Anterior Cruciate Ligament (ACL) Injuries: Surgical Management
Key Takeaway
Anterior cruciate ligament (ACL) injuries are among the most common sports-related knee pathologies, with over 100,000 reconstructions performed annually in the United States. This comprehensive guide details the surgical management of ACL tears, encompassing applied biomechanics, advanced imaging diagnostics, and meticulous operative techniques. Emphasizing anatomic graft placement and evidence-based fixation methods, it provides orthopedic surgeons with a definitive framework for optimizing patient outcomes and restoring knee stability.
ANTERIOR CRUCIATE LIGAMENT INJURIES
Incidence and Modern Paradigm
The exact incidence of anterior cruciate ligament (ACL) injuries remains challenging to quantify definitively; however, epidemiological data estimates that approximately 200,000 ACL tears occur annually in the United States, resulting in over 100,000 surgical reconstructions each year.
The contemporary orthopedic controversy regarding the management of this injury has shifted significantly. The debate no longer centers primarily on whether surgery is necessary for the active patient, but rather focuses on the nuances of surgical technique—specifically, the choice of graft selection, anatomic versus isometric tunnel placement, and the method of graft fixation. In the past two decades alone, the proliferation of more than 2,000 scientific articles and numerous textbooks dedicated to the ACL underscores the rapid evolution and critical importance of this topic in operative sports medicine.
Applied Surgical Anatomy
The anterior cruciate ligament is a complex, intra-articular but extrasynovial structure. It is composed of longitudinally oriented bundles of type I collagen tissue arranged in fascicular subunits within larger functional bands. Because the ligament is enveloped by a synovial fold originating from the posterior capsule, it remains isolated from the synovial fluid.
Osseous Attachments:
* Tibial Footprint: The ACL inserts on the tibial plateau in a depressed area anterolateral to the anterior tibial spine, passing medial to the insertion of the anterior horn of the lateral meniscus. The tibial attachment site is anatomically larger and biomechanically more secure than the femoral site.
* Femoral Footprint: The ligament attaches to the posteromedial aspect of the lateral femoral condyle within the intercondylar notch.
Dimensions and Vascularity:
The average ACL is 31 to 35 mm in length with a cross-sectional area of 31.3 mm².
The primary blood supply is derived from the middle geniculate artery, which pierces the posterior capsule and enters the intercondylar notch near the femoral attachment. A secondary, yet vital, vascular contribution arises from the retropatellar fat pad via the inferior medial and lateral geniculate arteries. This secondary source plays a critical role in the healing response when the ligament is injured. The osseous attachments contribute negligibly to the ligament's overall vascularity.
Fig. 1: Sagittal anatomical representation of the anterior cruciate ligament demonstrating its oblique intra-articular course and extrasynovial envelope.
Innervation and Proprioception:
The posterior articular nerve, a branch of the tibial nerve, provides the primary innervation to the ACL. Histological analyses have identified intrafascicular nerve fibers consistent with pain transmission. Crucially, mechanoreceptors (Ruffini corpuscles, Pacinian corpuscles, and Golgi tendon organ-like endings) are concentrated at the ligamentous insertions—particularly at the femoral footprint—residing deep to the external synovial sheath. These receptors provide an essential afferent arc for knee proprioception and postural control.
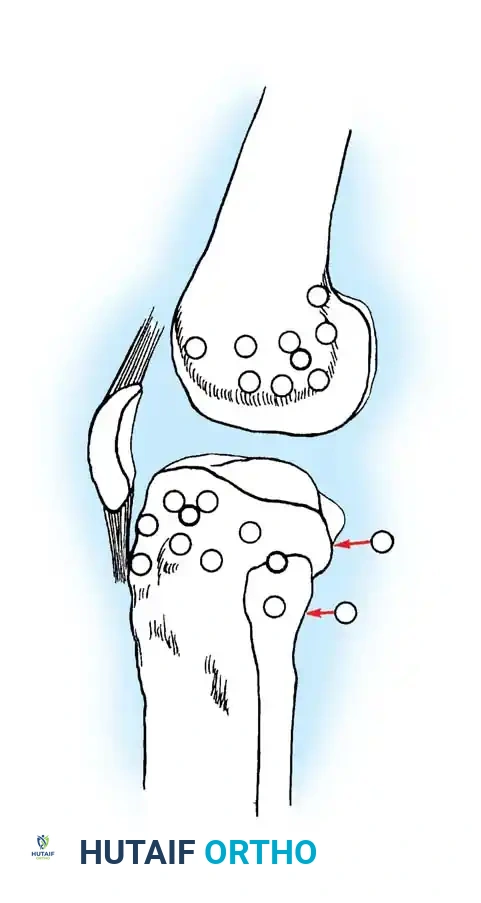
Fig. 2: Cross-sectional anatomy highlighting the fascicular arrangement and neurovascular penetration of the ACL.
Biomechanics and Kinematics
The ACL is the primary restraint to anterior tibial translation, providing approximately 85% of the resistance to the anterior drawer force when the knee is at 90 degrees of flexion and neutral rotation.
Functionally, the ACL is divided into two primary bundles named for their tibial insertion sites:
1. Anteromedial (AM) Bundle: Tightens in flexion and serves as the primary restraint to anterior translation during the Lachman test.
2. Posterolateral (PL) Bundle: Tightens in extension, providing the principal resistance against hyperextension and rotatory loads.
BIOMECHANICAL PEARL: Tension in the intact ACL is at its lowest between 30 and 40 degrees of knee flexion. The ligament also acts as a secondary restraint to internal tibial rotation and varus-valgus angulation at full extension.
In vivo kinematics dictate that the ACL's fibers are recruited differentially based on subtle three-dimensional changes in joint position. Consequently, the ligament can fail under varying load vectors depending on the knee's position at the moment of injury.
Biomechanical tensile testing of the ACL is highly dependent on specimen age, knee flexion angle, and the rate of applied load. Landmark studies by Noyes determined the ultimate load to failure of the native ACL to be 1725 ± 269 N, with a stiffness of 182 ± 33 N/mm. Subsequent studies by Woo et al. in younger cadaveric specimens demonstrated an ultimate load of 2160 ± 157 N and a stiffness of 242 ± 28 N/mm.
Clinical Evaluation: History and Physical Examination
The classic history of an ACL rupture involves a noncontact deceleration, pivoting, jumping, or cutting maneuver. Patients frequently report a sensation of the knee "popping out of joint" and spontaneously reducing, accompanied by an audible or palpable "pop." Immediate functional impairment is common; the patient typically falls and is unable to resume athletic activity.
Within 2 to 12 hours, a tense hemarthrosis develops. In the presence of an acute traumatic hemarthrosis, the statistical probability of an underlying ACL tear exceeds 70%.
Physical Examination:
Early examination—prior to the onset of severe effusion and muscle guarding—is highly diagnostic.
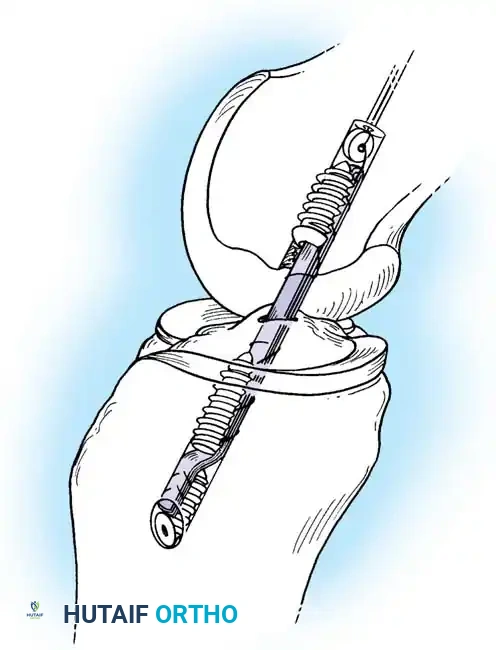
* Lachman Test: The most sensitive clinical test (95% sensitivity) for anterior tibial displacement. It is performed at 20 to 30 degrees of flexion. Increased excursion compared to the contralateral knee and the absence of a firm, distinct endpoint are diagnostic of an ACL rupture.
* Pivot Shift Test: Highly specific for anterolateral rotatory instability. It requires a relaxed patient and an intact medial collateral ligament (MCL). It is often best elicited under anesthesia or in chronic cases where muscle guarding is absent.
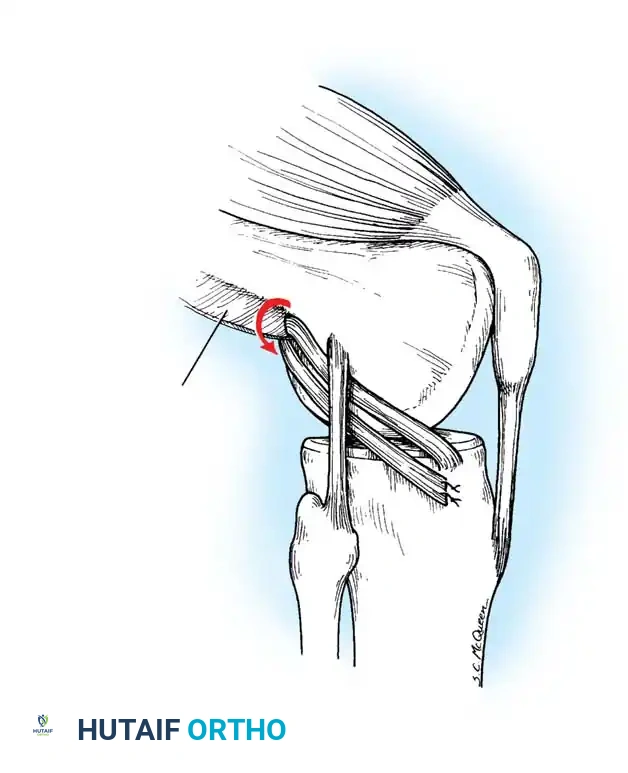
Fig. 3: Clinical demonstration of the Lachman test, emphasizing the stabilization of the distal femur and anterior translation of the proximal tibia.
Instrumented Arthrometry:
Devices such as the KT-1000/2000 arthrometer provide objective quantification of anterior laxity. A manual maximal displacement resulting in a side-to-side difference of ≥ 3 mm is present in 90% of knees with an acute ACL injury.
Diagnostic Imaging
While the diagnosis of an ACL tear is primarily clinical, imaging is essential for confirming the diagnosis and identifying concomitant pathology.
Radiographs:
Standard weight-bearing orthogonal views are mandatory. While often normal, specific radiographic signs are highly indicative of ACL injury:
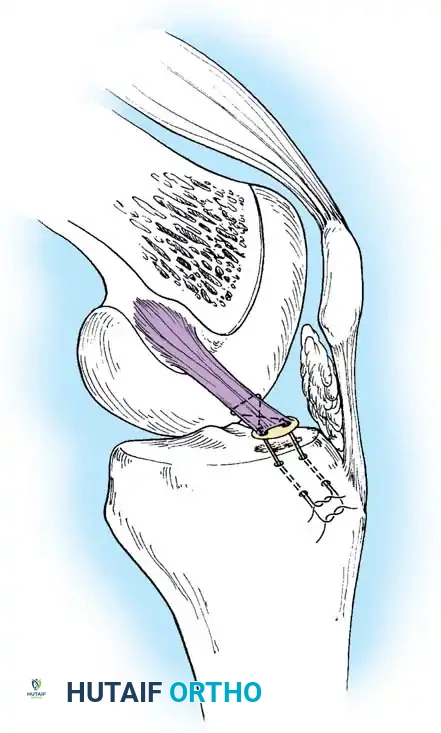
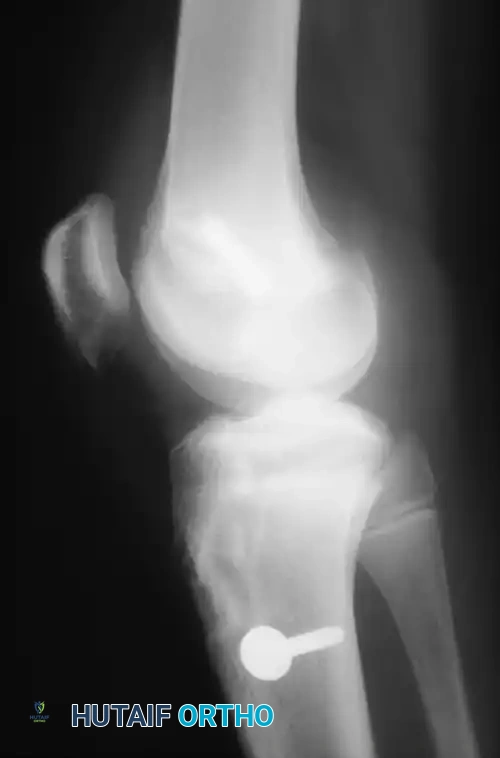
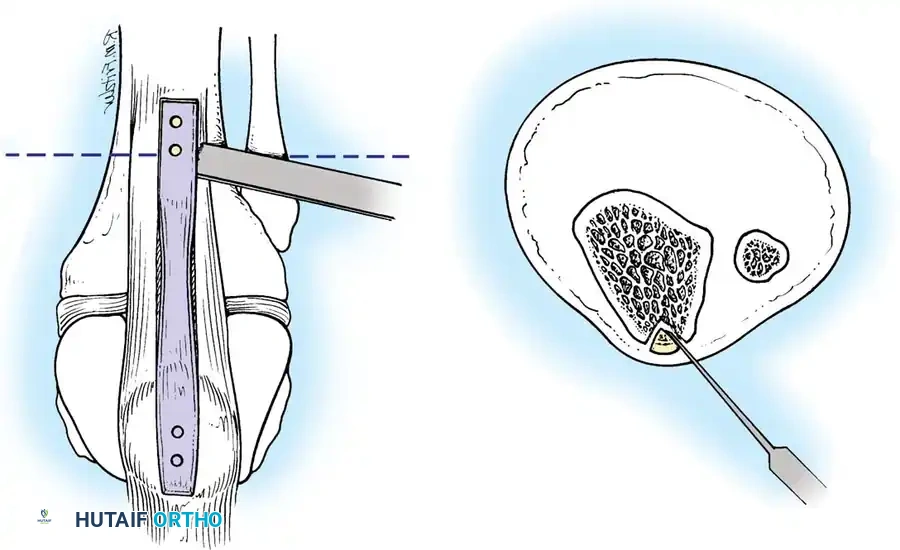
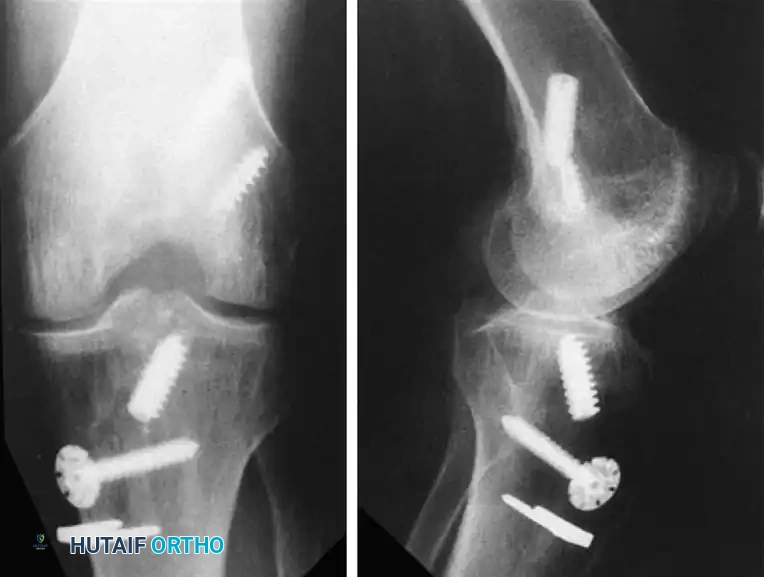
* Segond Fracture: An avulsion fracture of the anterolateral tibial capsule. This finding is considered pathognomonic for an ACL tear.
* Tibial Eminence Fracture: Indicates an avulsion of the tibial attachment of the ACL, more commonly seen in pediatric populations.
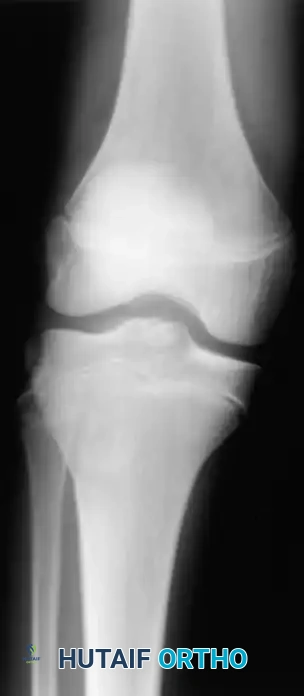
Fig. 43-101 Avulsion fracture of the tibia (Segond fracture) with anterior cruciate ligament tear.
Magnetic Resonance Imaging (MRI):
MRI is the gold standard advanced imaging modality, with reported accuracies approaching 95% to 100%. Because the ACL courses obliquely, standard orthogonal sagittal planes may not capture the entire ligament.
RADIOGRAPHIC PEARL: Utilizing a nonorthogonal plane—achieved by externally rotating the knee approximately 15 degrees during the scan—allows for visualization of the entire ACL in a single continuous frame.
MRI is also highly sensitive for detecting associated bone bruises (microtrabecular fractures), which occur in up to 80% of acute ACL tears. These are typically located on the lateral femoral condyle and the posterolateral tibial plateau, reflecting the footprint of the pivot-shift mechanism.
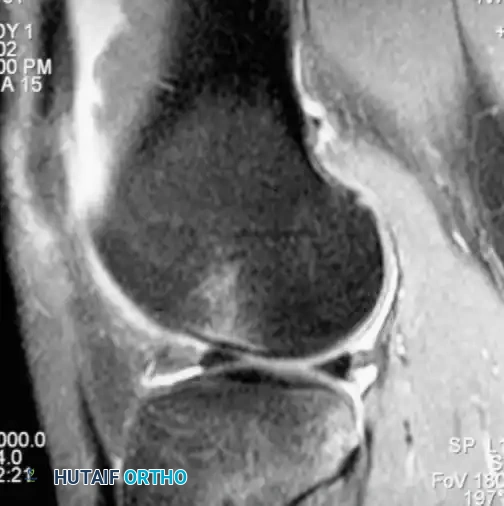
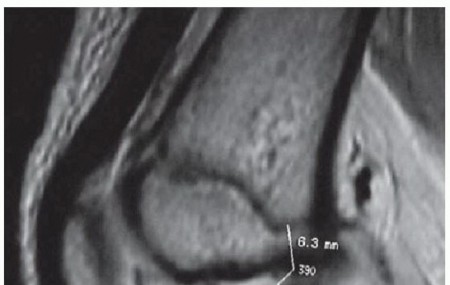
Fig. 43-102 Magnetic resonance image shows bone bruise after anterior cruciate ligament tear.
Epidemiology, Risk Factors, and Natural History
Gender Disparities and Risk Factors:
Data from the NCAA Injury Surveillance System demonstrates significantly higher ACL injury rates in female athletes participating in soccer, basketball, and rugby compared to their male counterparts. The etiology is multifactorial:
* Extrinsic Factors: Muscle strength imbalances, shoe-surface interface, and landing mechanics.
* Intrinsic Factors: Joint laxity, hormonal fluctuations (estrogen, progesterone, relaxin), limb alignment, and intercondylar notch dimensions.
* Neuromuscular Control: Hewett et al. demonstrated that female athletes who subsequently tore their ACLs exhibited significantly different landing kinematics, notably an 8-degree greater knee abduction (valgus) angle upon landing compared to uninjured cohorts.
Notch Width Index:
Souryal and Freeman identified intercondylar notch stenosis as a significant risk factor for noncontact ACL tears. The Notch Width Index is the ratio of the width of the intercondylar notch to the width of the distal femur at the level of the popliteal groove.
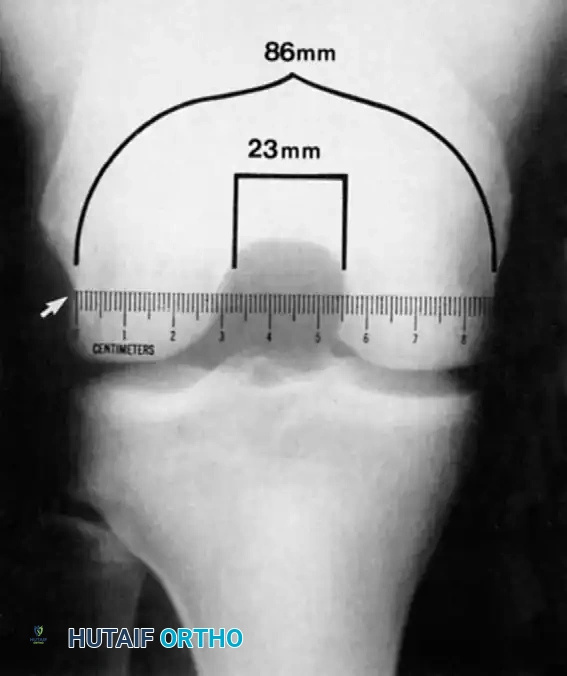
Fig. 43-103 Notch width index is ratio of width of intercondylar notch to width of distal femur at level of popliteal groove (arrow). Ruler must be parallel to joint line. Narrowest portion of notch at level of ruler is to be measured.
Natural History and Joint Degeneration:
The natural history of the ACL-deficient knee in an active individual is characterized by recurrent instability, leading to secondary intra-articular damage.
* Meniscal Tears: Present in 50% to 70% of acute injuries (lateral meniscus most common initially). In chronic ACL deficiency, the medial meniscus is subjected to massive shear forces, leading to a high rate of late medial meniscal tears.
* Biochemical Alterations: Cameron et al. found that chronic ACL-deficient knees exhibit markedly elevated levels of proinflammatory cytokines (IL-1, TNF-α) and decreased protective anti-inflammatory proteins (IL-1ra). Lohmander et al. reported elevated stromelysin-1 and TIMP-1 up to 18 years post-injury, driving the progression of post-traumatic osteoarthritis (PTOA).
SURGICAL RECONSTRUCTION: STEP-BY-STEP TECHNIQUE
The goal of ACL reconstruction is to restore the native kinematics of the knee through anatomic graft placement, rigid fixation, and aggressive postoperative rehabilitation.
1. Patient Positioning and Examination Under Anesthesia (EUA)
The patient is placed supine on the operating table. A thorough EUA is performed to confirm the pivot shift and assess for concurrent collateral ligament laxity. A tourniquet is applied to the proximal thigh. The leg is positioned either in a standard leg holder or with a lateral post to allow full range of motion and valgus stress for medial compartment access.
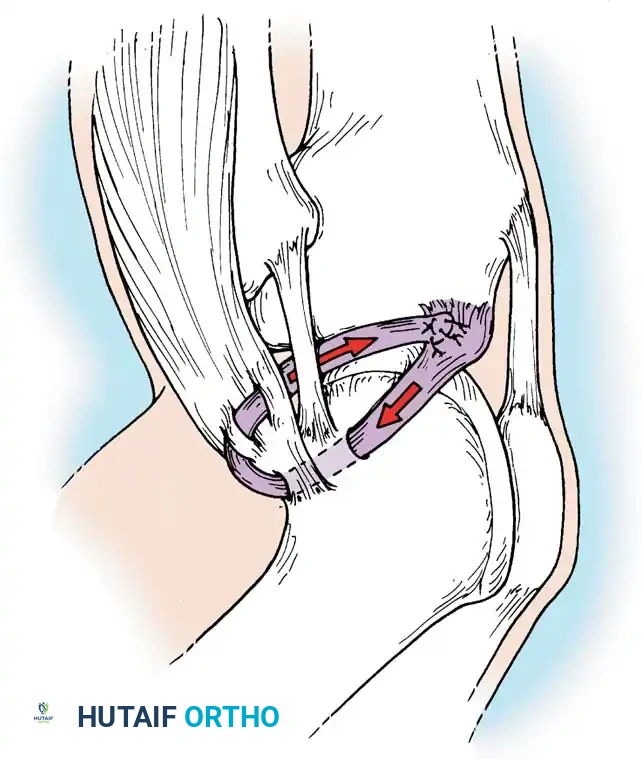
Fig. 4: Standard operating room setup with the patient supine and the operative leg secured in a thigh holder to allow dynamic manipulation.
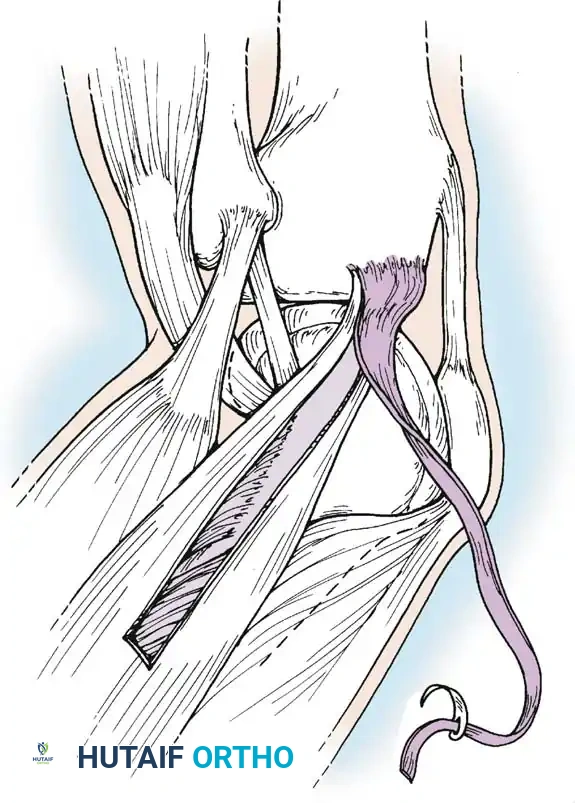
Fig. 5: Alternative positioning utilizing a lateral post, facilitating hyperflexion and figure-of-four positioning.
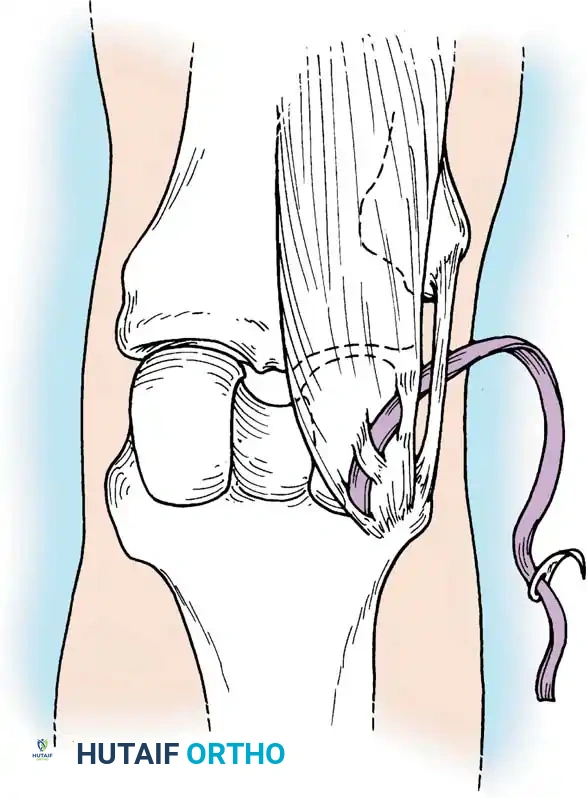
Fig. 6: Application of valgus stress against the lateral post to open the medial compartment for meniscal evaluation.
2. Graft Harvest and Preparation
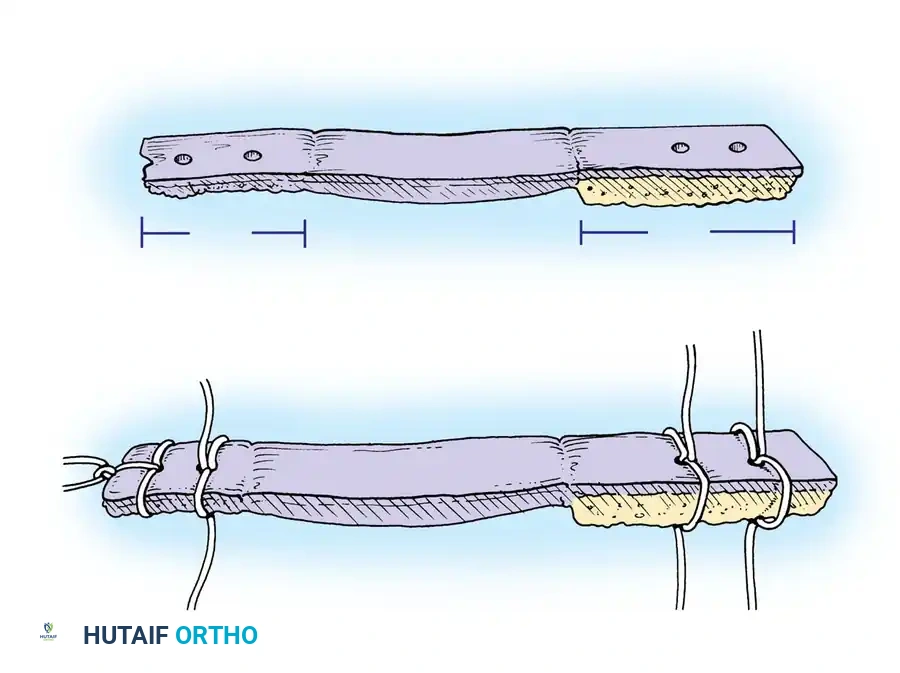
Graft selection is tailored to the patient's age, activity level, and surgeon preference. The two most common autografts are the Bone-Patellar Tendon-Bone (BTB) and the quadrupled Hamstring (Gracilis and Semitendinosus) graft.
Bone-Patellar Tendon-Bone (BTB) Harvest:
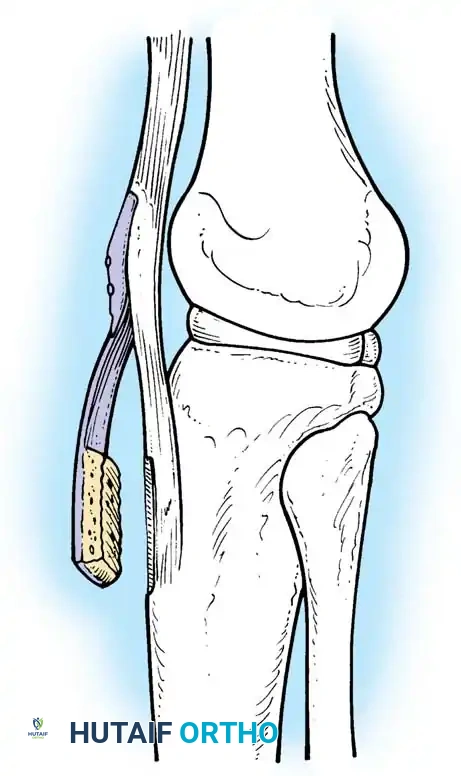
A longitudinal incision is made from the inferior pole of the patella to the tibial tubercle. The central third of the patellar tendon (typically 9-10 mm wide) is harvested with trapezoidal bone blocks from the patella and tibia.
Fig. 7: Incision and exposure for the central third bone-patellar tendon-bone autograft harvest.
Fig. 8: Oscillating saw technique for harvesting the patellar and tibial bone blocks, ensuring a trapezoidal cut to prevent stress risers.
Hamstring Harvest:
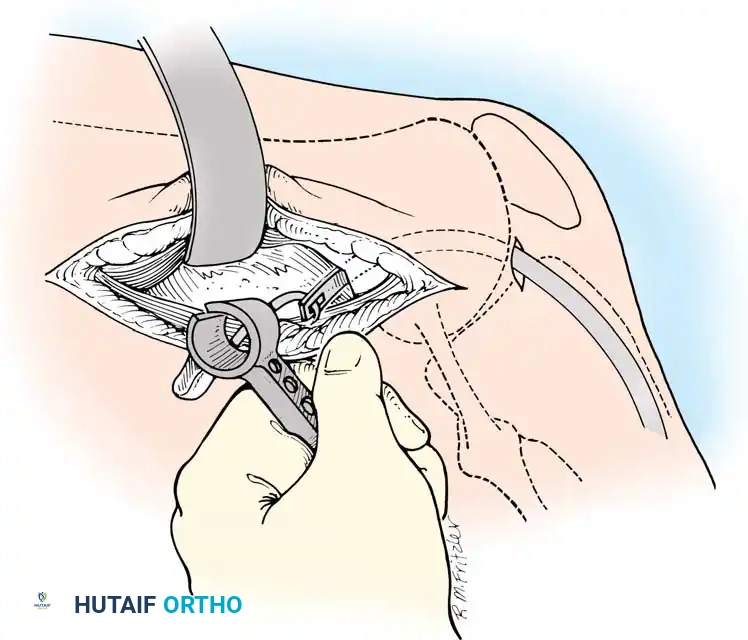
An oblique incision is made over the pes anserinus. The sartorial fascia is incised, and the gracilis and semitendinosus tendons are identified, isolated, and harvested using an open-ended tendon stripper.
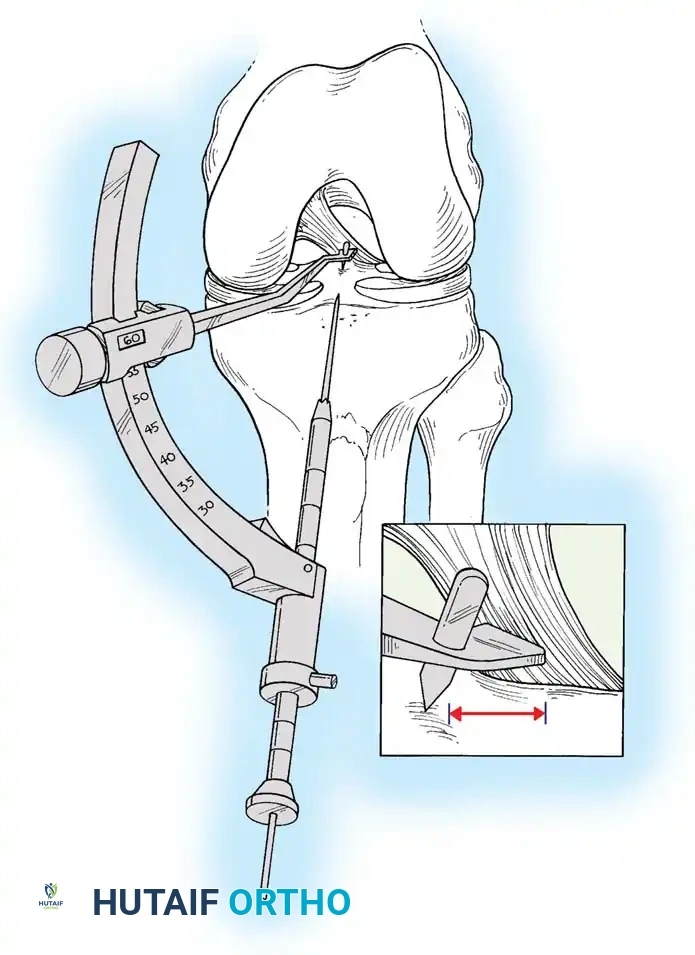
Fig. 9: Isolation of the semitendinosus and gracilis tendons prior to stripping. Care must be taken to release all accessory fascial bands to prevent premature graft amputation.
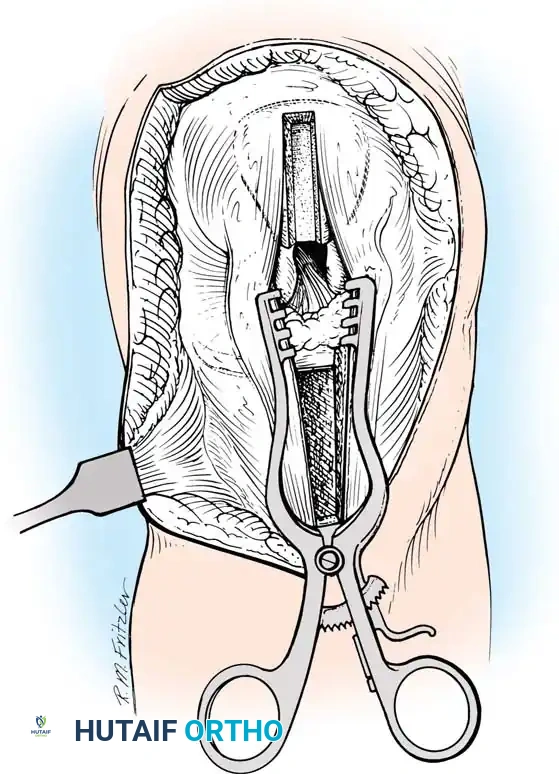
3. Diagnostic Arthroscopy and Intercondylar Notch Preparation
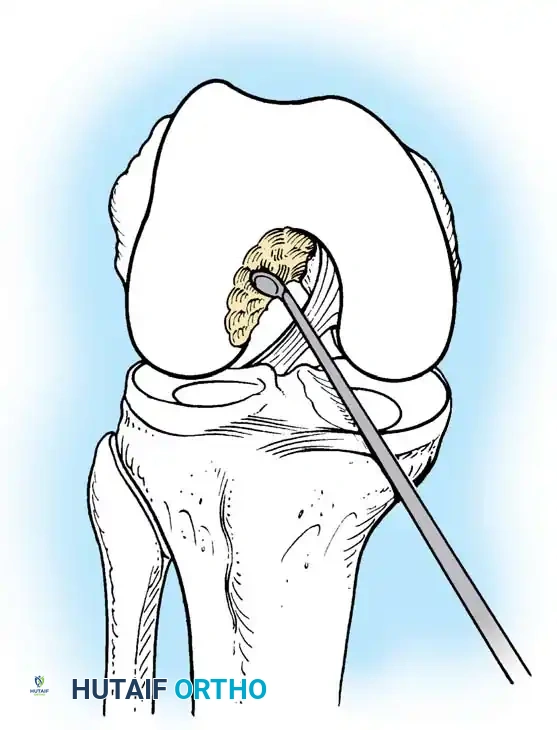
Standard anterolateral (viewing) and anteromedial (working) portals are established. A comprehensive diagnostic sweep is performed, addressing any meniscal or chondral pathology. The ruptured ACL stump is debrided, preserving the tibial footprint to aid in anatomic tunnel placement and preserve mechanoreceptors.
If notch stenosis is present, a limited notchplasty is performed using a motorized burr to prevent graft impingement in full extension.
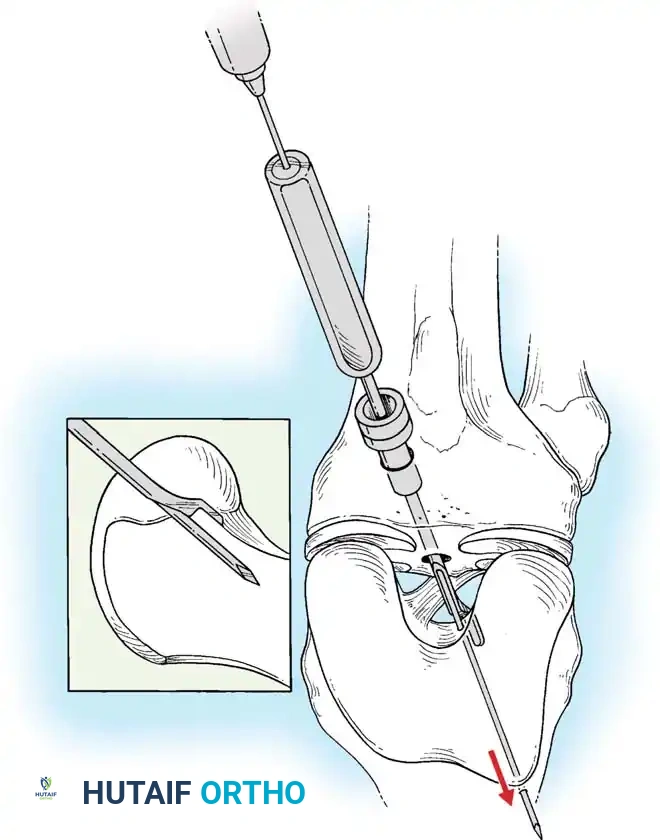
Fig. 10: Arthroscopic view of the intercondylar notch prior to debridement, demonstrating the torn ACL fibers obscuring the lateral femoral condyle.
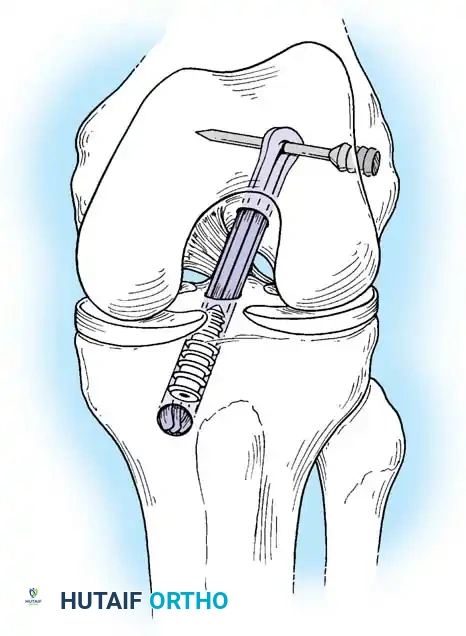
Fig. 11: Execution of a targeted wall notchplasty using a motorized burr to expand the intercondylar space and prevent graft impingement.
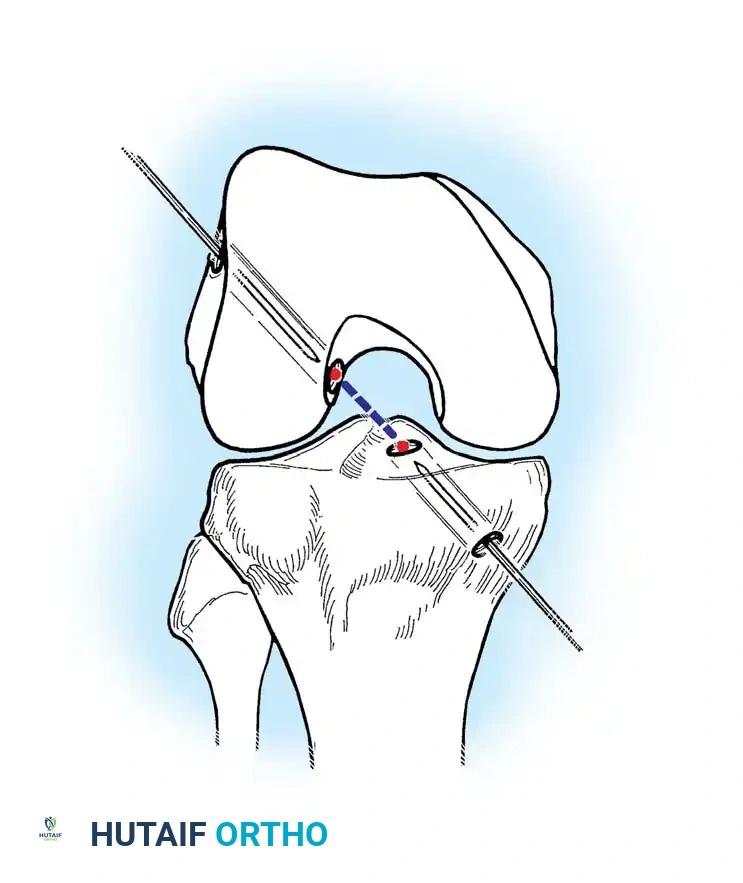
4. Femoral Tunnel Preparation
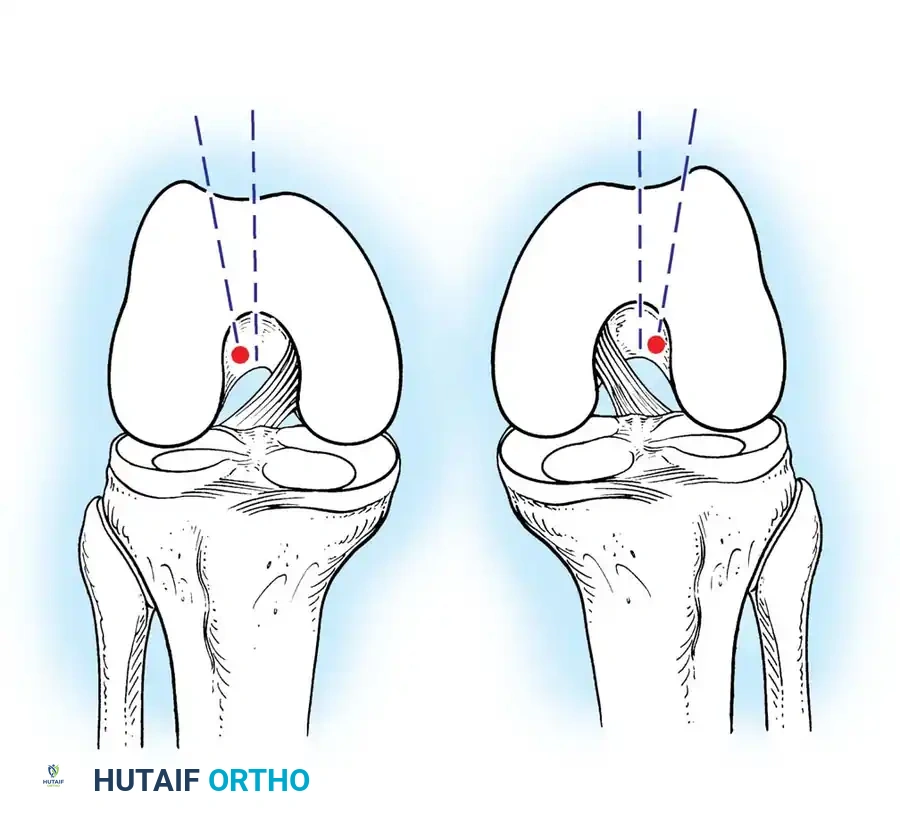
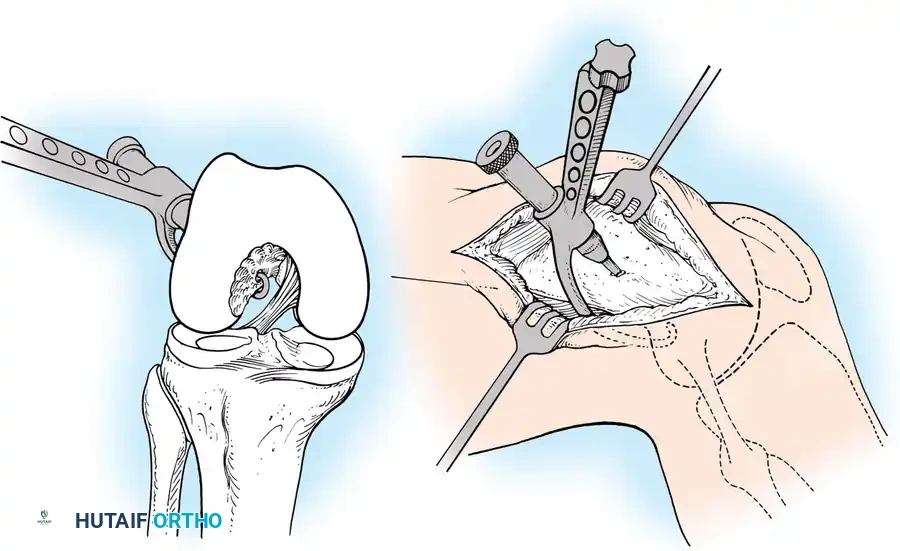
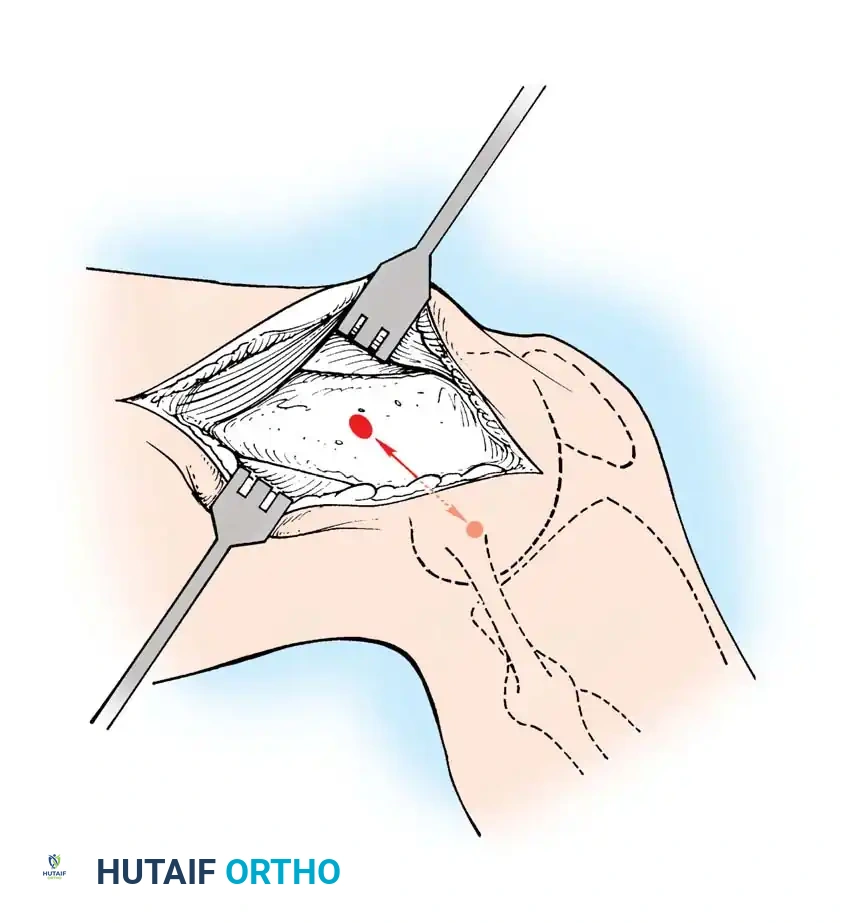
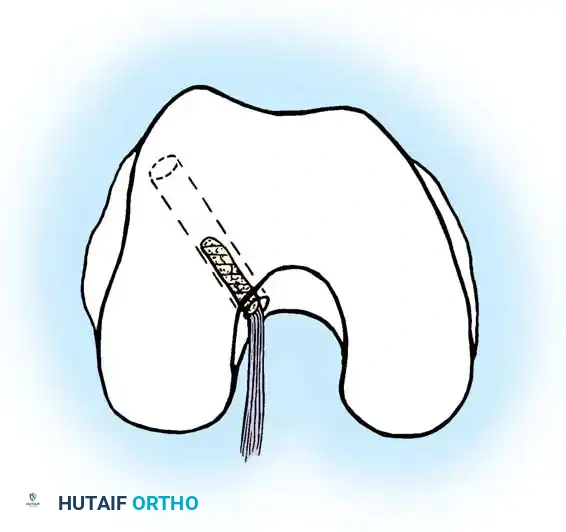
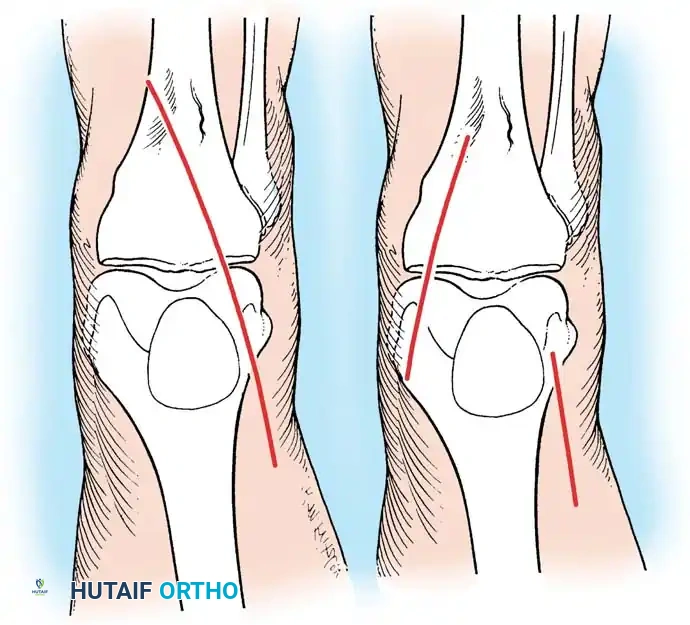
Anatomic placement of the femoral tunnel is the most critical step in restoring rotational stability. The tunnel should be placed at the center of the native femoral footprint, typically at the 10 o'clock (right knee) or 2 o'clock (left knee) position.
This can be achieved via a transtibial approach or an independent anteromedial (AM) portal approach. The AM portal approach allows for more anatomic, lower placement of the femoral tunnel independent of the tibial tunnel trajectory.
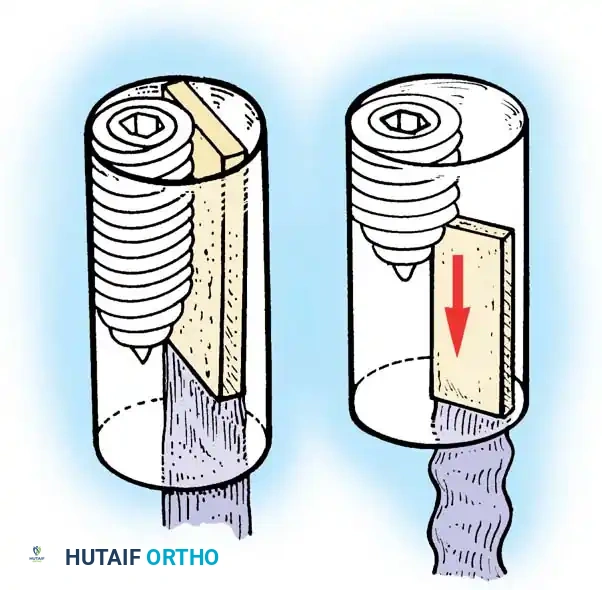
Fig. 12: Identification of the femoral footprint. The over-the-top guide is positioned to reference the posterior cortical margin of the lateral femoral condyle.
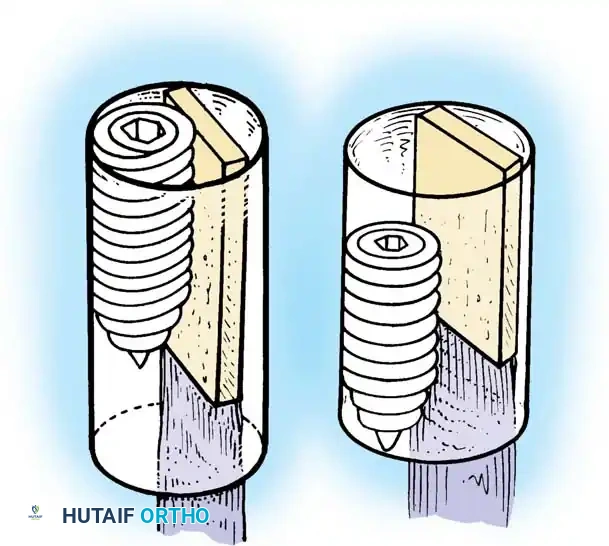
Fig. 13: Placement of the femoral offset guide through the anteromedial portal. The knee is hyperflexed to >110 degrees to prevent posterior wall blowout.


You Might Also Like