Masterclass in Ankle Arthroscopy: Impingement Syndromes and Surgical Techniques

Key Takeaway
Ankle arthroscopy is a highly effective, minimally invasive surgical intervention for treating anterior and posterior ankle impingement syndromes. Success relies on meticulous portal placement to avoid neurological injury, appropriate use of noninvasive distraction, and systematic arthroscopic debridement. This guide details the biomechanics, clinical evaluation, step-by-step surgical techniques, and postoperative rehabilitation protocols essential for optimizing patient outcomes and minimizing complications in foot and ankle arthroscopy.
INTRODUCTION TO ANKLE ARTHROSCOPY
Ankle arthroscopy has evolved from a purely diagnostic modality into a highly sophisticated therapeutic intervention. It is now considered the gold standard for managing a variety of intra-articular pathologies, most notably anterior and posterior ankle impingement syndromes, osteochondral lesions of the talus (OLTs), and arthrofibrosis. The complex, congruent anatomy of the tibiotalar joint demands meticulous surgical technique, precise portal placement, and a profound understanding of the surrounding neurovascular structures to minimize complications and optimize functional outcomes.
This comprehensive guide delineates the evidence-based principles of ankle arthroscopy, focusing on patient positioning, portal anatomy, the management of impingement syndromes, complication avoidance, and postoperative rehabilitation.
PATIENT POSITIONING AND OPERATING ROOM SETUP
Optimal visualization of the tibiotalar joint requires appropriate patient positioning and joint distraction. The ankle joint is inherently tight, and accessing the central and posterior compartments from an anterior approach necessitates mechanical separation of the articular surfaces.
Positioning Techniques
The patient is typically placed in the supine position for anterior ankle arthroscopy. A thigh tourniquet is applied to provide a bloodless surgical field. The operative leg is secured in a specialized leg holder, which stabilizes the thigh and allows the lower leg to hang freely, facilitating manipulation and the application of distraction forces.
Joint Distraction
Distraction is critical for safe instrument insertion and comprehensive joint evaluation. While invasive skeletal distraction (using calcaneal and tibial pins) was historically utilized, noninvasive distraction techniques are now the standard of care, significantly reducing the risk of pin-tract infections and neurovascular injury.
Noninvasive distraction utilizes a sterile strap applied around the hindfoot and midfoot, connected to a tensioning device secured to the operating table.


Surgical Warning: Excessive or prolonged noninvasive distraction can lead to neuropraxia, particularly of the superficial peroneal nerve or the sural nerve. Distraction forces should generally not exceed 30 lbs, and the duration of continuous distraction should be minimized, ideally released periodically during prolonged procedures.
SURGICAL ANATOMY AND PORTAL PLACEMENT
The cornerstone of safe ankle arthroscopy is precise portal placement. The anterior portals are the workhorses of ankle arthroscopy, providing access to the anterior compartment, the medial and lateral gutters, and the talar dome.
The Anteromedial Portal
The anteromedial portal is typically established first and serves as the primary viewing portal.
* Landmarks: Located just medial to the tibialis anterior tendon, at the level of the joint line.
* Technique: The joint line is palpated, and the portal site is localized using an 18-gauge spinal needle. The needle is directed toward the center of the joint, aiming slightly proximal to avoid iatrogenic cartilage damage to the talar dome. Once intra-articular placement is confirmed (often by injecting sterile saline to distend the joint), a vertical skin incision is made.
Clinical Pearl: Always use a "nick and spread" technique. Make a superficial skin incision with a #11 blade, then use a small hemostat to bluntly dissect down to the joint capsule. This minimizes the risk of injury to the saphenous vein and nerve, which lie in close proximity to the anteromedial portal.
The Anterolateral Portal
The anterolateral portal is the primary working portal. Its placement is more perilous due to the variable course of the superficial peroneal nerve (SPN).
* Landmarks: Located just lateral to the peroneus tertius tendon (or the extensor digitorum longus if the tertius is absent), at the joint line.
* Technique: Prior to incision, the path of the superficial peroneal nerve must be identified and marked. This is best achieved by asking the patient to actively plantarflex and invert the foot preoperatively, or by passively performing this maneuver after anesthesia, which often makes the nerve visible or palpable under the skin.

Once the nerve is marked, the portal is established under direct intra-articular visualization from the anteromedial portal. A spinal needle is used to localize the optimal trajectory. Following the skin incision, a blunt instrument (such as a hemostat or a blunt trocar) is used to penetrate the capsule, followed by the insertion of the arthroscopic shaver or other instrumentation.

ANKLE IMPINGEMENT SYNDROMES
Impingement syndromes of the ankle are characterized by painful mechanical limitations of terminal joint motion, caused by osseous or soft-tissue hypertrophy. They are broadly classified into anterior and posterior impingement.
Anterior Ankle Impingement
Anterior ankle impingement is frequently observed in athletes subjected to repetitive dorsiflexion microtrauma, such as soccer players ("footballer's ankle") and dancers.
Pathomechanics and Clinical Presentation
The condition can be driven by osseous structures, soft tissues, or a combination of both.
* Osseous Impingement: Caused by the formation of anterior tibial and talar osteophytes. These "kissing lesions" impinge upon each other during terminal dorsiflexion.
* Soft Tissue Impingement: Results from hypertrophic synovium, capsular thickening, or a thickened anteroinferior tibiofibular ligament (Bassett's ligament) that becomes entrapped between the tibia and talus.
Patients typically present with chronic, deep anterior ankle pain that is exacerbated by activities requiring forced dorsiflexion (e.g., squatting, stair climbing). Physical examination reveals localized tenderness along the anterior joint line and pain with passive forced dorsiflexion.
Diagnostic Imaging
Standard weight-bearing anteroposterior and lateral radiographs are the initial imaging modalities of choice. However, standard lateral views may underrepresent the size of anteromedial osteophytes due to the superimposition of the lateral malleolus. An anteromedial oblique view (AMI view) is often highly sensitive for detecting these lesions.
While MRI is excellent for evaluating osteochondral lesions and tendon pathology, standard MRI is not highly sensitive for isolated soft tissue impingement. Advanced imaging techniques, such as MR arthrography or contrast-enhanced, fat-suppressed, three-dimensional fast-gradient recalled acquisition in the steady state with radiofrequency spoiling (CE 3D-FSPGR MRI), offer superior sensitivity and specificity for soft tissue pathology, though they are less practical for routine clinical use.
Diagnostic Injections
A careful physical examination combined with a diagnostic intra-articular injection of local anesthetic can definitively pinpoint the diagnosis. If the patient experiences immediate, near-complete relief of anterior pain during provocative maneuvers following the injection, the diagnosis of intra-articular impingement is confirmed.
Surgical Warning: The routine use of intra-articular local anesthetics (particularly bupivacaine) has been scrutinized due to potential dose- and time-dependent cytotoxicity to chondrocytes observed in in vitro studies. However, there is currently a lack of robust in vivo clinical evidence substantiating significant chondrolysis following single diagnostic injections in the ankle. Surgeons should use the lowest effective concentration and volume.
Arthroscopic Management
If conservative measures (activity modification, NSAIDs, immobilization, physical therapy) fail, arthroscopic débridement is highly effective.
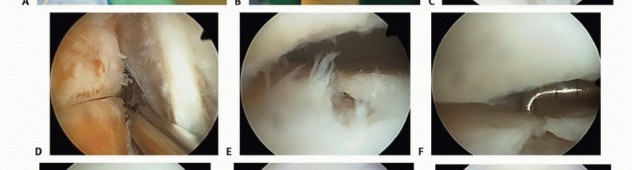
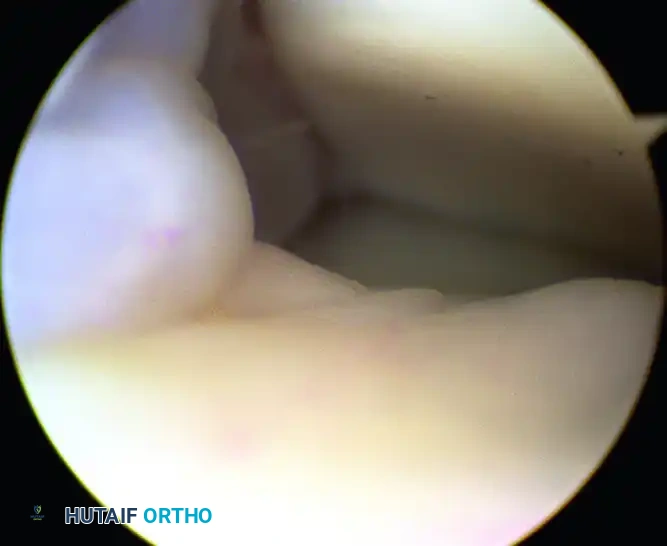
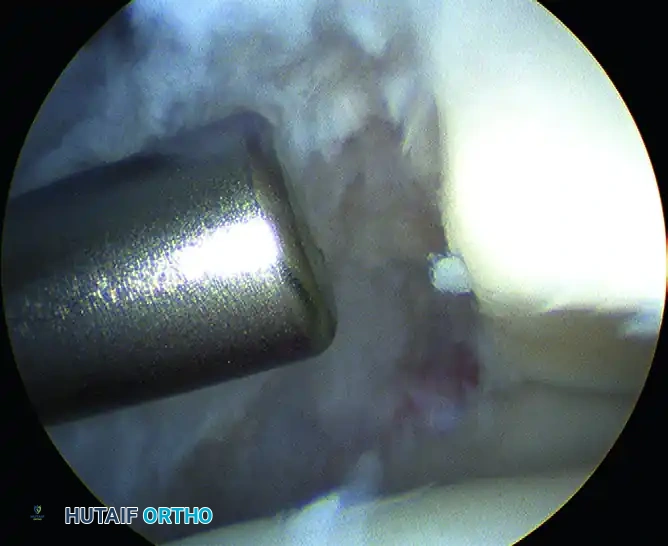
The procedure involves a systematic evaluation of the anterior compartment. Hypertrophic synovium and fibrotic scar tissue are resected using an arthroscopic shaver and radiofrequency ablation wands.

Once the soft tissue is cleared, the osseous anatomy is delineated. Anterior tibial and talar osteophytes are resected using a high-speed motorized burr or arthroscopic osteotomes. The resection must be thorough enough to restore impingement-free dorsiflexion, which is confirmed intraoperatively by releasing the distraction and taking the ankle through a full range of motion under direct visualization.
Outcomes: Level II evidence demonstrates success rates ranging from 73% to 96% for arthroscopic treatment of anterior impingement. According to a 2009 systematic review, there is a Grade B recommendation (fair evidence) supporting this intervention. Prognosis is generally excellent, though outcomes may be compromised in patients with diffuse, high-grade osteoarthritic changes or those lacking a definitive preoperative diagnosis. While osteophytes may radiographically recur over time, they are rarely symptomatic.
Posterior Ankle Impingement
Posterior ankle impingement syndrome (PAIS) is a classic "nutcracker" phenomenon occurring in the posterior compartment during forced plantar flexion. It is endemic among ballet dancers (en pointe positioning), gymnasts, and fast bowlers in cricket.
Pathomechanics and Clinical Presentation
The impingement occurs when structures are compressed between the posterior tibial plafond and the posterior superior aspect of the calcaneus. The most common anatomical culprits include:
* Os Trigonum: An unfused accessory ossicle posterior to the lateral tubercle of the posterior talar process.
* Stieda Process: An elongated, hypertrophic lateral tubercle of the posterior talar process.
* Soft Tissue: Hypertrophic posterior capsule, synovitis, or pathology of the flexor hallucis longus (FHL) tendon.
Patients present with deep posterior ankle pain. The hallmark clinical sign is a positive forced plantar flexion test. The examiner aggressively plantarflexes the ankle while applying overpressure; reproduction of the patient's deep posterior pain is considered a positive result.
Diagnostic Imaging and Management
Lateral radiographs typically reveal the presence of an os trigonum or a prominent posterior talar process. MRI is invaluable for identifying associated bone marrow edema within the os trigonum or talus, FHL tenosynovitis, and posterior capsulitis. A fluoroscopically or ultrasound-guided injection of local anesthetic and corticosteroid into the posterior impingement interval can provide both diagnostic confirmation and therapeutic relief.
When conservative management fails, surgical excision of the offending osseous structures and soft tissue débridement is indicated. This is increasingly performed via a two-portal endoscopic posterior approach with the patient in the prone position, utilizing posteromedial and posterolateral portals adjacent to the Achilles tendon.
COMPLICATIONS OF ANKLE ARTHROSCOPY
While generally considered safe, ankle arthroscopy carries a complication rate ranging from 9% to 17%. The tight confines of the joint and the proximity of vital neurovascular structures demand meticulous technique.
- Neurological Injury: This is the most common complication. The superficial peroneal nerve is at highest risk during anterolateral portal placement. The saphenous nerve is at risk medially, and the sural nerve is at risk during posterolateral portal placement. Strict adherence to the "nick and spread" technique and preoperative nerve marking are mandatory.
- Vascular Injury: Injury to the anterior tibial artery or the saphenous vein can occur with errant portal placement or aggressive anterior capsular resection.
- Infection and Joint Fistula: Superficial portal site infections and synovial fistulas can occur. Fistulas are often the result of early, aggressive range of motion before capsular healing or failure to adequately close the portal sites.
- Iatrogenic Articular Damage: Scuffing of the talar dome cartilage can occur during instrument insertion, particularly if joint distraction is inadequate.
- Complex Regional Pain Syndrome (CRPS): A devastating complication characterized by disproportionate pain, autonomic dysfunction, and trophic changes. Early recognition and aggressive multidisciplinary management are required.
- Other Complications: Deep venous thrombosis (DVT), compartment syndrome (due to fluid extravasation, especially if a capsular defect exists or pump pressures are excessively high), and instrument breakage.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative protocol is tailored to the specific procedures performed but generally follows a progressive, phased approach designed to protect the surgical site while restoring mobility and strength.
Phase I: Immediate Postoperative (Weeks 0-2)
- Immobilization: Patients are typically placed in a well-padded compressive dressing and a removable controlled ankle motion (CAM) walking boot.
- Weight-Bearing: For isolated soft tissue or bony impingement débridement, patients are generally allowed to bear weight as tolerated (WBAT) in the boot. However, they must be strictly cautioned against excessive activity, which can precipitate acute hemarthrosis, severe inflammation, and delayed wound healing.
- Edema Control: Strict elevation and cryotherapy are emphasized.
Phase II: Early Rehabilitation (Weeks 2-6)
- Wound Care: Sutures are removed at 10 to 14 days postoperatively.
- Physical Therapy: Formal physical therapy is initiated once wounds are fully healed and acute postoperative pain has subsided.
- Range of Motion: Active and active-assisted range of motion exercises (plantar flexion, dorsiflexion, inversion, eversion) are prioritized to prevent arthrofibrosis.
- Strengthening: Isometric strengthening progresses to isotonic exercises using resistance bands.
Phase III: Return to Activity (Weeks 6+)
- Proprioception: Aggressive proprioceptive and balance training (e.g., BAPS board, single-leg stance) is critical for restoring dynamic joint stability.
- Functional Progression: Patients gradually transition to sport-specific or work-specific functional drills. Return to high-impact sports or heavy labor is permitted once the patient demonstrates full, pain-free range of motion, symmetrical strength, and no effusion.
By adhering to strict indications, mastering the complex regional anatomy, and executing precise surgical techniques, orthopedic surgeons can utilize ankle arthroscopy to deliver profound pain relief and functional restoration for patients suffering from ankle impingement syndromes.
You Might Also Like