Masterclass in Open Fractures: Surgical Management & Limb Salvage
Key Takeaway
Open fractures represent critical surgical emergencies requiring immediate, aggressive intervention. Successful management hinges on a multidisciplinary approach, prioritizing life preservation before limb salvage. This comprehensive guide details the evolution of open fracture care, from meticulous surgical debridement and targeted antibiotic prophylaxis to advanced stabilization techniques like intramedullary nailing. By understanding biofilm microbiology and utilizing validated severity scores, orthopedic surgeons can optimize functional outcomes and mitigate severe complications such as chronic osteomyelitis and amputation.
Introduction and Epidemiology
An open fracture refers to an osseous disruption in which a break in the skin and underlying soft tissue communicates directly with the fracture and its surrounding hematoma. While the term compound fracture historically referred to this same injury pattern, it is now considered archaic and should be abandoned in modern orthopedic nomenclature. The management of open fractures represents one of the most critical and time-sensitive challenges in orthopedic trauma, requiring a comprehensive understanding of both osseous stability and soft tissue viability.
Epidemiological data demonstrates that open fractures are predominantly the result of high-energy trauma. Consequently, approximately one-third of patients presenting with open fractures are multiply injured, necessitating a multidisciplinary approach to initial resuscitation and management. A fundamental clinical axiom dictates that any wound occurring on the same limb segment as a fracture must be suspected to be a consequence of an open fracture until proven otherwise.
Soft tissue injuries in the context of an open fracture have three primary and severe consequences that dictate the clinical course. First, there is immediate contamination of the wound and the fracture site due to exposure to the external environment, establishing a nidus for potential infection. Second, the mechanism of injury typically involves significant crushing, stripping, and devascularization. This results in severe soft tissue compromise, local hypoxia, and a dramatically increased susceptibility to deep infection. Third, the destruction or loss of the soft tissue envelope directly affects the method of fracture immobilization. The loss of periosteal and muscular coverage compromises the contribution of overlying soft tissues to fracture healing, specifically the critical supply of osteoprogenitor cells and regional blood flow. Furthermore, this structural damage frequently results in long-term functional deficits secondary to muscle, tendon, nerve, vascular, ligament, or extensive skin loss.
Surgical Anatomy and Biomechanics
Kinetic Energy and Injury Mechanics
Open fractures result primarily from the application of violent external forces. The severity of the injury is directly proportional to the amount of kinetic energy transferred to the limb. The applied kinetic energy is dissipated by both the soft tissue envelope and the underlying osseous structures.

According to the principles of physics, kinetic energy is calculated as one-half the mass times the velocity squared. Therefore, high-velocity injuries, such as motorcycle collisions or high-caliber ballistic trauma, impart exponentially greater energy to the limb compared to low-velocity crush injuries or ground-level falls. The amount of bony displacement and comminution observed on initial radiographs is highly suggestive of the degree of surrounding soft tissue injury and is directly proportional to the applied force. Severe comminution indicates a massive energy transfer that has invariably caused extensive, often occult, damage to the surrounding musculature and microvasculature.

Soft Tissue Envelope Dynamics
The soft tissue envelope of the extremities acts as a critical biological barrier and a vascular reservoir. In the lower extremity, particularly the anteromedial tibia, the soft tissue envelope is notoriously thin, making it highly susceptible to open fractures and subsequent healing complications. The periosteal blood supply, which provides the majority of the blood flow to the outer third of the diaphyseal cortex, is frequently stripped during the initial displacement of the fracture fragments.

When the medullary blood supply is simultaneously disrupted by the fracture, the cortical bone becomes completely avascular. The survival of this bone relies entirely on the rapid revascularization from the surrounding muscle beds. If the surrounding muscle is crushed or devitalized, the bone remains ischemic, leading to a high risk of osteomyelitis, nonunion, and structural failure.
Vascular and Neurological Considerations
The proximity of major neurovascular bundles to the skeletal structures places them at high risk during the initial traumatic displacement. For example, fractures of the distal femur or proximal tibia frequently compromise the popliteal artery due to its tethering at the adductor hiatus and the soleal arch. Similarly, the radial nerve is highly susceptible to traction or transection in open fractures of the humeral shaft. Understanding the anatomical zones of injury is paramount; the true zone of injury extends far beyond the visible skin laceration, encompassing a wide area of microvascular thrombosis and cellular stunning that will declare itself in the days following the initial trauma.
Indications and Contraindications
Operative Management Criteria
The presence of an open fracture is an absolute indication for urgent operative intervention. The primary goals of surgery are the prevention of infection, stabilization of the fracture, and the restoration of soft tissue coverage. Operative management includes formal surgical debridement, copious irrigation, and skeletal stabilization.

Non Operative Considerations
True contraindications to the operative management of an open fracture are exceedingly rare and are generally limited to patients who are medically unstable and cannot tolerate anesthesia, or those in extremis where life-saving resuscitative measures take absolute precedence over limb salvage. In highly selected, isolated, low-energy open fractures (e.g., inside-out puncture wounds from low-energy torsional tibial fractures), some literature supports meticulous emergency department management followed by close clinical observation, though this remains controversial and is generally discouraged in academic trauma centers.
| Clinical Scenario | Operative Indication | Non Operative Indication | Rationale and Management Strategy |
|---|---|---|---|
| High Energy Open Fracture | Absolute | None | Requires urgent OR debridement, irrigation, and stabilization to prevent sepsis and osteomyelitis. |
| Hemodynamically Unstable Polytrauma | Damage Control Orthopedics | Definitive Fixation Contraindicated | Rapid external fixation and hemostasis; delay definitive intramedullary or plate fixation until physiologically optimized. |
| Mangled Extremity with Ischemia | Immediate Revascularization or Amputation | None | Prolonged warm ischemia time dictates immediate shunting or primary amputation based on MESS or clinical judgment. |
| Patient in Extremis | None | Absolute | Life over limb; supportive care and bedside provisional splinting until the patient can survive transport to the OR. |
Pre Operative Planning and Patient Positioning
Initial Trauma Evaluation and Resuscitation
Patient assessment must strictly adhere to Advanced Trauma Life Support protocols, prioritizing the ABCDEs: airway, breathing, circulation, disability, and exposure. The orthopedic surgeon must initiate resuscitation and address life-threatening injuries in concert with the general trauma surgery team. A thorough evaluation of injuries to the head, chest, abdomen, pelvis, and spine is mandatory before focusing on the extremities.
Once life-threatening conditions are stabilized, identify all injuries to the extremities. Assess and meticulously document the neurovascular status of the injured limbs prior to any manipulation or splinting.
Wound Assessment and Antimicrobial Prophylaxis
Assess the skin and soft tissue damage carefully. A critical principle in the emergency management of open fractures is that formal exploration of the wound in the emergency setting is strictly contraindicated if operative intervention is planned. Emergency room exploration risks driving superficial contaminants deeper into the wound bed, provides limited useful information due to inadequate lighting and anesthesia, and may precipitate severe, uncontrollable hemorrhage by dislodging provisional clots.
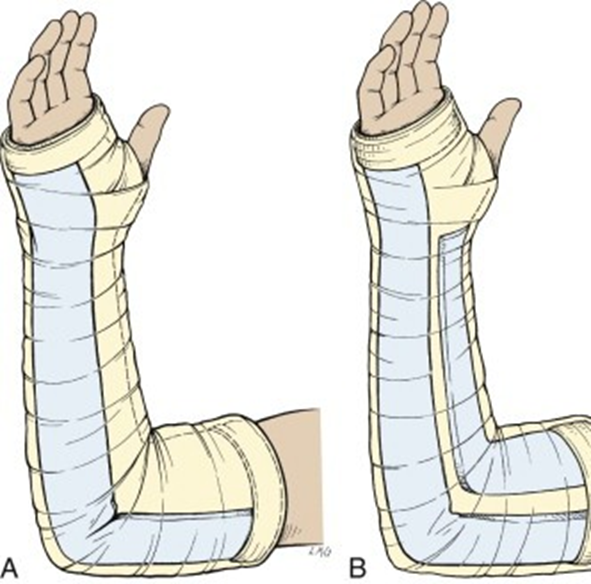
Obvious foreign bodies that are easily accessible at the surface may be removed in the emergency room under sterile conditions. If a significant surgical delay is expected, superficial irrigation of the wounds with sterile normal saline may be performed, followed by the application of a sterile, saline-soaked dressing and a well-padded splint.
Intravenous antibiotics must be administered as soon as possible, ideally within one hour of injury. The choice of antibiotics is dictated by the Gustilo-Anderson classification. Type I and II fractures typically require first-generation cephalosporins (e.g., Cefazolin) to cover Gram-positive organisms. Type III fractures require the addition of Gram-negative coverage, typically an aminoglycoside (e.g., Gentamicin) or a third-generation cephalosporin (e.g., Ceftriaxone). If gross contamination with soil or organic matter is present, high-dose Penicillin should be added to cover anaerobic organisms, specifically Clostridium species, to prevent gas gangrene. Tetanus prophylaxis must be updated based on the patient's immunization history.
Imaging and Vascular Assessment
Identify the skeletal injury and obtain necessary orthogonal radiographs of the affected limb, including the joints above and below the fracture.

Computed tomography has been shown to be a highly effective method to assess for traumatic arthrotomy in periarticular open fractures. The presence of intra-articular air on a CT scan in the presence of an open periarticular wound is diagnostic for a traumatic arthrotomy and necessitates formal joint exploration and washout.
Vascular injuries must be ruled out. Ankle brachial indices must be obtained if any signs of vascular compromise exist. This is obtained by measuring the systolic pressure at the ankle and dividing it by the systolic pressure at the arm. A normal ratio is greater than 0.9. An ABI less than 0.9, or asymmetric pulses, mandates further investigation.

A formal vascular surgery consultation and a CT angiogram should be obtained immediately if a vascular injury is suspected. Hard signs of vascular injury (pulsatile bleeding, expanding hematoma, absent distal pulses, palpable thrill) dictate immediate operative exploration, often preceding or concurrent with orthopedic stabilization. Specific indications for an angiogram include high-risk injury patterns such as a knee dislocation with an asymmetric pulse examination.
Operating Room Setup
Proper patient positioning is dictated by the location of the fracture and the planned surgical approach. A radiolucent table is generally required to facilitate unrestricted fluoroscopic imaging. The entire limb must be prepped and draped freely to allow for dynamic manipulation, assessment of mechanical alignment, and potential extension of incisions. A sterile tourniquet should be applied proximal to the injury zone; however, it should remain uninflated during the initial debridement to allow the surgeon to accurately assess tissue perfusion and muscular contractility.
Detailed Surgical Approach and Technique
Wound Debridement Principles
The cornerstone of open fracture management is radical and meticulous surgical debridement. The objective is to convert a contaminated, necrotic wound into a clean, viable surgical bed.

The traumatic wound should be extended proximally and distally along standard, extensile internervous planes to fully expose the zone of injury. Skin margins should be sharply excised until healthy, bleeding dermal edges are encountered.
Muscle viability is assessed using the classic four Cs: color, consistency, contractility, and capacity to bleed. Muscle that is dark, friable, non-contractile to electrocautery stimulation, and does not bleed must be aggressively excised. Retained necrotic muscle is the primary substrate for deep infection. Bone fragments that are completely devoid of soft tissue attachments and lack cortical bleeding should generally be removed, particularly if they are small and non-articular. However, large articular fragments or critical diaphyseal segments necessary for length and stability may be retained after thorough mechanical cleaning, provided the surrounding soft tissue envelope is robust enough to eventually support revascularization.
Following debridement, the wound is subjected to copious irrigation. Current evidence, notably the FLOW trial, suggests that irrigation with normal saline delivered via low-pressure gravity flow is as effective as, and potentially less damaging to host tissues than, high-pressure pulsatile lavage or the use of castile soap.
Fracture Stabilization Strategies
Once the wound is adequately debrided, the fracture must be stabilized. Stabilization reduces dead space, prevents further soft tissue trauma from mobile bone fragments, restores length and alignment, and creates a mechanical environment conducive to soft tissue healing and immune function.

The choice of fixation depends on the patient's physiologic status, the location of the fracture, and the severity of the soft tissue injury.
1. External Fixation: Frequently utilized as a damage control measure in polytraumatized patients or in cases of severe soft tissue compromise (Gustilo-Anderson Type IIIB or IIIC) where internal implants would be exposed or at unacceptably high risk of infection. Spanning external fixators provide rapid stability and allow unrestricted access for subsequent wound care and soft tissue coverage.
2. Intramedullary Nailing: The gold standard for diaphyseal fractures of the femur and tibia. Reamed intramedullary nailing can be safely performed in most low-grade open fractures and selected high-grade open fractures after adequate debridement. It provides load-sharing stability and preserves the periosteal blood supply.
3. Plate Osteosynthesis: Typically reserved for periarticular open fractures or upper extremity diaphyseal fractures. Meticulous soft tissue handling is required to avoid further devascularization of the fracture fragments.
Soft Tissue Coverage and Management
The timing and method of soft tissue coverage are critical determinants of limb salvage. The "fix and flap" philosophy advocates for early definitive skeletal stabilization and simultaneous soft tissue coverage, ideally within 72 hours of injury. If the wound cannot be closed primarily without tension, negative pressure wound therapy is frequently employed as a temporary dressing. NPWT reduces tissue edema, promotes granulation tissue formation, and manages wound exudate while awaiting definitive coverage.
For Gustilo-Anderson Type IIIB fractures, local rotational flaps (e.g., gastrocnemius flap for the proximal third of the tibia, soleus flap for the middle third) or free tissue transfer (e.g., anterolateral thigh flap, latissimus dorsi flap for the distal third of the tibia) are required to provide robust, vascularized coverage over exposed bone and hardware.
Management of Traumatic Arthrotomy
If a traumatic arthrotomy is confirmed, the joint must be formally explored, debrided, and irrigated. Intra-articular foreign bodies and loose chondral fragments must be removed. The joint capsule should be closed primarily if possible, or managed with a temporary seal (e.g., antibiotic bead pouch) if staged management is planned.
Complications and Management
Compartment Syndrome
An open fracture does not preclude the development of acute compartment syndrome. This is a critical and frequently misunderstood concept. The fascial defect created by an open fracture is rarely sufficient to decompress the entire fascial compartment, particularly with severe blunt trauma, high-energy crush injuries, or prolonged ischemia-reperfusion scenarios.
Severe pain out of proportion to the injury, decreased sensation in the distribution of nerves traversing the compartment, excruciating pain to passive stretch of the fingers or toes, and a palpably tense extremity are all classic clinical clues to the diagnosis. However, in polytraumatized, intubated, or unconscious patients, clinical examination is unreliable. A strong clinical suspicion in the appropriate clinical setting warrants immediate monitoring of compartment pressures.
Compartment pressures greater than 30 mm Hg raise significant concern. More accurately, a differential pressure (delta P) calculated as the diastolic blood pressure minus the intracompartmental pressure of less than 30 mm Hg is highly indicative of compartment syndrome. If these criteria are met, immediate, four-compartment fasciotomies (in the lower leg) or appropriate regional fasciotomies must be performed without delay. It is vital to remember that distal pulses may remain present and palpable long after muscle and nerve ischemia have occurred and irreversible damage has been sustained.
Infection and Osteomyelitis
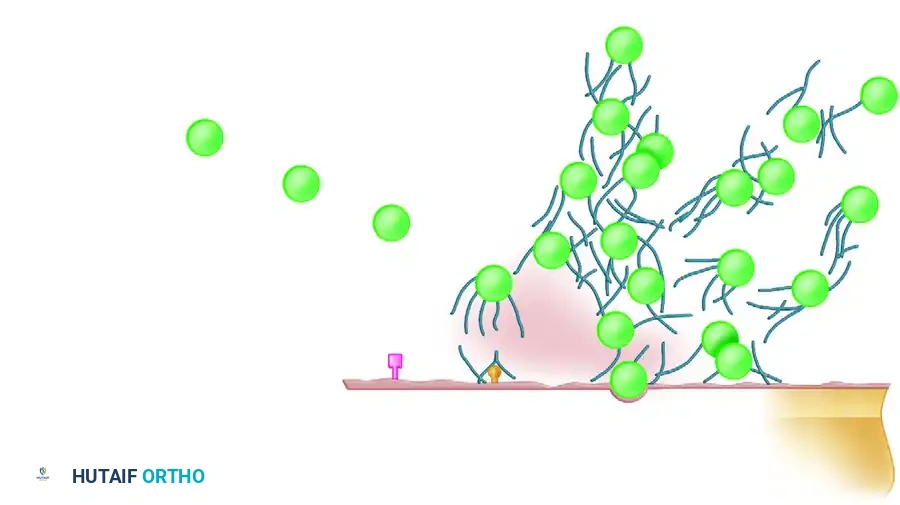
Deep infection remains the most devastating complication of open fractures. The presence of necrotic tissue, avascular bone, and orthopedic hardware creates an ideal environment for bacterial colonization and biofilm formation.

Management of post-traumatic osteomyelitis requires a multidisciplinary approach involving radical surgical debridement of all infected and non-viable bone, removal of colonized hardware, and targeted, prolonged systemic antibiotic therapy directed by deep tissue cultures. Dead space management frequently involves the use of local antibiotic delivery systems, such as polymethylmethacrylate cement spacers loaded with heat-stable antibiotics (e.g., Tobramycin, Vancomycin).
Nonunion and Amputation
The combination of severe osseous disruption, periosteal stripping, and soft tissue compromise frequently leads to delayed union or nonunion. Management may require revision fixation, autologous bone grafting (e.g., iliac crest bone graft), or the utilization of the Masquelet induced-membrane technique for critical-sized bone defects.
In cases of unsalvageable severe soft tissue destruction, irreversible ischemic injury, or overwhelming sepsis, amputation may be the only viable option to preserve the patient's life.

| Complication | Incidence Rate | Pathophysiology | Salvage and Management Strategy |
|---|---|---|---|
| Deep Infection / Osteomyelitis | 5-30% (Increases with Gustilo Grade) | Bacterial contamination, devascularized bone, biofilm formation on hardware. | Radical serial debridement, hardware removal if unstable, antibiotic cement spacers, culture-directed IV antibiotics. |
| Acute Compartment Syndrome | 2-9% (Highest in tibial shaft fractures) | Increased intracompartmental pressure exceeding capillary perfusion pressure despite open fascial defect. | Emergent multi-compartment fasciotomies. Delayed primary closure or split-thickness skin grafting once swelling subsides. |
| Aseptic Nonunion | 10-25% | Biological failure due to periosteal stripping, lack of soft tissue coverage, or mechanical instability. | Revision osteosynthesis to optimize stability, autologous bone grafting, or bone transport via Ilizarov methods. |
| Amputation | Variable (Dependent on vascular injury) | Irreversible ischemia, overwhelming local sepsis, or massive crush injury precluding functional salvage. | Level chosen based on tissue viability and prosthetic fitting. Early psychological support and rehabilitation. |
Post Operative Rehabilitation Protocols
Early Mobilization Strategies
The rehabilitation of a patient with an open fracture must be highly individualized, balancing the need for early mobilization to prevent systemic complications with the mechanical limitations of the fracture fixation and the fragility of the soft tissue reconstruction. Early mobilization is paramount to prevent deep vein thrombosis, pulmonary embolism, atelectasis, and generalized deconditioning.
Range of motion exercises for adjacent, uninjured joints should commence immediately post-operatively. For periarticular fractures, early passive and active-assisted range of motion of the affected joint is initiated as soon as the surgical wound and soft tissue coverage are deemed stable by the operating surgeon, often utilizing continuous passive motion machines to prevent intra-articular adhesions and arthrofibrosis.
Weight Bearing Progression
Weight-bearing status is strictly dictated by the biomechanical stability of the osteosynthesis construct and the biological progression of fracture healing.
* Intramedullary Nailing: For diaphyseal fractures treated with statically locked intramedullary nails, early weight-bearing as tolerated is frequently permitted and biomechanically encouraged, as the load-sharing nature of the device promotes secondary bone healing via callus formation.
* Plate Osteosynthesis: Fractures managed with load-bearing constructs, such as bridging plates for comminuted metaphyseal fractures, typically require a period of protected, non-weight-bearing or touch-down weight-bearing until radiographic evidence of bridging callus is observed (typically 6 to 12 weeks).
* External Fixation: Patients managed in spanning external fixators are generally restricted to non-weight-bearing status on the affected extremity.
Rigorous deep vein thrombosis prophylaxis, utilizing low molecular weight heparin or direct oral anticoagulants, is mandatory until the patient is fully mobilized, barring any specific medical contraindications.
Summary of Key Literature and Guidelines
Foundational Studies
The management of open fractures is heavily guided by several foundational studies and classification systems. The Gustilo-Anderson classification, originally published in 1976 and modified in 1984, remains the universal standard for categorizing open fractures based on wound size, degree of soft tissue injury, and contamination. This classification directly dictates antibiotic protocols and predicts the risk of infection and amputation.
The Lower Extremity Assessment Project was a landmark multicenter prospective study that evaluated the outcomes of severe lower extremity trauma. A critical finding of the LEAP study was that there is no significant difference in long-term functional outcomes between patients who undergo early amputation and those who undergo complex limb salvage procedures. This data is vital when counseling patients with severely mangled extremities, emphasizing that limb salvage does not necessarily equate to functional salvage.
Current Evidence Based Guidelines
The Fluid Lavage of Open Wounds (FLOW) trial revolutionized the approach to wound irrigation. This international, randomized controlled trial demonstrated that very low-pressure irrigation with normal saline is safe, effective, and potentially superior to high-pressure pulsatile lavage or the use of castile soap, which were found to be locally toxic to osteoblasts and soft tissue cells.
The Eastern Association for the Surgery of Trauma (EAST) guidelines provide the current evidence-based recommendations for antimicrobial prophylaxis in open fractures. They strongly advocate for the administration of systemic antibiotics as soon as possible after injury, ideally within 60 minutes, and recommend limiting the duration of prophylactic antibiotics to 24-48 hours following definitive wound closure to minimize the risk of selecting for resistant organisms. Prolonged prophylactic antibiotic courses have not been shown to decrease the rate of deep infection and are associated with increased rates of Clostridioides difficile colitis and acute kidney injury.
Clinical & Radiographic Imaging
You Might Also Like