Surgical Management of Spinal Deformities in Neurofibromatosis

Key Takeaway
Neurofibromatosis type 1 (NF-1) frequently presents with complex spinal deformities, categorized as nondystrophic or dystrophic. Dystrophic curves are characterized by short-segment, sharp angulations with severe vertebral wedging and penciled ribs. Management requires rigorous preoperative MRI to rule out intraspinal lesions. While nondystrophic curves mimic idiopathic scoliosis, dystrophic kyphoscoliosis often mandates combined anterior and posterior arthrodesis with robust strut grafting to prevent pseudarthrosis and progression.
UNUSUAL CAUSES OF SCOLIOSIS: NEUROFIBROMATOSIS
Neurofibromatosis is a complex, hereditary hamartomatous disorder derived from the neural crest. The aberrant proliferation of these hamartomatous tissues can manifest across any organ system, presenting unique and often severe challenges in orthopedic surgery. Clinically, the disorder is bifurcated into two primary classifications: peripheral neurofibromatosis (NF-1) and central neurofibromatosis (NF-2).
The classic peripheral form, NF-1 (historically described by von Recklinghausen), is an autosomal dominant condition affecting approximately 1 in 4,000 individuals. Pathophysiologically, patients with NF-1 are predisposed to developing Schwann cell tumors and distinct pigmentation abnormalities. Orthopedic manifestations are profoundly common in this cohort, with spinal deformity—most notably scoliosis—reigning as the most frequent osseous defect. Conversely, NF-2 is a much rarer autosomal dominant disorder characterized predominantly by bilateral acoustic neuromas; it notably lacks the bone involvement and orthopedic manifestations seen in NF-1.
Clinical Diagnosis of Neurofibromatosis Type 1
The diagnosis of NF-1 remains primarily clinical, relying on a strict set of criteria. For a definitive diagnosis, a patient must exhibit at least two of the following pathognomonic features:
- A minimum of six café au lait spots (larger than 1.5 cm in diameter in postpubertal patients, and larger than 5 mm in prepubertal patients).
- Two or more neurofibromas of any histological type, or one plexiform neurofibroma.
- Axillary or inguinal freckling (Crowe sign).
- Optic glioma.
- Two or more iris Lisch nodules (identified via slit-lamp examination).
- A distinctive osseous lesion (e.g., sphenoid dysplasia or thinning of long bone cortex, with or without pseudarthrosis).
- A first-degree relative with a definitive diagnosis of NF-1 based on the aforementioned criteria.
Clinical Pearl: Functional scoliosis in NF-1 patients may not always be structural. Always evaluate for leg-length discrepancies resulting from lower extremity hypertrophy or congenital dysplasia of the long bones (such as anterolateral bowing of the tibia) before diagnosing structural spinal deformity.
EPIDEMIOLOGY AND CLASSIFICATION OF SPINAL DEFORMITIES
Scoliosis is the hallmark osseous defect in NF-1. Epidemiological data from Crawford and Bagamery indicate that in a generalized pool of scoliosis patients, approximately 3% have underlying neurofibromatosis. Conversely, within a dedicated population of neurofibromatosis patients, up to 60% exhibit some form of spinal disorder. Akbarnia et al. refined this, noting structural spinal deformities in 10% of an unselected cross-section of 220 NF patients, which is widely accepted as the true prevalence rate.
Spinal deformities in NF-1 are biomechanically and radiographically divided into two distinct categories: Nondystrophic and Dystrophic.

Nondystrophic Scoliosis
Nondystrophic deformities behave biomechanically like typical adolescent idiopathic scoliosis (AIS). The curve patterns, progression risks, and responses to conservative treatment closely mirror those of idiopathic, congenital, or Scheuermann kyphosis etiologies. In these cases, the underlying NF-1 diagnosis appears to have minimal influence on the curve's natural history, with one critical exception: the phenomenon of "modulation."
Dystrophic Scoliosis
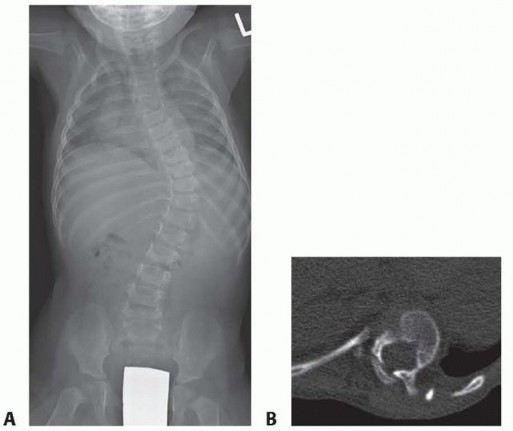
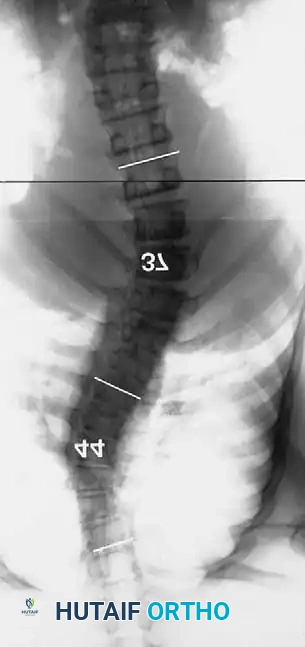
Dystrophic scoliosis is the most aggressive and challenging variant. It is characterized by a short-segment, sharply angulated curve. Radiographically, dystrophic curves present with a constellation of severe structural anomalies:
* Severe wedging of the apical vertebral bodies.
* Extreme axial rotation of the vertebrae.
* Posterior scalloping of the vertebral bodies (often secondary to dural ectasia).
* Spindling (thinning) of the transverse processes.
* Enlargement of the neural foramina.
* "Penciled ribs": Rotation of the ribs 90 degrees in the anteroposterior direction, making them appear abnormally thin and dysplastic.

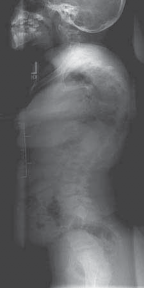
Curves with significant sagittal plane deformity are highly prevalent in dystrophic scoliosis. Neurofibromatosis kyphoscoliosis is particularly notorious, characterized by acute, rigid angulation in the sagittal plane and striking destruction or deformity of the vertebral bodies near the apex. Severe thoracic lordoscoliosis has also been documented by Winter, presenting unique respiratory and biomechanical challenges.
Surgical Warning: Observation of a progressing dystrophic spinal deformity is strictly unjustified. Because only a fraction of dystrophic curves remain small, early operative intervention is the gold standard to prevent catastrophic neurological compromise and severe cardiopulmonary restriction.
PREOPERATIVE EVALUATION AND ADVANCED IMAGING
The preoperative workup for an NF-1 patient with spinal deformity must be exhaustive. The presence of intraspinal lesions—such as pseudomeningoceles, dural ectasia, or intraspinal neurofibromas (dumbbell tumors)—must be definitively ruled out before any surgical instrumentation is attempted.

Impingement of these occult lesions against the spinal cord during the correction maneuvers of instrumentation has been documented to cause acute, irreversible paraplegia.
Routine total spine Magnetic Resonance Imaging (MRI) is mandatory. Ramachandran et al. demonstrated that 37% of NF-1 patients (in both dystrophic and nondystrophic groups) harbored intraspinal and paraspinal neurofibromas, often adjacent to the convexity of the curve. While MRI is superior for evaluating cord displacement and the subarachnoid extent of neurofibromas, severe kyphoscoliotic deformities may render MRI inadequate due to artifact and complex multi-planar anatomy. In such cases, complete high-volume CT myelography in the prone, lateral, and supine positions is required to accurately map the spinal canal.
MANAGEMENT OF NONDYSTROPHIC CURVES
Nondystrophic curves share the prognosis and evolutionary trajectory of idiopathic curves, albeit with a statistically higher risk of pseudarthrosis following operative fusion.
The Concept of Modulation
Crawford highlighted a critical phenomenon termed "modulation"—the transition of a nondystrophic curve into a dystrophic one over time. A spinal deformity developing before 7 years of age demands hyper-vigilant observation. If the curve acquires three "penciled" ribs or a combination of three dystrophic radiographic features, rapid clinical progression is almost a certainty.
Treatment Guidelines
- Observation: Curves less than 20 to 25 degrees are observed clinically and radiographically.
- Bracing: If no dystrophic changes are present, a TLSO brace is prescribed when the deformity progresses to 30 degrees.
- Surgical Fusion: If the deformity exceeds 40 to 45 degrees, posterior spinal fusion with segmental hook or pedicle screw instrumentation is recommended.


Modern segmental instrumentation (e.g., Cotrel-Dubousset principles) utilizing high-density pedicle screw constructs provides excellent correction without the absolute need for postoperative immobilization, yielding results comparable to AIS cohorts.
MANAGEMENT OF DYSTROPHIC SCOLIOSIS
The management of dystrophic curves is dictated by two primary factors: the presence or absence of a kyphotic deformity, and the patient's neurological status.
Surgical Warning: Brace treatment is universally contraindicated for typical dystrophic curves in neurofibromatosis. Winter et al. reported an average progression of 27 degrees during brace treatment in dystrophic patients, with zero cases of improvement.
Dystrophic Scoliosis Without Kyphosis
Patients presenting with dystrophic scoliosis lacking a kyphotic component should be observed at 6-month intervals if the curve is under 20 degrees. The moment progression is documented, posterior spinal fusion must be executed.
If posterior fusion is performed early, an anterior approach may be avoided. However, for neglected curves exceeding 80 degrees, Betz et al. strongly recommend a combined anterior and posterior arthrodesis. Primary anterior and posterior fusion is the standard for dystrophic scoliosis >40 degrees unless specific contraindications exist (e.g., massive anterior neurofibromas, excessive venous plexuses, severe osteopenia, or thrombocytopenia secondary to splenic fibromas).

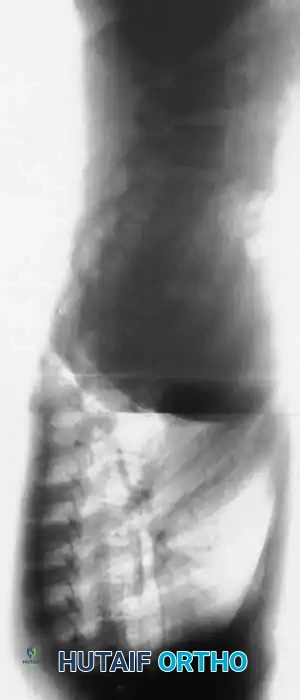


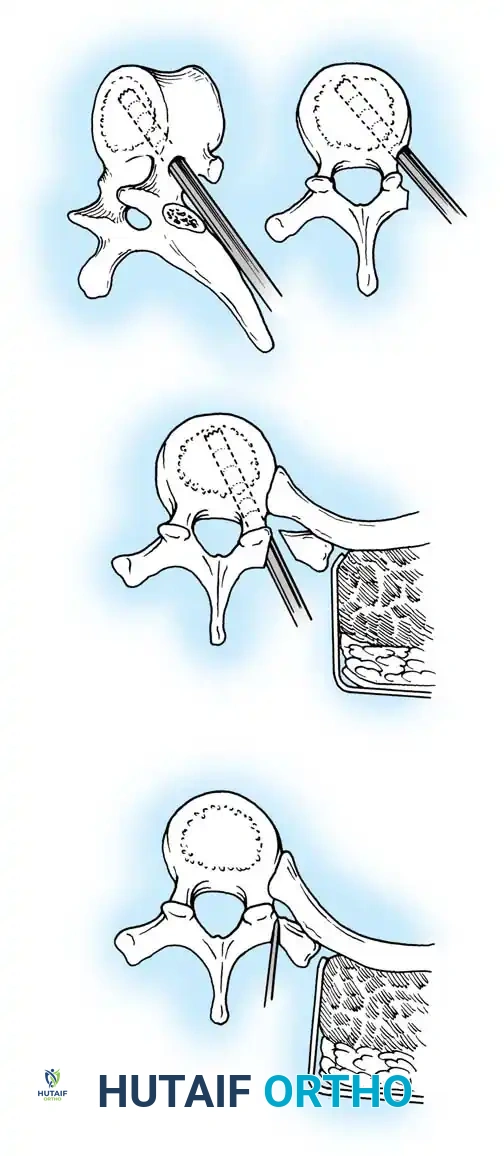
Fig. 38-201: Surgical diagrams illustrating pedicle preparation and instrumentation strategies in dystrophic vertebrae.
Segmental pedicle screw systems provide superior biomechanical purchase in dysplastic bone, permitting early ambulation. However, the fusion mass in NF-1 is notoriously unreliable. If the instrumentation purchase is tenuous, postoperative bracing is mandatory. Furthermore, the fusion mass must be scrutinized at 1 year postoperatively; if progression exceeds 10 degrees or pseudarthrosis is suspected, the mass must be re-explored and augmented with robust autogenous iliac crest bone grafting.
Dystrophic Kyphoscoliosis
Dystrophic scoliosis coupled with angular kyphosis represents one of the most formidable challenges in spine surgery. Patients with this pathology respond exceptionally poorly to posterior fusion alone. Consistent, long-term success is achieved almost exclusively through combined anterior and posterior (360-degree) fusions.



Winter and Hsu emphasized that the primary reasons for failure in these curves are inadequate bone graft volume and insufficient fusion area. The surgical strategy must include:
1. Anterior Release and Corpectomy: The entire structural area of the deformity must be addressed anteriorly. This requires complete, aggressive disc excision back to the posterior longitudinal ligament.
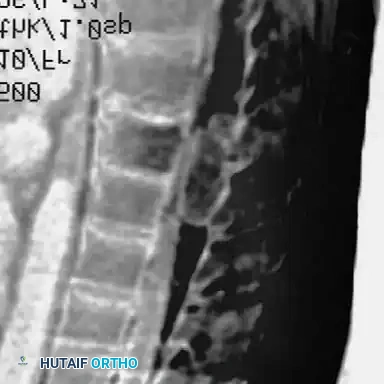
2. Structural Strut Grafting: Strong strut grafts are biomechanically imperative to support the anterior column and prevent kyphotic collapse. Fibular allografts or autografts, supplemented with rib and iliac crest cancellous bone, are standard.
3. Vascularized Rib Grafts: For severe, rigid kyphoscoliotic deformities, vascularized rib graft augmentation (as described by Bradford) provides superior biological healing potential in the hostile, dysplastic environment of the NF-1 spine.
4. Posterior Instrumentation: Following the anterior stage, robust posterior segmental instrumentation and arthrodesis are performed.


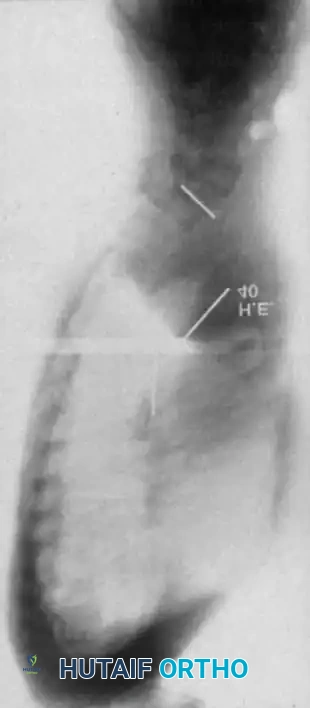
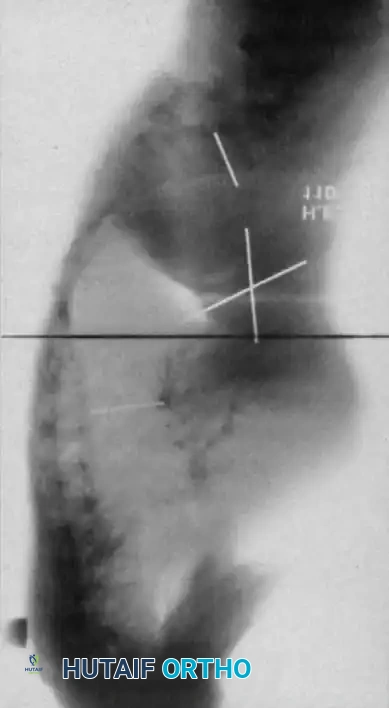
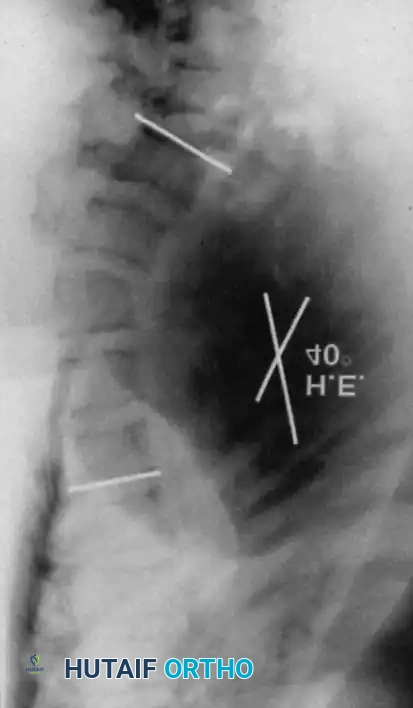
Fig. 38-202: Postoperative radiographs demonstrating anterior fusion with vascularized rib graft and structural strut grafting in a patient with severe dystrophic kyphoscoliosis.
For smaller dystrophic kyphoscoliosis (kyphosis <40 degrees), posterior instrumentation and arthrodesis may be attempted early, but the fusion mass must be explored at 6 to 12 months. If kyphosis exceeds 50 degrees, the combined anterior/posterior approach is non-negotiable. The anterior fusion must extend one or two levels beyond the end vertebrae of the kyphotic segment to prevent junctional failure.


MANAGEMENT OF SPINAL CORD COMPRESSION
Neurological deficits in NF-1 patients can arise from two distinct etiologies: direct compression from an intraspinal tumor (e.g., neurofibroma) or mechanical compression from severe angular kyphosis.
CRITICAL PITFALL: If spinal cord compression is caused by a kyphoscol
Associated Surgical & Radiographic Imaging



You Might Also Like