Templating for Primary THA: Optimize Outcomes & Avoid Pitfalls
Key Takeaway
This topic focuses on Templating for Primary THA: Optimize Outcomes & Avoid Pitfalls, Templating for primary total hip arthroplasty (THA) is crucial for accurate preoperative planning, indicated for every case. It prevents complications like dislocation and leg length inequality by ensuring precise component alignment and position. This process helps decide fixation type, optimize implant size, restore the center of rotation, and alert surgeons to potential intraoperative difficulties, improving overall surgical success.
Introduction
1. Templating is a familiar terminology to orthopedic surgeons whether it is used preoperatively or intraoperatively.
1. Templating has been extensively used for preoperative planning of fracture fixation and total joint arthroplasty.
2. Intraoperative templates have been routinely used to know the size and the shape of metallic plates before the latter are selected and contoured to fit the corresponding bone surfaces.
3. Templating in total hip arthroplasty (THA) is not new, and it has long been used with traditional radiographic films and printed templates (acetates).
2. Digital templating has become possible with the introduction of digital radiography and computers into clinical practice.
-
This chapter outlines the indications and rationale for templating, explains different methods used, and then describes in more detail the technical steps and possible pitfalls.
Indications - Templating is indicated for every primary THA whether it is a straightforward or a complicated case.
- The hip joint is deep and, even with maximum exposure, many of the anatomic details and landmarks are not visible.
- The introduction of limited and minimally invasive techniques for THA has increased the demand for accurate and reliable preoperative planning.
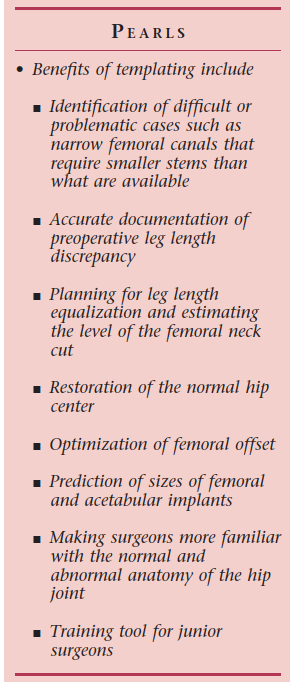
- Templating can help in deciding the type of fixation needed, whether cemented, cementless, or hybrid.
- Bone stock is important, and it is useful to know in advance the cup size and the level of femoral neck cut to facilitate minimal bone removal.
-
Center of rotation has to be restored, offset needs to be optimized, and alignment of the stem should be anatomic.
55 ### Templating for Primary THA - Leg length, ideally, should be equal particularly after the increasing rate of litigation in North America due to leg length discrepancy.
- Templating alerts the surgeon to otherwise unexpected intraoperative difficulties and complications.
- Surgeons should be aware well in advance regarding unusual implants or instruments. Larger femoral heads or constrained cups may be required if a higher risk of dislocation is expected.
- The difficulty related to keeping a complete inventory of implants and instrumentation is another concern. In smaller institutions or centers where the turnover of THA cases is not large, manufacturers may supply a limited stock of implants. In such cases, templating is useful in predicting implant sizes and in providing adequate inventory.
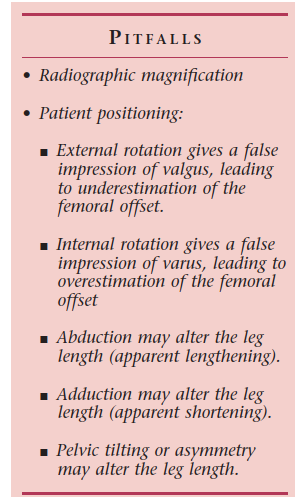
- Radiographs should include an anteroposterior (AP) view of the pelvis (both hips) and both AP and lateral views of the affected hip that include the acetabulum and the proximal third of the femur.
- Patient positioning is critical to avoid misleading information.
- Templating can be done whether using printed acetates or specific software. The printed acetates may be applied to radiographic films or digital images.
- Radiographic films are still frequently used in many hospitals around the world, but the use of digital imaging is on the rise.
-
Traditional Templating
- In this method, surgeons lay and match printed acetates (templates) of implants over radiographic films. The acetates are usually magnified to a certain number of degrees to compensate for x-ray magnification. Manufacturers usually provide information about the percentage of magnification of the templates.
Templating with Acetates over
Digital Images
-
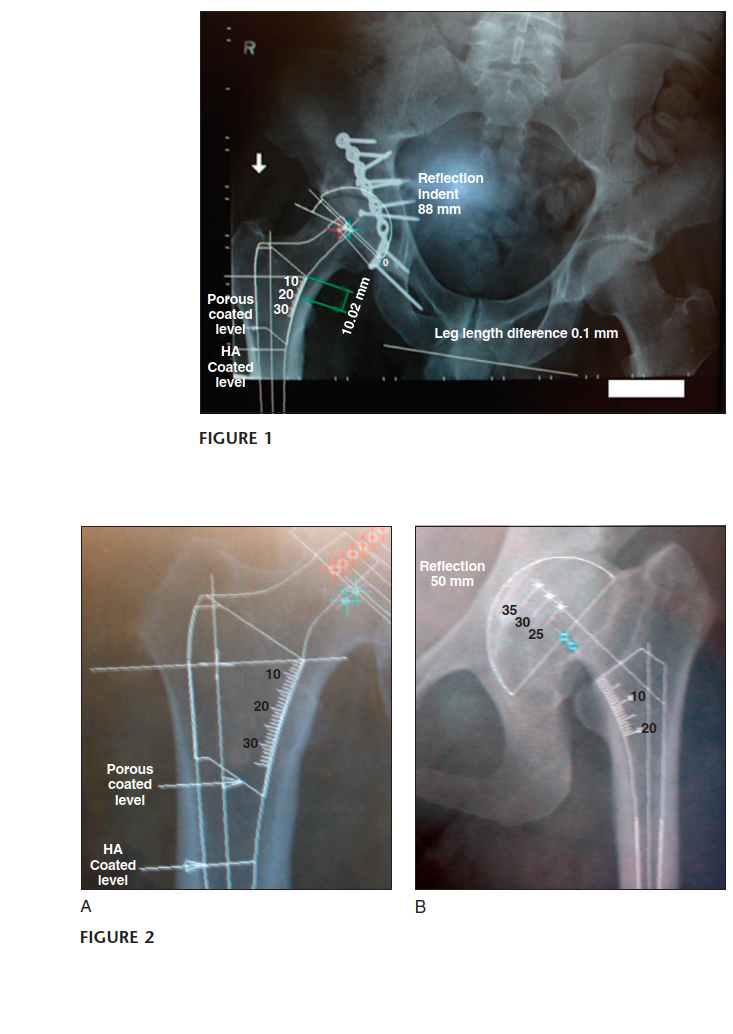
Digital Templating
- In this method, the templating is entirely performed using specific software. There is automatic scaling once the degree of magnification is selected, thus correcting the magnification on the displayed radiographic images.
-
The software has a library of implants from different
manufacturers in various sizes, which can be imported and superimposed on the radiographic images in coronal or sagittal views. The implants can be manipulated by translation or angulation until the optimal position is achieved. Measurements of leg length, distances, and angles can be done in decimals. - Several software systems are available, such as OrthoView, OrthWork, VAMP, Sectra, mdesk, Merge, mediCAD, IMPAX, and EndoMap.
- Ideally, templating should be done in outpatient clinics to give enough notice to obtain the required implants and instruments. For straightforward cases, templating can be done in the operating room just before surgery.
- History and physical examination are indispensable to preoperative planning and templating.
- Patients should be asked if they are aware of leg length discrepancy. Do they notice it (symptomatic or not)? Has it been measured or corrected by a heel lift?
- Inquire about a history of previous surgery for the same or contralateral side.
- Read old hospital notes to obtain implant sizes for previous THA (contralateral).
- Measure leg lengths and account for pelvic obliquity and flexion deformity. In the case of pain or spasm, the measurement should be deferred until the patient is anesthetized.
- Information obtained from history and examination, particularly leg length measurement, should be applied during templating.
-
Good-quality radiographs are essential and should include anteroposterior and lateral views
extending beyond the expected tip of the femoral component and the cement restrictor. The position of the patient and the leg during radiographic examination is critical (see Pitfalls above).
Templating for revision procedures should be done in the outpatient clinic and should be repeated just before surgery to take into consideration any changes that occurred during the waiting time for surgery.
Procedure
Step 1: Radiographic Assessment
- Perform routine radiographic assessment looking at the quality of bone, amount of bone stock, dysplasia, osteophytes, and other abnormalities.
- Make a preliminary decision on what type of implants to be used, whether cemented, cementless, or hybrid implants.
- For uncemented femoral components, decide whether distal or proximal loading stems are to be used. 58
Templating for Primary THA
- In case of a contralateral total hip replacement, determine the type of implants used and consider templating for the same implant type and size.
Step 2: Correct Radiographic Magnification
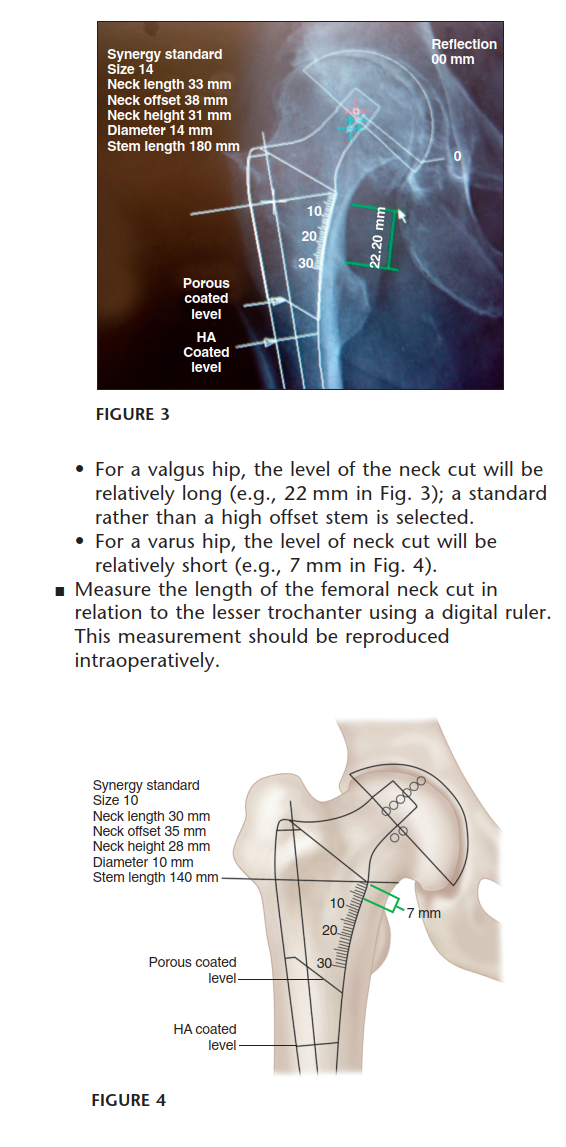


You Might Also Like