Scapulothoracic Dissociation: Epidemiology, Anatomy & Clinical Implications
Key Takeaway
Scapulothoracic dissociation (STD) is a rare, devastating high-energy orthopedic trauma where the scapula separates from its chest wall attachments. This injury causes extensive muscular, brachial plexus, and major vascular damage, often termed a 'subcutaneous forequarter amputation.' It carries severe morbidity and high mortality, despite an intact skin envelope masking its profound internal severity.
Introduction & Epidemiology
Scapulothoracic dissociation (STD) represents a rare, yet devastating, closed traumatic disruption of the scapula from its muscular and neurovascular attachments to the posterior chest wall. Often described as a "subcutaneous forequarter amputation," this injury signifies the profound forces involved and the extensive underlying soft tissue and neurovascular damage, even in the absence of overt skin violation. The primary distinguishing feature from a true forequarter amputation is the intact skin envelope, which paradoxically can mask the severity of the underlying trauma.
This high-energy injury typically results from violent traction and rotation forces, most commonly observed in motor vehicle accidents, particularly motorcycle collisions, and pedestrian versus vehicle impacts. The mechanism often involves a significant shearing force that leverages the upper extremity away from the torso, leading to the avulsion of critical muscular attachments (e.g., trapezius, rhomboids, levator scapulae, serratus anterior) and the stretching or tearing of the brachial plexus and subclavian or axillary vessels.
Epidemiologically, STD is exceedingly rare, with an incidence estimated to be less than 1% of all major blunt trauma cases. Despite its rarity, the associated morbidity and mortality are remarkably high. Mortality rates can range from 10% to 20%, primarily due to massive hemorrhage, associated thoracic injuries, or prolonged hypovolemic shock. For survivors, significant long-term disability, predominantly related to irreversible brachial plexopathy, is almost universal.
The initial presentation often includes massive swelling of the shoulder and periscapular region, a pulseless or compromised arm, and profound neurological deficit. Early recognition is paramount for limb salvage and reduction of systemic complications. Diagnosis is frequently confirmed by the characteristic lateral displacement of the scapula relative to the thoracic spine on a nonrotated chest radiograph, a subtle but critical indicator of the extent of muscular avulsion.

Surgical Anatomy & Biomechanics
A thorough understanding of the complex regional anatomy and the biomechanics of injury is crucial for effective management of STD. The scapulothoracic articulation is a musculofascial pseudo-joint, lacking true synovial connection but providing substantial mobility and stability to the shoulder girdle.
Bony Anatomy
The primary bony components involved are the scapula, clavicle, and the posterior thoracic cage (ribs and vertebral column). While STD describes the dissociation of the scapula, associated fractures of the clavicle, scapula, ribs, or proximal humerus are common. The integrity of the clavicle is particularly important as it serves as the only direct bony link between the upper extremity and the axial skeleton.
Muscular Attachments
The scapula is suspended by a robust network of muscles that are violently disrupted in STD:
*
Trapezius:
Originates from the nuchal line, ligamentum nuchae, and spinous processes of C7-T12, inserting onto the clavicle, acromion, and scapular spine. Provides superior and medial support.
*
Rhomboids (Major and Minor):
Originate from spinous processes of C7-T5, inserting onto the medial border of the scapula. Retract and rotate the scapula inferiorly.
*
Levator Scapulae:
Originates from transverse processes of C1-C4, inserting onto the superior angle of the scapula. Elevates and rotates the scapula.
*
Serratus Anterior:
Originates from the first eight or nine ribs, inserting along the entire medial border of the scapula. Crucial for protraction, rotation, and stability, preventing "winging."
*
Latissimus Dorsi, Teres Major, and Rotator Cuff muscles:
While not directly suspending the scapula from the thorax, their origins and insertions on the scapula and humerus are subject to severe traction.
Neurovascular Structures
The periscapular region is densely packed with critical neurovascular structures, making injury to these elements almost axiomatic in STD:
*
Brachial Plexus:
Formed by the ventral rami of C5-T1, the plexus passes through the scalene triangle, behind the clavicle, and over the first rib to innervate the entire upper extremity. Its close proximity to the scapula and axillary vessels makes it highly vulnerable to stretch, rupture, or avulsion. Complete brachial plexopathy is reported in 80% of cases, with partial plexopathy in 15%. This often involves avulsion from the spinal cord, indicating an extremely poor prognosis for recovery.
*
Subclavian and Axillary Arteries:
The subclavian artery transitions to the axillary artery at the lateral border of the first rib. These vessels supply the entire upper extremity and are tethered proximally to the aortic arch and distally by their branches. Violent traction forces can lead to intimal tears, lacerations, or complete transection, with vascular injury (subclavian or axillary artery) occurring in 88% of reported cases.
*
Subclavian and Axillary Veins:
Course anterior and inferior to their arterial counterparts. While less prone to complete transection due to their thinner walls and lower pressure, significant venous injury can lead to massive hemorrhage and venous outflow obstruction.
*
Long Thoracic Nerve:
Originates from C5-C7, running superficially on the serratus anterior muscle. Susceptible to stretch injury, leading to scapular winging.
*
Dorsal Scapular Nerve:
Originates from C5, innervates the rhomboids and levator scapulae. Injury affects scapular retraction and elevation.
*
Suprascapular Nerve:
Arises from the upper trunk of the brachial plexus, innervating the supraspinatus and infraspinatus muscles. Vulnerable to stretch or compression in severe scapular displacement.
Biomechanics of Injury
The mechanism of STD is characterized by the application of extreme forces that overwhelm the muscular and ligamentous stabilizers of the shoulder girdle. The "subcutaneous forequarter amputation" analogy highlights the fundamental disruption:
1.
Massive Traction/Shearing Force:
A violent force, often applied to the abducted and externally rotated upper extremity, pulls the limb away from the torso. This elongates and tears the muscles attaching the scapula to the thorax (e.g., serratus anterior, rhomboids, trapezius).
2.
Leverage Effect:
The scapula, humerus, and clavicle act as a lever arm. As the limb is pulled, the scapula is violently displaced laterally, often by several centimeters, on the posterior chest wall. This lateralization is the pathognomonic radiographic sign.
3.
Neurovascular Tension:
The stretch on the upper extremity translates directly to tension on the brachial plexus and the subclavian/axillary vessels. The relatively fixed points of the brachial plexus at the spinal cord and the subclavian artery at its origin from the aortic arch/brachiocephalic trunk make them highly susceptible to avulsion or transection when extreme distal tension is applied. The first rib and clavicle can act as fulcrums, further exacerbating the tension and compression.
4.
Associated Fractures:
The forces can also cause fractures of the clavicle (midshaft or medial), scapular body or neck, acromion, coracoid, glenoid, or even ribs, adding to the instability and complexity. However, it's critical to note that STD can occur without obvious osseous injury, with soft tissue and neurovascular damage predominating.
This complete disruption leads to a flail upper extremity, often with irreversible neurological damage and acute limb ischemia.
Indications & Contraindications
Management of scapulothoracic dissociation is complex, requiring a multidisciplinary approach focused on immediate life-saving interventions, limb salvage, and long-term functional recovery. Operative intervention is typically indicated, especially given the high incidence of vascular injury.
Indications for Operative Intervention
The primary indications for surgery in STD are driven by the need for hemorrhage control, limb revascularization, and stabilization of associated injuries.
- Vascular Injury with Limb Ischemia: This is the most pressing indication. Any evidence of arterial injury (pulseless extremity, expanding hematoma, thrill/bruit, objective signs of ischemia such as pallor, poikilothermia, paresthesia, pain, or paralysis) necessitates urgent surgical exploration and repair. Revascularization within 6-8 hours is critical for limb viability.
- Ongoing Hemorrhage/Hematoma: Significant and uncontrolled bleeding from vascular injury or extensive soft tissue damage warrants immediate surgical exploration for source control.
- Progressive Neurological Deficit (Acute Compression): While primary repair of a completely avulsed brachial plexus is not feasible acutely, an acute and worsening neurological deficit potentially due to an expanding hematoma or direct nerve compression may warrant early exploration for decompression, though this is less common than exploring for vascular injury.
- Associated Unstable Fractures: Displaced fractures of the clavicle, scapula, or ribs that compromise neurovascular structures, thoracic stability, or necessitate open reduction and internal fixation (ORIF) as part of the overall stabilization strategy.
- Open Injury: Though rare in STD, any open wound with communication to the dissociated area requires urgent surgical debridement and management of contamination.
- Need for Definitive Soft Tissue Debridement: Extensive muscle necrosis or contamination in delayed presentations, though aggressive debridement is balanced against further devitalization in an already compromised limb.
Contraindications to Acute Operative Intervention
Absolute contraindications are few and generally revolve around the patient's overall physiological status.
1.
Hemodynamic Instability:
In the polytrauma patient, life-threatening injuries to the brain, chest, or abdomen take precedence. Operative management of STD may be delayed until the patient is physiologically stable, though this can sometimes mean accepting limb loss if vascular injury is present.
2.
Non-salvageable Limb:
In situations where there is complete brachial plexus avulsion combined with irreversible ischemia (e.g., delayed presentation >12-24 hours with established rigor mortis or severe muscle necrosis), especially in a patient with multiple comorbidities, primary amputation might be considered the most appropriate course of action, avoiding futile revascularization attempts.
3.
Severe Concurrent Injuries:
A high Injury Severity Score (ISS) with multiple life-threatening injuries may dictate a damage control approach, with definitive management of STD deferred or secondary to stabilization of other critical systems.
Non-Operative Management
True scapulothoracic dissociation with significant neurovascular injury is rarely managed non-operatively.
1.
Subtle Scapular Displacement without Neurovascular Compromise:
In cases where the lateral scapular displacement is minimal (<1.0-1.5 cm) and there are no signs of vascular injury or significant neurological deficit, non-operative management with observation, pain control, and early mobilization may be considered. However, these cases might represent less severe periscapular injuries rather than true STD.
2.
Palliative Care:
In patients with unsalvageable limbs and severe comorbidities where surgical intervention is deemed futile or contraindicated due to patient wishes or medical futility.
Table: Operative vs. Non-Operative Indications in Scapulothoracic Dissociation
| Feature | Operative Indication | Non-Operative Consideration |
|---|---|---|
| Vascular Status | Acute limb ischemia (pulseless, pallor, paresthesia, etc.) | No vascular injury or signs of ischemia. |
| Expanding hematoma, uncontrolled hemorrhage. | Minor vascular spasm without persistent compromise (rare in STD). | |
| Neurological Status | Acute, rapidly worsening deficit due to compression. | Established complete brachial plexus avulsion (primary repair not possible). |
| Open nerve injury (rare). | Partial or stretch injury without acute compromise. | |
| Scapular Displacement | Significant lateral displacement (>1.5-2 cm on CXR). | Minimal lateral displacement (<1.0-1.5 cm). |
| Associated Fractures | Unstable, displaced clavicle/scapula/rib fractures. | Stable, non-displaced associated fractures. |
| Wound Status | Open injury with contamination. | Closed injury without contamination. |
| Patient Stability | Hemodynamically stable or stabilized. | Unstable polytrauma with more life-threatening injuries (temporary contraindication). |
| Limb Viability | Salvageable limb. | Non-salvageable limb (e.g., prolonged ischemia, established necrosis). |
Pre-Operative Planning & Patient Positioning
Successful management of STD hinges on meticulous pre-operative planning, rapid resuscitation, and appropriate patient positioning to facilitate comprehensive assessment and surgical access.
Pre-Operative Planning
-
Initial Assessment and Resuscitation:
Adherence to Advanced Trauma Life Support (ATLS) protocols is paramount.
- Airway, Breathing, Circulation (ABC): Secure airway, assess ventilation, and control hemorrhage. Hypotension is common due to significant blood loss into the large periscapular space and associated injuries.
- Neurovascular Assessment: Immediate and repeated evaluation of distal pulses (palpation, Doppler ultrasound) and neurological function (motor and sensory examination of the upper extremity). An ankle-brachial index (ABI) can be helpful but may be limited by proximal injury.
- Hemodynamic Stabilization: Aggressive fluid resuscitation, blood product transfusion (packed red blood cells, fresh frozen plasma, platelets, cryoprecipitate) to address hypovolemic shock and coagulopathy. Consider tranexamic acid.
-
Diagnostic Imaging:
-
Plain Radiographs:
- Chest X-ray (CXR): Crucial for initial diagnosis. Lateral displacement of the medial border of the scapula by >1-2 cm relative to the spinous process of T2-T7 on a non-rotated AP chest film is pathognomonic. Also assess for associated rib fractures, pneumothorax, hemothorax, and clavicle fractures.
- Shoulder Series: AP, Scapular Y, Axillary views to identify associated glenohumeral dislocation or proximal humerus/scapular fractures.
- Cervical Spine Films: To rule out associated cervical spine injury.
- Computed Tomography Angiography (CTA): The gold standard for evaluating suspected vascular injury and defining the extent of soft tissue and bony trauma. It precisely localizes arterial and venous injuries, identifies active extravasation, pseudoaneurysm formation, or intimal tears, and provides detailed information on associated fractures (clavicle, scapula, ribs, humerus) and their displacement.
- MRI: Less urgent in the acute setting but invaluable for comprehensive evaluation of the brachial plexus post-stabilization, delineating root avulsions from peripheral nerve lesions, and assessing muscle viability.
-
Plain Radiographs:
-
Consultations:
A multidisciplinary team approach is mandatory.
- Trauma Surgery: For overall patient management and coordination.
- Vascular Surgery: Essential for evaluation and repair of arterial and venous injuries.
- Orthopedic Surgery: For stabilization of associated fractures and overall limb management.
- Neurosurgery/Plastic Surgery (with Nerve Expertise): For brachial plexus evaluation and potential reconstruction (usually delayed).
- Anesthesiology: For perioperative management of a complex, often unstable patient.
-
Pre-operative Optimization:
- Blood Bank: Ensure immediate availability of adequate blood products.
- Coagulopathy Correction: Address any pre-existing or trauma-induced coagulopathy.
- Antibiotics: Prophylactic broad-spectrum antibiotics, especially if open injury or prolonged ischemia.
- Tetanus Prophylaxis: Administer as indicated.
Patient Positioning
Proper positioning is critical for optimal surgical access and exposure of the extensive injury zone.
1.
Supine Position:
This is the most common initial position, allowing immediate access to the entire anterior shoulder, supraclavicular, infraclavicular, and axillary regions.
* The affected arm should be prepped and draped free to allow for manipulation and assessment of distal perfusion.
* A roll can be placed under the ipsilateral shoulder to elevate it slightly, providing better access to the supraclavicular fossa and allowing the scapula to fall posteriorly.
* Allows for simultaneous access to potential donor sites for vascular grafts (e.g., saphenous vein from the leg) if needed.
* Consider positioning for potential chest entry if proximal subclavian or great vessel injury is suspected (e.g., left lateral thoracotomy position for left subclavian, median sternotomy for great vessels).
2.
Lateral Decubitus or Semi-Lateral Position:
May be considered if there is extensive posterior soft tissue damage requiring debridement or for fixation of specific posterior scapular fractures. However, this position limits access to the anterior neurovascular bundle and typically requires repositioning if a vascular repair is the primary goal. This is usually reserved for secondary procedures.
3.
Beach Chair Position:
Rarely used acutely for STD due to the need for extensive anterior exposure and management of potential hemodynamic instability. It may be used if the primary associated injury is a glenohumeral fracture or dislocation, but not for the dissociation itself.
Regardless of the position, ensuring secure access to the patient's airway, central venous access, arterial line, and urinary catheter is paramount. The surgical field must be prepped and draped to allow for extensive exposure of the shoulder, clavicle, axilla, and potentially the supraclavicular region, as well as the chest and neck if necessary.
Detailed Surgical Approach / Technique
The surgical management of scapulothoracic dissociation is dictated by the specific injuries identified, with a primary focus on hemorrhage control, vascular reconstruction, and management of associated skeletal injuries. Brachial plexus repair is typically a delayed procedure.
Goals of Surgery
- Life Salvage: Control of hemorrhage from major vessels or extensive soft tissue tearing.
- Limb Salvage: Revascularization of the ischemic extremity.
- Debridement: Removal of devitalized tissue and contaminants.
- Stabilization: Fixation of associated unstable fractures (e.g., clavicle, scapula, ribs).
- Neurological Assessment: Initial evaluation of brachial plexus injury, though definitive repair is usually delayed.
Surgical Approaches
Due to the widespread nature of the injury, a comprehensive exposure is often required. The most common primary approach is anterior, often combined with a supraclavicular extension.
-
Anterior (Deltopectoral) Approach with Supraclavicular Extension: This is the workhorse approach for proximal vascular and brachial plexus injuries.
- Incision: A long, curvilinear incision extending from the sternal notch, along the medial two-thirds of the clavicle, curving inferiorly in the deltopectoral groove, and then extending into the axilla. This allows for excellent exposure of the entire subclavian/axillary vessels and the brachial plexus.
-
Exposure of Clavicle and Pectoralis Major:
- Identify and ligate/preserve the cephalic vein in the deltopectoral groove.
- Retract the deltoid laterally and the pectoralis major medially. If needed for wider exposure of the infraclavicular space, a portion of the pectoralis major may be released from the clavicle, or a pectoralis minor tenotomy may be performed.
- The clavicle may be osteotomized or resected to gain superior access to the supraclavicular and retroclavicular spaces, though this is often not necessary if a medial clavicular fracture is already present. If a claviculectomy is performed, consideration must be given to potential future reconstruction.
-
Subclavian/Axillary Vessel Exposure:
- Carefully dissect through the clavipectoral fascia.
- Identify the axillary vein (inferior and anterior) and artery (superior and posterior to the vein).
- Trace these vessels proximally to the subclavian vessels and distally as needed.
- Crucial Step: Obtain proximal and distal vascular control with vessel loops before addressing any injury. This may require extending the incision medially into the neck for proximal subclavian control or even a sternotomy or anterior thoracotomy if the innominate or great vessels are involved, though this is rare.
-
Brachial Plexus Exposure:
- The brachial plexus lies superior and posterior to the axillary artery.
- Careful dissection through scar tissue and hematoma will expose the cords and divisions of the plexus.
- Identify the extent of injury: stretch, rupture, or avulsion.
- Acute repair of a complete avulsion from the spinal cord is not feasible. For other types of injuries, primary repair (if clean laceration) or tag placement for delayed reconstruction may be considered.
- Associated Clavicle Fracture Fixation: If a clavicle fracture is present and unstable, it should be addressed. Options include plate and screw fixation, which also aids in restoring some shoulder girdle stability.
-
Posterior Approach (Modified Judet or Extended Utility Incision): Less commonly a primary approach but may be necessary for:
- Extensive debridement of posterior musculature.
- Fixation of complex scapular fractures, especially glenoid fractures.
- Drainage of large posterior hematomas.
- Incision: A long curvilinear incision along the medial border of the scapula, potentially extending laterally along the scapular spine.
- Dissection: Elevate the trapezius and rhomboids off the scapula (or identify their avulsion points). Identify the serratus anterior and assess its integrity.
- Care must be taken to protect the dorsal scapular nerve and long thoracic nerve, which are often stretched or damaged.
Step-by-Step Surgical Technique
Phase 1: Emergency Life & Limb Salvage (Acute)
- Patient Positioning: Supine with the affected arm draped free. Access to lower extremity for potential saphenous vein graft.
- Incision: Long anterior approach as described above, centered on the clavicle and deltopectoral groove, extending to the axilla.
-
Hemorrhage Control:
- Rapidly identify the major vascular injury. This often involves dissecting through a large hematoma.
- Obtain proximal and distal control of the injured vessel (subclavian/axillary artery and vein) using vessel loops or vascular clamps.
- Ligate any actively bleeding smaller vessels.
-
Vascular Reconstruction:
- Debridement: Excise all devitalized or thrombosed vessel segments.
-
Options:
- Primary Repair: If a clean laceration with minimal tissue loss and no tension, direct end-to-end repair with fine non-absorbable sutures (e.g., 6-0 Prolene) may be possible.
- Interposition Graft: More commonly, significant tissue loss requires an interposition graft. The contralateral greater saphenous vein is the preferred conduit. Synthetic grafts (PTFE) may be used but have a higher risk of infection and thrombosis in contaminated fields. Ensure adequate length to bridge the gap without tension.
- Ligation: In dire circumstances, particularly for venous injuries, ligation may be necessary. For arterial injuries, ligation is a last resort, as it invariably leads to limb amputation.
- Completion Angiography: Intraoperative angiography or Doppler ultrasound should be performed to confirm patency and assess for any distal thrombi.
- Fasciotomy: Prophylactic fasciotomies of the forearm and hand compartments should be strongly considered after successful revascularization, especially if ischemia time was prolonged (>4-6 hours) or significant swelling is present. This mitigates compartment syndrome.
-
Brachial Plexus Exploration (Initial Assessment):
- Gently explore the brachial plexus to identify the level of injury (roots, trunks, cords).
- Identify complete avulsion versus stretch or rupture.
- Do not attempt primary repair of avulsions from the spinal cord. Mark the proximal and distal stumps of ruptured nerves with non-absorbable sutures (e.g., 4-0 Prolene) for delayed reconstruction.
- If a compressive hematoma is identified, decompress the plexus.
- Debridement: Copious irrigation and removal of all devitalized muscle and soft tissue, especially if the wound is contaminated.
Phase 2: Fracture Stabilization (Concurrently or Delayed)
- Clavicle Fixation: If the clavicle is fractured and significantly displaced, plate and screw fixation (e.g., locking plate) helps restore the integrity of the shoulder girdle. This provides a stable platform for muscle reattachment and protects the underlying neurovascular structures.
- Scapular Fracture Fixation: If there are significant, displaced scapular fractures (e.g., glenoid fracture, displaced scapular neck), these may be addressed via appropriate anterior or posterior approaches.
- Humerus/Glenoid: Associated injuries to the proximal humerus or glenoid are managed according to standard orthopedic trauma principles.
Phase 3: Closure
- Hemostasis: Ensure meticulous hemostasis.
- Drains: Placement of suction drains in the deep spaces (axilla, periscapular) is recommended to prevent hematoma formation.
- Layered Closure: Reapproximate muscles and fascia. Close subcutaneous tissue and skin layers without tension.
- Post-operative Dressing: Apply a bulky, sterile dressing. Immobilize the limb in a sling or shoulder immobilizer, depending on the extent of repair and associated fractures.

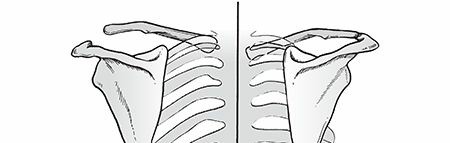
Illustration of severe soft tissue disruption and neurovascular injury characteristic of scapulothoracic dissociation.
Complications & Management
Scapulothoracic dissociation is associated with a high rate of severe complications, both early and late, reflecting the extensive damage to critical structures. Management strategies must be proactive and multidisciplinary.
Early Complications (Acute Phase)
-
Hemorrhage (Incidence: High, often immediate):
- Description: Life-threatening blood loss from major vascular injuries (subclavian/axillary artery/vein) or extensive muscle avulsions. Can lead to hypovolemic shock.
- Management: Immediate surgical exploration for vascular repair or ligation, aggressive fluid resuscitation, massive transfusion protocols, correction of coagulopathy.
-
Acute Limb Ischemia (Incidence: 88% with arterial injury):
- Description: Insufficient blood supply to the limb due to arterial transection, thrombosis, or spasm, leading to tissue necrosis.
- Management: Urgent revascularization (primary repair, interposition graft). Prophylactic fasciotomy often indicated after revascularization.
-
Compartment Syndrome (Incidence: Variable, up to 30% after revascularization):
- Description: Increased pressure within muscle compartments, impairing perfusion and leading to irreversible muscle and nerve damage.
- Management: Prophylactic fasciotomy, especially after prolonged ischemia (>6 hours) or if significant swelling is present; emergent fasciotomy for clinical signs of compartment syndrome (tense compartment, pain out of proportion, progressive motor/sensory deficit).
-
Infection (Incidence: Low for primary closed injury, higher if open or repeated surgery):
- Description: Localized or systemic infection (sepsis) from wound contamination, devitalized tissue, or compromised host immunity.
- Management: Aggressive surgical debridement of necrotic tissue, appropriate broad-spectrum antibiotics, wound VAC therapy if indicated.
-
Acute Respiratory Distress Syndrome (ARDS) / Multi-organ Failure (Incidence: Significant in polytrauma):
- Description: Systemic inflammatory response from massive trauma, shock, and reperfusion injury affecting pulmonary function and other organs.
- Management: Intensive care unit support, ventilatory management, supportive care for organ systems, early recognition and treatment of sepsis.
-
Death (Incidence: 10-20%):
- Description: Often due to uncontrolled hemorrhage, associated major chest/head trauma, or multi-organ failure.
- Management: Aggressive resuscitation, damage control surgery, focus on life-saving interventions.
Late Complications (Chronic Phase)
-
Persistent Neurological Deficit (Incidence: Near 100% with high-grade plexopathy):
- Description: Flail limb, anesthesia, chronic neuropathic pain, loss of motor and sensory function due to irreversible brachial plexus injury (most commonly avulsion).
-
Management:
- Delayed Reconstruction: Nerve transfers (e.g., intercostal to musculocutaneous, contralateral C7), free functional muscle transfers (e.g., gracilis), or tendon transfers may provide limited function for specific muscles (e.g., elbow flexion). Requires specialized nerve surgeon expertise and is typically performed 3-9 months post-injury.
- Amputation: For a painful, insensate, non-functional limb, especially with severe causalgia, secondary amputation may be considered to improve quality of life and facilitate prosthetic fitting.
- Orthotics and Assistive Devices: For support and function.
- Chronic Pain Management: Multimodal approach including pharmacotherapy, nerve blocks, spinal cord stimulators.
-
Chronic Pain (Incidence: High):
- Description: Neuropathic pain (causalgia), musculoskeletal pain from residual instability, or phantom limb pain.
- Management: Multidisciplinary pain clinic involvement, pharmacological interventions (neuromodulators, opioids judiciously), physical therapy, psychological support.
-
Limb Shortening/Deformity (Incidence: Variable with associated fractures):
- Description: Residual limb length discrepancy or angular deformity from malunion of associated fractures (e.g., clavicle).
- Management: Corrective osteotomies if functionally limiting, bracing.
-
Nonunion/Malunion of Associated Fractures (Incidence: Moderate):
- Description: Failure of bone healing or healing in an unacceptable position, particularly for clavicle and scapular fractures.
- Management: Revision ORIF with bone grafting for nonunion; corrective osteotomy for symptomatic malunion.
-
Psychological Distress (Incidence: High):
- Description: Depression, anxiety, PTSD, body image issues, and adjustment disorders related to severe trauma and life-altering disability.
- Management: Psychological counseling, support groups, psychiatric intervention.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage / Management Strategies |
|---|---|---|
| Early | ||
| Hemorrhage | High (immediate) | Urgent surgical exploration, vascular repair/ligation, massive transfusion, coagulopathy correction. |
| Acute Limb Ischemia | 88% with arterial injury | Urgent revascularization (primary repair, interposition graft), consider prophylactic fasciotomy. |
| Compartment Syndrome | Up to 30% after revascularization | Prophylactic or emergent fasciotomy. |
| Infection | Low (closed); Higher (open/repeated surgery) | Aggressive surgical debridement, targeted antibiotics, wound VAC therapy. |
| ARDS/Multi-organ Failure | Significant in polytrauma | ICU support, ventilatory management, supportive care, sepsis treatment. |
| Death | 10-20% | Aggressive resuscitation, damage control surgery. |
| Late | ||
| Persistent Neurological Deficit | Near 100% with high-grade plexopathy | Delayed nerve transfers, free functional muscle transfers, tendon transfers; orthotics; chronic pain management; secondary amputation for unsalvageable, painful limb. |
| Chronic Pain | High | Multidisciplinary pain clinic, pharmacotherapy (neuromodulators), nerve blocks, psychological support. |
| Limb Shortening/Deformity | Variable | Corrective osteotomies, bracing. |
| Nonunion/Malunion of Fractures | Moderate | Revision ORIF with bone grafting (nonunion); corrective osteotomy for symptomatic malunion. |
| Psychological Distress | High | Psychological counseling, support groups, psychiatric intervention. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following scapulothoracic dissociation is a protracted and challenging process, demanding a multidisciplinary team approach involving orthopedic surgeons, vascular surgeons, neurologists, physical therapists, occupational therapists, and pain management specialists. The protocol is highly individualized, depending on the extent of vascular repair, associated skeletal injuries, and the severity and type of brachial plexus injury.
Phase 1: Immediate Post-Operative / Protective Phase (Weeks 0-6)
Goals: Protect surgical repairs, control pain and edema, maintain joint integrity, prevent complications.
-
Immobilization:
- If vascular repair was performed, the arm is often kept in a sling or shoulder immobilizer in a neutral position to minimize tension on the repair. Avoid extreme abduction or rotation.
- If associated fractures were fixed, immobilization depends on fracture stability and surgeon preference (e.g., shoulder immobilizer for clavicle fixation, sling for scapular fixation).
- Continuous monitoring of distal neurovascular status is paramount.
- Pain Management: Aggressive, multimodal pain control using a combination of opioids, NSAIDs, acetaminophen, and neuropathic agents (gabapentin, pregabalin) if nerve injury is present.
- Edema Control: Elevation of the affected extremity, gentle compression dressings, manual lymphatic drainage.
-
Early Motion (Non-Involved Joints):
- Active range of motion (AROM) of the elbow, wrist, and hand on the affected side, as tolerated and without stressing the shoulder/vascular repair.
- Gentle AROM for the contralateral upper extremity and lower extremities to maintain overall conditioning.
- Wound Care: Meticulous wound care, drain management.
- Deep Vein Thrombosis (DVT) Prophylaxis: As per institutional protocols.
- Patient Education: Instruct on signs of complications (e.g., infection, worsening ischemia, compartment syndrome).
Phase 2: Early Mobilization / Strengthening Phase (Weeks 6-12)
Goals: Gradual increase in range of motion, initiate gentle strengthening, address early neuropathic pain, scar management.
-
Progressive Range of Motion (ROM):
- Passive Range of Motion (PROM): Gentle, pain-free PROM of the shoulder (flexion, abduction, rotation) initiated by a therapist, gradually progressing. Avoid end-range motions that may stress repairs.
- Active-Assisted Range of Motion (AAROM): Progress to AAROM as pain allows and stability of repairs is confirmed.
- Active Range of Motion (AROM): Gradually introduce AROM within a protected range.
-
Gentle Strengthening:
- Isometrics: Initiate gentle isometric exercises for shoulder girdle musculature, if there is evidence of muscle innervation.
- Scapular Stabilization: Focus on exercises to activate the remaining scapular stabilizers (e.g., rhomboids, serratus anterior if partially functioning).
- Scar Management: Desensitization, massage, silicone sheeting to prevent hypertrophic scarring, especially over nerve repair sites.
-
Neurological Assessment & Rehabilitation:
- Ongoing neurological examination to monitor for any signs of recovery (Tinel's sign, muscle reinnervation).
- Sensory re-education for areas with partial sensory return.
- Electrical stimulation may be considered for denervated muscles to prevent atrophy and promote reinnervation (controversial, but often used).
- Referral for nerve reconstruction if delayed intervention is planned (typically 3-9 months post-injury).
Phase 3: Advanced Strengthening & Functional Integration Phase (Months 3-6+)
Goals: Maximize strength, endurance, and functional use of the limb; address long-term neurological deficits.
-
Progressive Strengthening:
- Concentric and eccentric resistance exercises for all available muscle groups of the shoulder, elbow, wrist, and hand.
- Focus on functional movement patterns.
- Gradual progression with resistance bands, light weights, and bodyweight exercises.
- Targeted exercises for core stability and trunk strength, as they contribute to overall upper extremity function.
-
Neuromuscular Re-education:
- Proprioceptive training and balance exercises specific to the upper extremity.
- Coordination drills.
-
Functional Activities:
- Integration of the affected limb into activities of daily living (ADLs), work-related tasks, and leisure activities.
- Occupational therapy plays a critical role in adaptive strategies and assistive device recommendations.
-
Brachial Plexus Reconstruction Outcomes:
- If nerve reconstruction was performed, rehabilitation focuses on training the reinnervated muscles. This is a long process, often taking 12-24 months for distal reinnervation.
- Management of compensatory movements.
- Vocational Rehabilitation: Assessment of work capacity, job modifications, or retraining as necessary.
- Long-Term Monitoring: Regular follow-up with orthopedic, neurology, and rehabilitation teams to address any emerging issues, chronic pain, or functional decline.
Long-Term Considerations & Support
- Orthoses and Assistive Devices: Custom splints, braces, or slings may be required for chronic weakness, instability, or to prevent contractures.
- Psychological Support: Given the profound impact on quality of life, access to psychological counseling and support groups is vital for coping with chronic pain, disability, and potential amputation.
- Amputation Considerations: For limbs that remain insensate, painful, and non-functional despite maximal reconstruction efforts, secondary amputation may be considered to improve quality of life, pain management, and enable prosthetic fitting. This is a complex decision requiring extensive patient counseling.
Rehabilitation for STD is measured in years, not months, and aims to optimize function and minimize disability in the context of often irreversible neurological deficits.
Summary of Key Literature / Guidelines
Scapulothoracic dissociation is a rare and severe injury, which means there are no large-scale randomized controlled trials or universally adopted, explicit guidelines akin to those for more common orthopedic conditions. The existing literature primarily consists of case reports, small case series, and expert opinion. Nevertheless, a consensus on critical management principles has emerged from the fields of trauma, vascular, and orthopedic surgery.
Key Principles from the Literature:
-
High Index of Suspicion and Early Diagnosis:
- The literature consistently emphasizes the importance of recognizing STD in the context of high-energy trauma, even in the absence of obvious bony fracture.
- The pathognomonic sign of lateral scapular displacement on chest radiograph (>1.0-2.0 cm from the spinous processes) is highlighted as a critical diagnostic clue (Zuckerman et al., 1986; Oreck et al., 1984).
- Takeaway: Any significant soft tissue swelling around the shoulder following high-energy trauma should prompt thorough neurovascular assessment and evaluation for scapular displacement.
-
Urgent Vascular Assessment and Management:
- Multiple studies (e.g., Ebraheim et al., 1990; Rubenstein et al., 1995) underscore that the most immediate life-threatening and limb-threatening complication is vascular injury.
- CTA is the gold standard for diagnosing vascular injury, its location, and extent.
- Limb salvage is paramount: Prompt surgical exploration and revascularization within the critical ischemic window (generally 6-8 hours) significantly impacts limb viability and subsequent function. Primary repair or interposition grafting (saphenous vein preferred) are the mainstay.
- Fasciotomy: Prophylactic fasciotomies of the forearm and hand are frequently recommended post-revascularization, especially after prolonged ischemia, to prevent compartment syndrome.
- Takeaway: Vascular injury detection and immediate surgical intervention is the highest priority after initial resuscitation.
-
Brachial Plexus Injury (BPI) – A Devastating Prognostic Factor:
- The prevalence of BPI in STD is exceptionally high, with complete plexopathy reported in 80% and partial in 15% (Oreck et al., 1984; Rubenstein et al., 1995).
- Prognosis: Most literature confirms that complete brachial plexus avulsion from the spinal cord (preganglionic injury) carries a dismal prognosis for functional recovery of the limb.
- Management: Acute repair of avulsed roots is not feasible. The consensus is for delayed exploration and reconstruction (typically 3-9 months post-injury) by a specialized nerve surgeon. Early exploration is usually reserved for acute compression by hematoma or open injuries.
- Reconstruction options (nerve transfers, free muscle transfers) offer limited, but sometimes meaningful, functional recovery (e.g., elbow flexion) and pain management.
- Takeaway: Brachial plexus injury defines the long-term functional outcome and often dictates eventual limb disposition.
-
Associated Injuries and Multidisciplinary Care:
- STD is rarely an isolated injury. Associated fractures (clavicle, scapula, ribs, humerus) and other polytrauma injuries (head, chest, abdomen) are common.
- Clavicle fracture is a frequent associated injury, and its fixation can contribute to shoulder girdle stability.
- Multidisciplinary team approach: The necessity of collaboration among trauma surgeons, vascular surgeons, orthopedic surgeons, neurosurgeons, and rehabilitation specialists is universally emphasized (e.g., Zupancic et al., 2011).
- Takeaway: Comprehensive trauma assessment and coordinated care are essential for managing the complex array of injuries.
-
Mortality and Morbidity:
- Mortality rates range from 10% to 20%, mainly due to associated injuries and hemorrhage (Oreck et al., 1984; Zupancic et al., 2011).
- For survivors, significant long-term disability, primarily due to the flail, often insensate limb from brachial plexopathy, is expected. Chronic pain is also a major issue.
- Amputation: Primary or secondary amputation may be considered for a painful, insensate, non-functional limb to improve quality of life and facilitate prosthetic use. This decision is made after thorough discussion with the patient and family, often after attempts at nerve reconstruction have failed or been deemed futile.
- Takeaway: The prognosis for STD, even with optimal management, is guarded, with high rates of mortality and profound long-term disability.
In summary, while specific step-by-step surgical guidelines for STD are not formally published, the principles outlined above represent the current standard of care derived from accumulated experience and the consistent findings in the available academic literature. The focus remains on rapid assessment, immediate life and limb-saving interventions, meticulous surgical technique, and a long-term, multidisciplinary rehabilitation strategy aimed at optimizing the patient's functional capacity and quality of life within the constraints of severe injury.
You Might Also Like