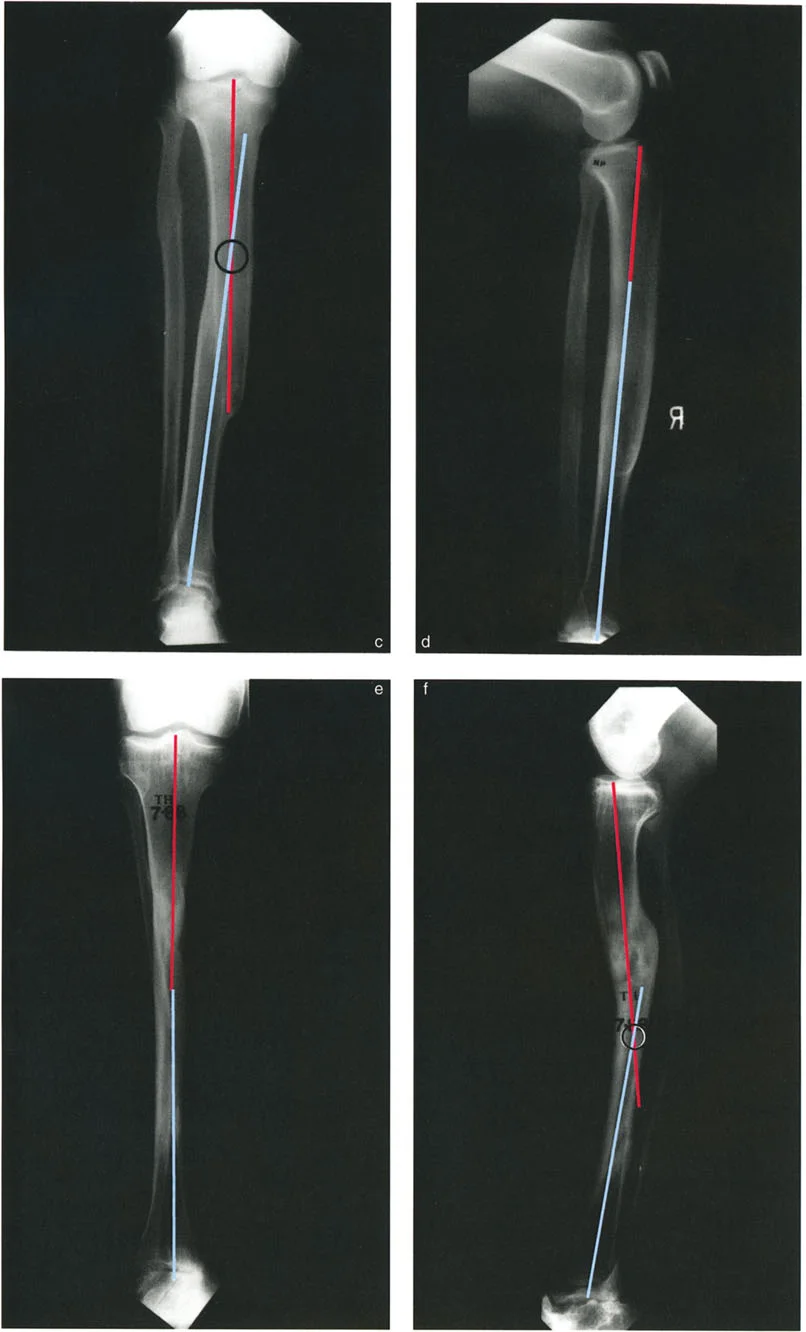
- Draw the Diaphyseal Axes: Draw the mid diaphyseal anatomical axes of the proximal and distal segments of the deformed bone.
- Locate the Center of Rotation of Angulation: Mark the exact point where the proximal and distal axes intersect. In an Angulation Translation Deformity, note how far this point lies outside the anatomical bone profile.
- Measure the Translation: Utilize the Proximal Reference Method to calculate the exact magnitude of translation at the planned osteotomy site.
- Determine the Osteotomy Level: Select an osteotomy site that optimizes bone healing (metaphyseal bone is preferred over diaphyseal bone) and soft tissue coverage.
- Apply the Osteotomy Rules: Plan the placement of your fixator hinge or internal fixation trajectory based on Paley Rule Two, ensuring the Axis of Correction of Angulation is positioned at the true Center of Rotation of Angulation.
Surgical Execution and Fixation Strategies
Once the preoperative plan is mathematically verified, the surgeon must choose the appropriate fixation strategy to execute the correction. The choice between external and internal fixation depends on the magnitude of the deformity, the quality of the soft tissue envelope, and the presence of any active infection or nonunion.
External Fixation Techniques
Circular external fixation, particularly the Taylor Spatial Frame and other hexapod systems, is the gold standard for correcting severe Angulation Translation Deformities. Hexapod frames utilize a virtual hinge, allowing the surgeon to place the Axis of Correction of Angulation exactly at the Center of Rotation of Angulation, even if that point is suspended in space outside the limb.
During surgery, the rings are applied orthogonally to the proximal and distal bone segments. The osteotomy is performed using a minimally invasive Gigli saw or multiple drill hole technique to preserve the periosteal blood supply. Postoperatively, the software program calculates a daily strut adjustment schedule. As the patient turns the struts, the frame simultaneously angulates and translates the bone segments, perfectly executing Paley Rule Two over a period of weeks.
Surgical Pearls for Hexapod Frames
* Mounting parameters must be measured with absolute precision. A small error in measuring the distance from the reference ring to the true Center of Rotation of Angulation will result in residual translation and axis deviation.
* Always account for soft tissue tension. Massive translations can stretch neurovascular structures. A gradual correction via distraction osteogenesis is much safer for the nerves than an acute intraoperative correction.
Internal Fixation Techniques
For milder Angulation Translation Deformities, acute correction followed by internal fixation with plates or intramedullary nails is highly effective.
When using plates, the surgeon can perform a closing wedge, opening wedge, or dome osteotomy. Dome osteotomies are particularly useful for Angulation Translation Deformities because the cylindrical cut allows the bone ends to rotate around a central axis without creating massive cortical steps or gaps.
Intramedullary nailing is technically demanding for these deformities because the rigid path of the nail dictates the final alignment. To achieve correction with a nail, the surgeon must use blocking screws (Poller screws). By strategically placing blocking screws in the concavity of the deformity, the surgeon artificially narrows the medullary canal, forcing the nail to translate the bone segment into the correct anatomical alignment as it is inserted.
Recently, the advent of motorized internal lengthening nails has revolutionized this field. Surgeons can now acutely correct the angulation and translation intraoperatively, stabilize the bone with the magnetic nail, and then gradually lengthen the limb postoperatively to address any associated shortening.
Postoperative Management and Rehabilitation
The success of a complex deformity correction extends far beyond the operating room. Postoperative management is a critical phase of the reconstructive process.
For patients undergoing gradual correction with an external fixator, pin site care is paramount to prevent superficial infections from tracking down to the bone. Physical therapy must begin immediately to maintain joint range of motion. The translation of bone segments can alter the resting length of muscles and tendons, making aggressive stretching protocols necessary to prevent contractures.
Weight bearing status depends on the chosen fixation. Circular frames generally allow for early weight bearing, which stimulates the mechanoreceptors in the regenerate bone, promoting faster consolidation. Internal fixation may require delayed weight bearing depending on the stability of the osteotomy construct.
Frequent radiographic follow up is required. During gradual correction, standing alignment films should be obtained every two weeks to verify that the mechanical axis is tracking toward the center of the knee joint. If the trajectory deviates, the software parameters of the hexapod frame can be adjusted dynamically, a concept known as "residual program generation."
Conclusion and Future Directions
Mastering Angulation Translation Deformities requires a profound shift in how an orthopedic surgeon visualizes the skeletal system. By moving away from subjective visual estimation and embracing the rigorous, mathematically driven Paley principles, surgeons can predictably restore normal biomechanics to the most severely deformed limbs.
The identification of the true Center of Rotation of Angulation, the accurate measurement of translation via the Proximal Reference Method, and the strategic application of the Osteotomy Rules are non negotiable skills for the modern deformity surgeon. As technology advances, the integration of three dimensional preoperative planning software, patient specific 3D printed cutting guides, and augmented reality intraoperative navigation will further refine our ability to execute these complex corrections with millimeter precision. However, these technological tools are only as effective as the surgeon's foundational understanding of the underlying geometry. The principles of mechanical axis restoration remain the immutable bedrock of orthopedic limb reconstruction.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like