Orthopedic Translation Deformities: Definition, Biomechanics, and Surgical Correction
Key Takeaway
Translation deformity is a parallel shift of a distal bone segment relative to its proximal segment without angular change. Caused by fractures or osteotomies, it disrupts bone contact, increases nonunion risk, and significantly impacts limb biomechanics, necessitating precise orthopedic correction.
Comprehensive Introduction to Translation Deformities
Translation deformity represents a fundamental deviation from normal osseous alignment, classically referred to in historical orthopedic literature as ad latus displacement. In the comprehensive analysis of limb deformity, translation is characterized by the parallel shift of the distal bone segment relative to the proximal segment without any alteration in their angular relationship. This distinct biomechanical and geometric entity occurs secondary to traumatic fractures, nonunions, malunions, or iatrogenic displacement following poorly stabilized osteotomies.
By strict orthopedic convention, translation deformity is described based on the displacement of the distal segment relative to the proximal segment. This standardized nomenclature applies universally to the appendicular skeleton, specifically the lower and upper extremities from the level of the femoral and humeral necks extending distally. Mastery of these concepts is the first step in applying the principles of deformity correction pioneered by Dr. Dror Paley, which rely heavily on precise mathematical and geometric definitions of bone segments in space.
Standardized Nomenclature and Clinical Communication
Clear communication between orthopedic surgeons, residents, and musculoskeletal radiologists requires an unwavering adherence to standardized nomenclature. When describing a translation deformity of the tibial diaphysis, for example, a "lateral translation" indicates that the distal tibial segment has shifted laterally relative to the proximal tibial segment. This descriptor dictates the subsequent vectors required for surgical correction. The magnitude of this shift is measured in millimeters, and the plane is defined by orthogonal radiographic projections.
Critical Exceptions in Axial and Articular Anatomy
Critical exceptions to the standard distal-relative-to-proximal rule exist and must be thoroughly understood by the reconstructive surgeon to avoid catastrophic errors in preoperative templating. In the axial skeleton, specifically the spine, the convention is inverted. Displacement is described as the proximal segment relative to the distal segment. A classic example is anterolisthesis of L4 on L5, where the L4 vertebral body (proximal) translates anteriorly over L5 (distal).
This reversed convention is also applied to the proximal articular segments of the appendicular skeleton, namely the femoral and humeral heads. A classic clinical manifestation of this exception is observed in slipped capital femoral epiphysis. In this pediatric hip pathology, the deformity is described by the displacement of the proximal epiphysis relative to the distal metaphysis, rather than vice versa. Understanding these nuanced conventions is paramount for accurate clinical communication, precise preoperative templating, and the flawless execution of complex reconstructive procedures.
Pathophysiology and Soft Tissue Envelope Dynamics
The pathophysiology of translation deformity is distinct from that of pure angular deformity, particularly regarding its profound impact on the surrounding soft tissue envelope and the bone healing cascade. In the context of distraction osteogenesis and deformity correction, the biological environment is just as critical as the mechanical construct.
Osseous Apposition and Nonunion Risk
Translation of bone ends inherently leads to a volumetric loss of cortical and cancellous bone contact. When the magnitude of the translation deformity exceeds the diaphyseal or metaphyseal diameter of the bone at that specific anatomical level, there is a complete loss of osseous apposition.
This catastrophic loss of contact disrupts the medullary canal, devascularizes the immediate fracture or osteotomy site, and severely compromises the intrinsic stability of the segment. The endosteal blood supply is entirely severed, forcing the bone to rely solely on the periosteal blood supply, which is often simultaneously compromised by the initial trauma or surgical approach. Consequently, translation deformities are highly associated with the development of atrophic or oligotrophic nonunions. The lack of mechanical continuity prevents the normal transmission of compressive forces necessary for secondary bone healing via endochondral ossification.
Shear Stress and Axial Shortening
In stark contrast to pure angulation, which leads to the asymmetric stretching of the soft tissue envelope on the convex side and relaxation on the concave side, pure translation disrupts bone contact entirely. The soft tissues, including the periosteum, muscle fascia, and critical neurovascular bundles, undergo severe shear stress rather than simple longitudinal tension.
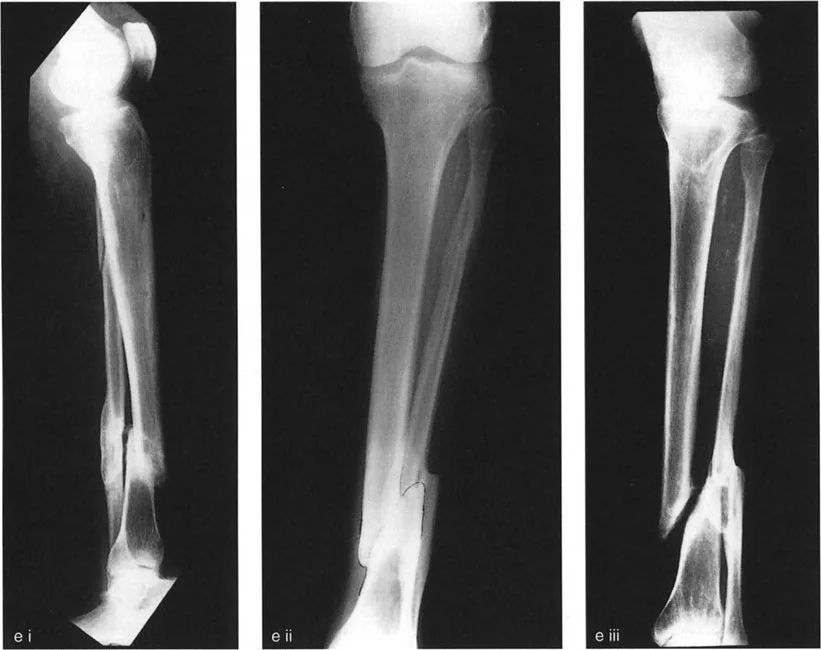
When complete loss of bone contact occurs, secondary deforming forces inevitably lead to axial shortening. These forces include gravity, weight-bearing loads, and relentless muscle spasm. Shortening is defined as displacement in the axial direction, whereas translation is displacement perpendicular to the long axis of the bone. In clinical reality, shortening and translation are inextricably linked. The region of bone overlap observed on orthogonal radiographs represents the exact level and magnitude of the translation deformity.
- Surgical Pearl Severe shear stress on neurovascular structures makes acute correction of long-standing translation deformities highly dangerous. Gradual correction using circular external fixation is often mandated to prevent neurapraxia or vascular tethering.
Geometric Parameters of Translation Deformity
To effectively analyze and correct translation deformities, the orthopedic surgeon must meticulously define the deformity using four critical parameters. These parameters mirror those used for angular deformities but require a different geometric approach based on Paley principles.
Defining Plane Direction Magnitude and Level
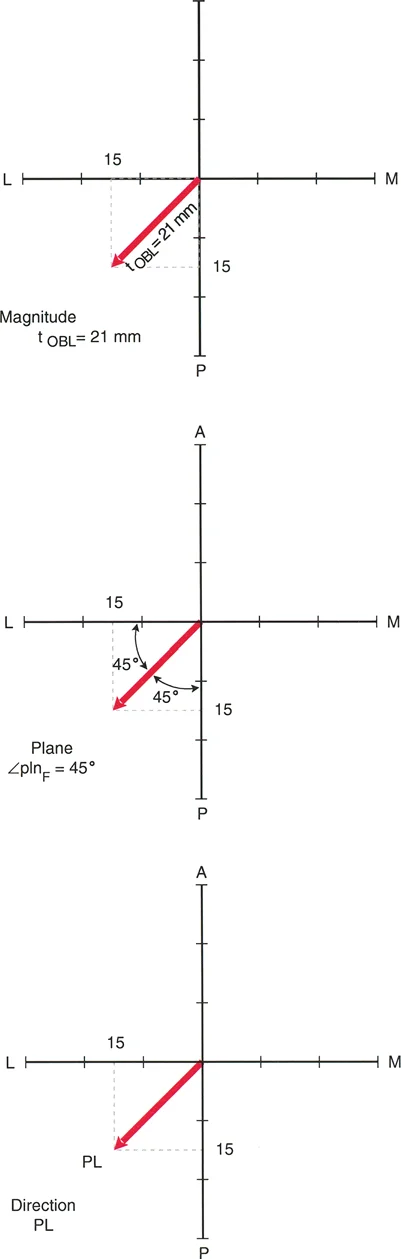
The four pillars of defining a translation deformity are plane, direction, magnitude, and level.
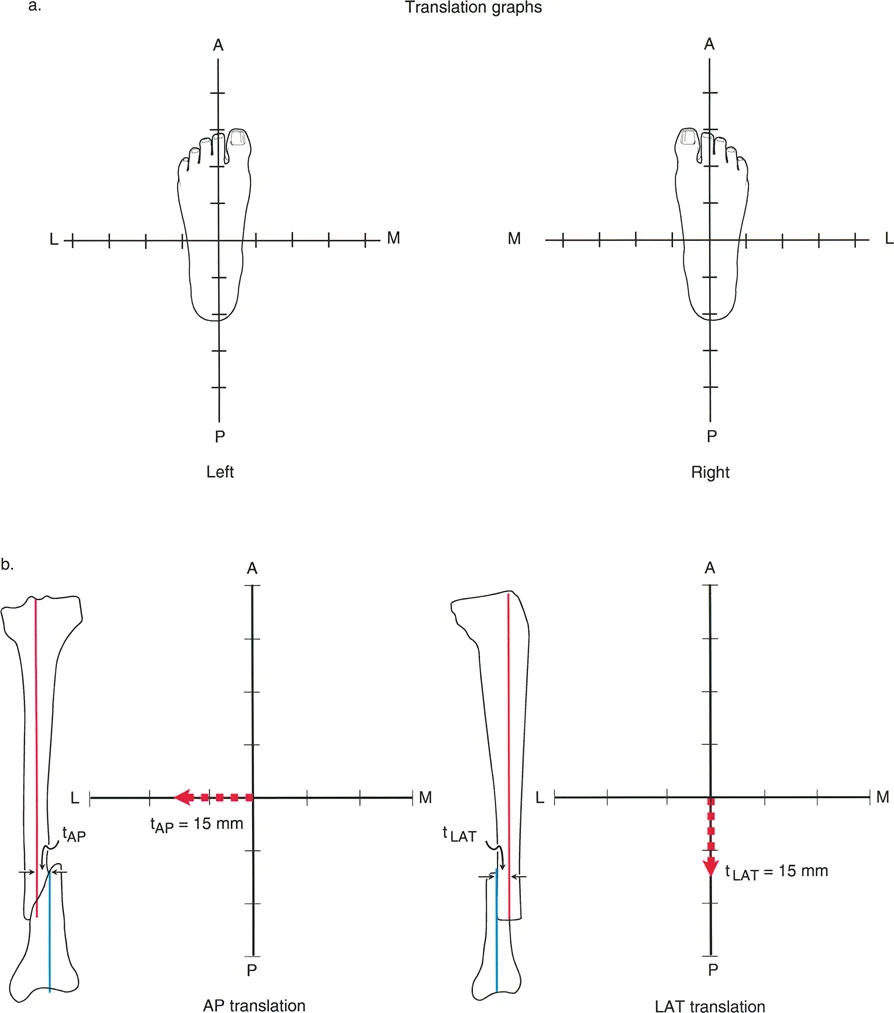
- Plane The plane of translation is categorized into anatomic planes (coronal/frontal or sagittal) and oblique planes. Anatomic plane translation deformities are visible purely on either the anteroposterior or lateral orthogonal radiographs. Oblique plane translation deformities, which represent the vast majority of clinical cases, exhibit translation on both projections.
- Direction This describes the vector of the distal segment's displacement. Vectors can be anterior, posterior, medial, lateral, or a combined oblique vector such as anterolateral.
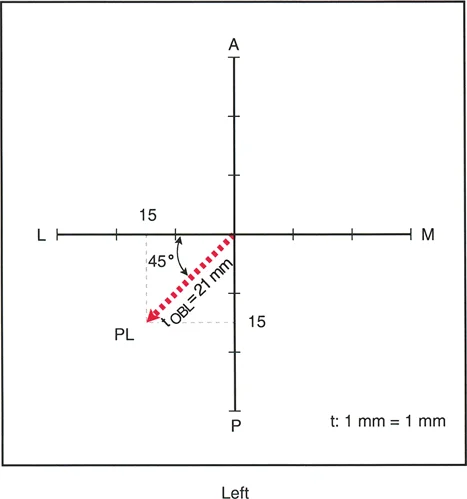
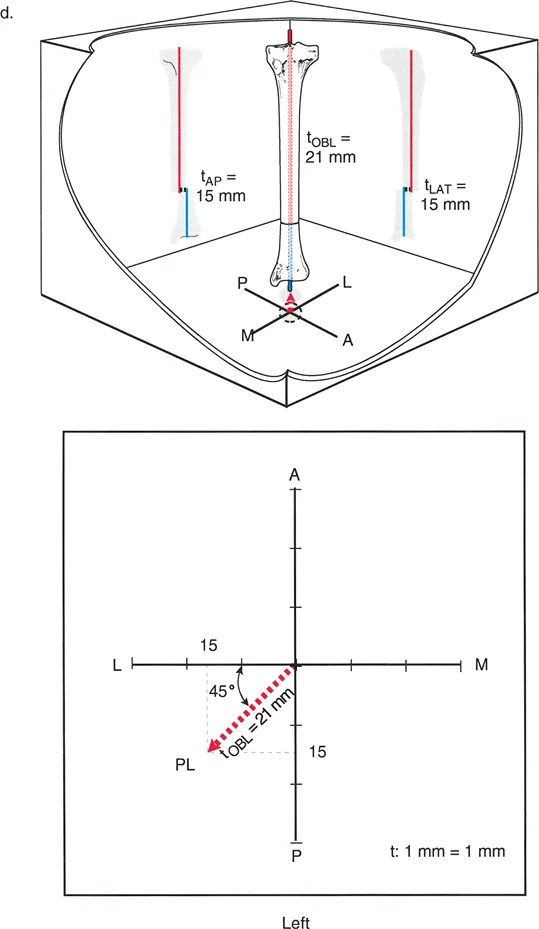
- Magnitude This is the absolute distance of displacement, measured in millimeters, in the true plane of the deformity. For oblique deformities, the true magnitude must be calculated using the Pythagorean theorem based on the AP and lateral translation values.
- Level The level of the deformity is defined as the specific cross-sectional zone where the bone ends are translated relative to each other. In the presence of concurrent shortening, this corresponds directly to the zone of cortical overlap.
Mastery of these four parameters forms the absolute foundation for all subsequent preoperative planning and surgical execution. Without defining the true oblique plane of a translation deformity, any attempt at correction will inadvertently induce a secondary iatrogenic deformity in the orthogonal plane.
Biomechanics and the Mechanical Axis Deviation Paradox
The biomechanical consequences of translation deformities are profound, primarily due to their direct effect on the mechanical axis of the lower extremity. While angular deformities are widely recognized as the primary drivers of Mechanical Axis Deviation and subsequent early-onset osteoarthritis, the deleterious effects of pure translation are frequently underestimated in clinical practice.
Impact on Lower Extremity Alignment
Translation deformity of the femur or tibia in the coronal plane produces significant Mechanical Axis Deviation. This shift alters the weight-bearing load across the knee and ankle joints, precipitating asymmetric cartilage wear, meniscal pathology, and subchondral sclerosis. The mechanical axis of the lower extremity is defined by a line drawn from the center of the femoral head to the center of the ankle joint. In a normally aligned limb, this line passes just medial to the center of the knee joint.
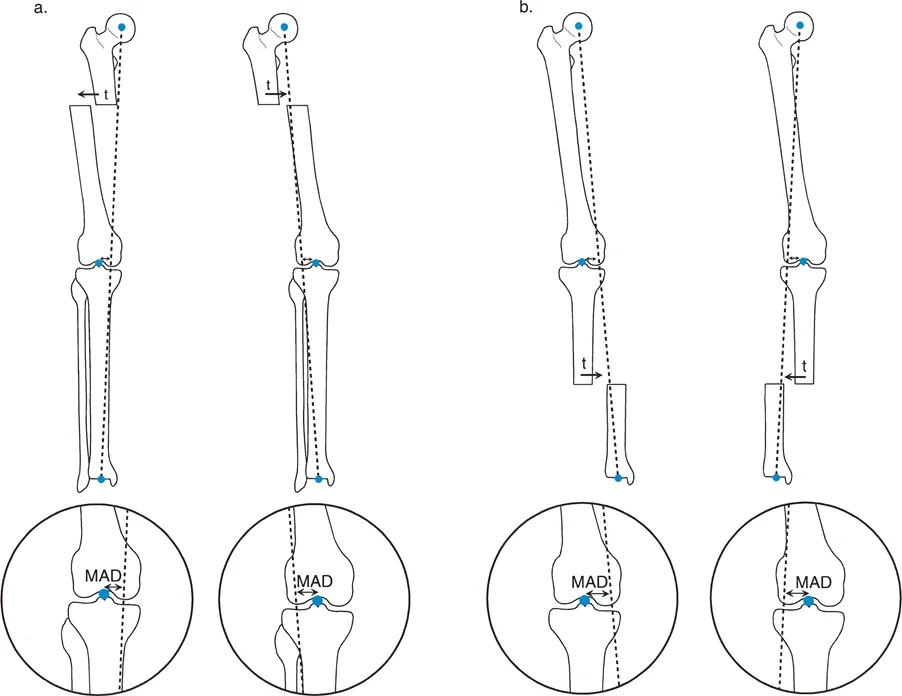
When translation occurs in the diaphysis or metaphysis, it physically moves the distal joint center relative to the proximal joint center. Even if the joint orientation angles remain perfectly normal, the shift in the joint center's location pulls the mechanical axis line away from the center of the knee.
Understanding the Translation Paradox
A critical biomechanical paradox exists regarding the direction of translation and its corresponding effect on the mechanical axis. This is known as the Translation Paradox, a high-yield concept for reconstructive surgeons.
- Femoral Translation Paradox Medial translation of the distal femoral segment physically moves the knee joint center medially. However, when the mechanical axis line is drawn from the femoral head to the ankle, this medial shift of the knee causes the mechanical axis line to fall lateral to the center of the knee. Therefore, medial translation of the femur creates a lateral Mechanical Axis Deviation, effectively inducing a valgus mechanical load. Conversely, lateral translation of the distal femur creates a medial Mechanical Axis Deviation, inducing a varus mechanical load.
- Tibial Translation Paradox Lateral translation of the distal tibial segment moves the ankle joint center laterally. This shifts the mechanical axis line medially relative to the knee joint, creating a medial Mechanical Axis Deviation and a varus mechanical load. Medial translation of the distal tibia shifts the mechanical axis laterally, creating a valgus mechanical load.
Understanding this paradox is essential. A surgeon might intuitively think that medial translation causes a medial mechanical shift, but the geometric reality is the exact opposite.
Applying Paley Principles to Translation Deformities
Dr. Dror Paley's principles of deformity correction provide a universal geometric language for understanding and correcting complex limb deformities. Applying these principles to pure translation requires a deep understanding of the Center of Rotation of Angulation and Joint Orientation Angles.
Center of Rotation of Angulation CORA in Translation
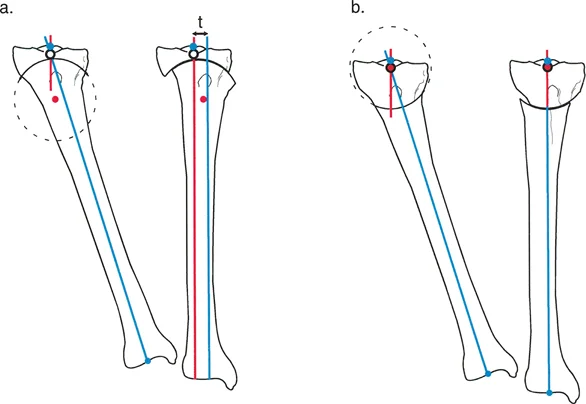
The Center of Rotation of Angulation is typically defined as the intersection point of the proximal and distal mechanical or anatomic axis lines. However, in a pure translation deformity, the proximal and distal axis lines are perfectly parallel. Because parallel lines never intersect, the CORA for a pure translation deformity is mathematically located at infinity.
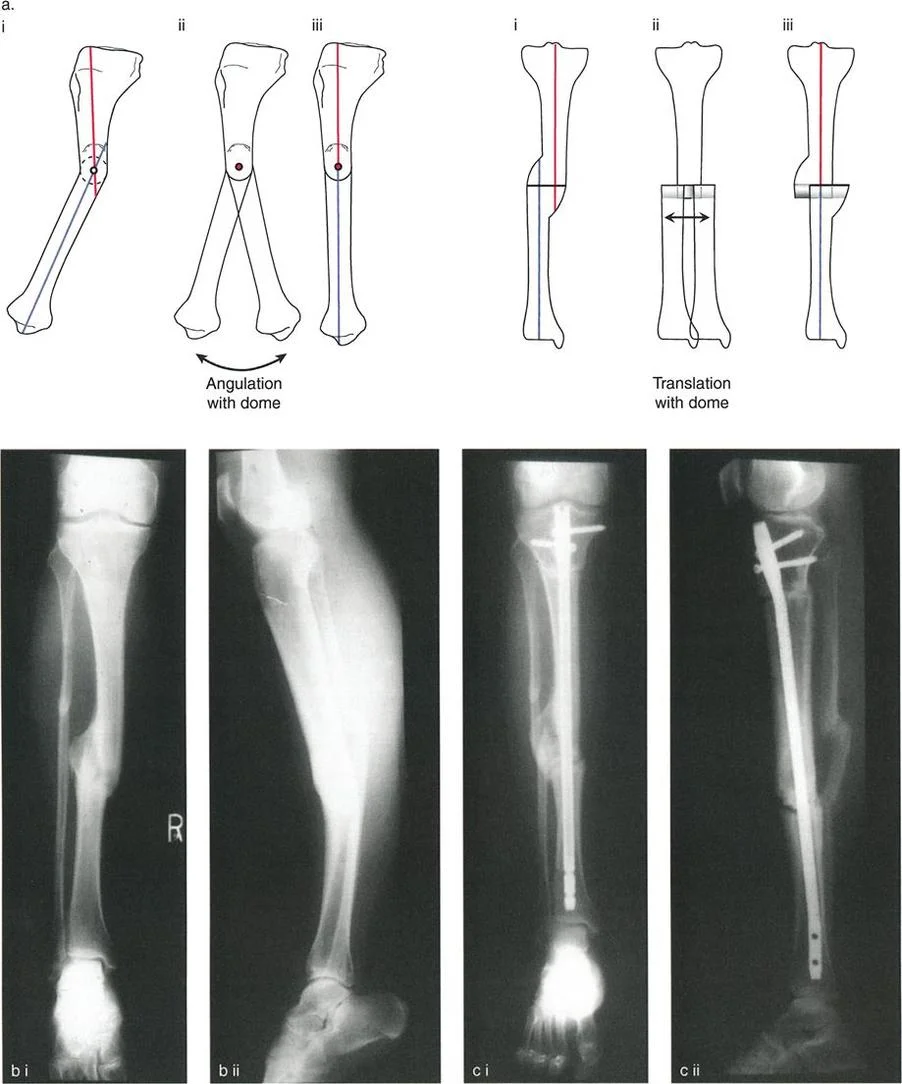
Since the surgeon cannot place a hinge at infinity to correct the deformity, pure translation must be corrected via a transverse sliding osteotomy, or by converting the translation into an angular deformity using a double-level osteotomy. If a single-level osteotomy is performed and angulated to correct the mechanical axis, it will inevitably create a secondary, compensatory angular deformity, violating Paley's rules.
Joint Orientation Angles mLDFA MPTA and JLCA
To confirm that a deformity is pure translation and does not possess a hidden angular component, the surgeon must measure the joint orientation angles. These angles define the relationship between the mechanical axis of a bone segment and its respective joint line.
| Joint Orientation Angle | Acronym | Normal Value Range | Clinical Significance |
|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85 to 90 degrees | Assesses coronal plane alignment of the distal femur. |
| Medial Proximal Tibial Angle | MPTA | 85 to 90 degrees | Assesses coronal plane alignment of the proximal tibia. |
| Joint Line Convergence Angle | JLCA | 0 to 2 degrees | Assesses intra-articular deformity or ligamentous laxity at the knee. |
| Mechanical Lateral Proximal Femoral Angle | mLPFA | 85 to 90 degrees | Assesses coronal plane alignment of the proximal femur. |
In a pure translation deformity, the mLDFA and MPTA will remain within normal limits, while the Mechanical Axis Deviation will be abnormal. If the joint orientation angles are abnormal, the surgeon is dealing with a combined angulation-translation deformity, which requires a more complex mathematical approach to locate the true CORA.
Paley Osteotomy Rules for Translation Correction
Dr. Paley established three fundamental osteotomy rules for deformity correction. While primarily designed for angular deformities, understanding how they interact with translation is crucial.
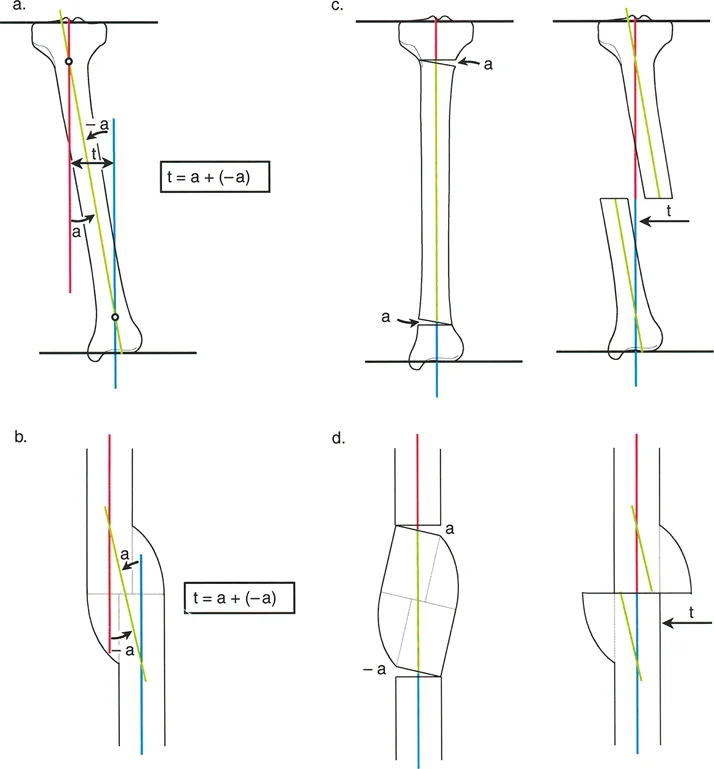
- Osteotomy Rule 1 When the osteotomy and the mechanical hinge are placed precisely at the CORA, pure angular correction occurs without inducing translation.
- Osteotomy Rule 2 When the mechanical hinge is placed at the CORA, but the osteotomy is performed at a different level, angular correction occurs simultaneously with translation at the osteotomy site.
- Osteotomy Rule 3 When the osteotomy and the mechanical hinge are placed at a level separate from the CORA, a secondary translation deformity is iatrogenically induced.
For a pre-existing pure translation deformity, the surgeon must perform a translation-only correction at the exact level of the deformity. If the translation is corrected at a level proximal or distal to the actual deformity, an iatrogenic step-off will be created, altering the anatomic axis and potentially compromising the medullary canal for future intramedullary nailing.
Preoperative Planning and Radiographic Templating
Meticulous preoperative planning is the hallmark of a successful deformity correction surgeon. The Malalignment Test and subsequent templating must be performed on weight-bearing, full-length orthogonal radiographs of the affected extremity.
Step by Step Guide to Deformity Analysis
The following standardized approach ensures that no geometric parameter is overlooked during the evaluation of a translation deformity.
- Obtain Proper Imaging Ensure full-length, weight-bearing AP and lateral radiographs are available, with the patella facing strictly forward to control for rotational variations.
- Perform the Malalignment Test Draw the mechanical axis of the entire lower extremity from the center of the femoral head to the center of the ankle plafond. Measure the Mechanical Axis Deviation in millimeters from the center of the knee joint.
- Analyze Joint Orientation Angles Measure the mLDFA and MPTA. If these are normal, but the MAD is abnormal, suspect a pure translation deformity.
- Draw Segmental Axes Draw the mechanical axis lines for the proximal and distal segments of the deformed bone. In pure translation, these lines will be parallel.
- Determine the Magnitude Measure the perpendicular distance between the parallel proximal and distal axis lines. This represents the magnitude of the translation deformity in that specific radiographic plane.
- Calculate Oblique Plane Parameters If translation is present on both AP and lateral views, use trigonometric principles to calculate the true oblique plane magnitude and direction.
- Identify the Level Locate the exact level of cortical overlap or step-off. This dictates the optimal level for the corrective osteotomy.
- Surgical Pearl Always evaluate for limb length discrepancy during the planning phase. Because translation deformities frequently result in axial shortening, a lengthening procedure is often required concomitantly with the translation correction.
Surgical Execution and Correction Strategies
Once the deformity has been perfectly quantified, the surgeon must choose the appropriate fixation strategy and dictate the pace of the correction. The biological health of the soft tissue envelope and the magnitude of the deformity are the primary drivers of this decision.
Acute versus Gradual Correction Techniques
The decision between acute and gradual correction is one of the most critical junctures in deformity surgery.
Acute Correction is generally reserved for translation deformities of small magnitude (typically less than 1 to 1.5 centimeters) where the soft tissue envelope is compliant. Acute correction requires extensive soft tissue stripping to mobilize the bone ends, which can further devascularize an already compromised nonunion site. Following acute translation, the bone can be stabilized using internal fixation, such as intramedullary nails or rigid locking plates.
Gradual Correction is mandated for large magnitude translation deformities, cases with severe soft tissue contractures, or when concurrent limb lengthening is required. Gradual correction utilizes the biological principle of distraction histogenesis, specifically the tension-stress effect described by Ilizarov. By moving the bone ends slowly (typically 1 millimeter per day), the periosteum, muscles, nerves, and blood vessels safely regenerate and accommodate the new anatomical position.
External Fixation and Spatial Frame Applications
Circular external fixation remains the gold standard for the gradual correction of complex translation deformities. Traditional Ilizarov frames rely on complex hinge and translation assemblies to achieve correction. The surgeon must build a mechanical construct that perfectly mirrors the geometric parameters of the deformity. For pure translation, this requires the use of translation mechanisms (such as threaded rods and nuts) mounted orthogonally to the bone axis.
Modern reconstructive surgery heavily utilizes hexapod circular fixators, such as the Taylor Spatial Frame. These devices utilize a virtual hinge and sophisticated software algorithms. The surgeon inputs the exact parameters of the deformity (plane, direction, magnitude, and level) along with the mounting parameters of the frame. The software then generates a daily prescription for the patient to turn the six struts.
The paramount advantage of the hexapod system in translation deformities is its ability to correct translation, angulation, rotation, and length simultaneously through a single osteotomy site. Because the software calculates the 3D movement of the bone segments, it prevents the severe shear stresses that manual translation might otherwise place on the neurovascular bundles, ensuring a safe, precise, and biologically sound restoration of the mechanical axis.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like