C3-C7 Cervical Spine Injuries: Epidemiology, Anatomy, & Biomechanics
Key Takeaway
C3-C7 cervical spine injuries are traumatic events primarily from high-energy MVAs and falls, carrying significant neurological risks. Diagnosis involves understanding their epidemiology, complex surgical anatomy, and biomechanics. Key tools include Denis's three-column model and White & Panjabi criteria for assessing spinal instability and guiding management.
C3-C7 Cervical Spine Injuries: Recognize, Diagnose, Treat
Introduction & Epidemiology
Traumatic injuries to the C3-C7 cervical spine represent a significant proportion of all spinal trauma, often resulting in devastating neurological sequelae including quadriplegia or death. Understanding the unique anatomy, biomechanics, and injury patterns of this region is paramount for optimal patient management. The incidence of cervical spine trauma varies geographically but is consistently high in populations exposed to high-energy mechanisms.
Epidemiological data indicate that motor vehicle accidents (MVAs) are the leading cause, accounting for approximately 45-50% of injuries. Falls from height or ground-level falls, particularly in the elderly, contribute 20-25%. Diving accidents, often involving axial loading with a flexed neck, comprise 5-10%, while blunt trauma, including sports-related injuries and assaults, makes up the remainder. A bimodal distribution is often observed, with a peak in young adult males (due to high-energy trauma) and another in older adults (due to falls and underlying degenerative changes).
Early recognition and diagnosis are critical. Patients presenting with cervical spine trauma often have associated injuries, including head trauma, thoracic and lumbar spine injuries, and solid organ damage. A thorough initial assessment, including primary and secondary surveys, adherence to ATLS protocols, and immediate cervical spine immobilization, is essential to prevent secondary neurological injury.
Surgical Anatomy & Biomechanics
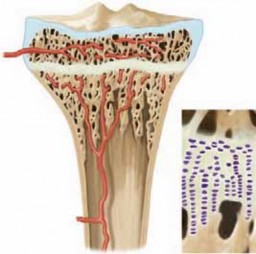
The C3-C7 cervical spine is a highly mobile segment, designed for a broad range of motion while protecting the spinal cord and nerve roots. This mobility is conferred by the intricate interplay of osseous structures, intervertebral discs, facet joints, and an extensive ligamentous network.
The vertebral bodies from C3 to C7 are kidney-shaped, increasing in size caudally. They possess a superior cortical surface that is concave in the coronal plane and convex in the sagittal plane. This morphology facilitates flexion, extension, and lateral tilt through the gliding motion of the superior articular facets on the inferior articular facets of the supra-adjacent vertebra. This anatomical configuration contributes to the inherent stability of the motion segments.
A distinctive feature of the C3-C7 vertebral bodies is the uncinate process , which projects superiorly from the lateral aspect of the vertebral body. These paired processes articulate with the inferior surface of the vertebral body above, forming the uncovertebral joints (also known as the joints of Luschka). These pseudoarthroses guide cervical motion, limit lateral translation, and protect the nerve roots from direct posterior migration of disc material. With degenerative changes, these uncovertebral joints can hypertrophy, forming osteophytes that may impinge on the nerve roots or vertebral artery.
The facet joints are true synovial joints, formed by the superior articular processes of the vertebra below and the inferior articular processes of the vertebra above. Their orientation changes throughout the cervical spine, becoming more coronally oriented from C3 to C7. In the lower cervical spine (C3-C7), they are oriented approximately 45 degrees to the transverse plane and 0-10 degrees to the sagittal plane, allowing for significant sagittal plane motion (flexion/extension) and lateral bending, while limiting axial rotation. The strong fibrous capsules of the facet joints contribute significantly to posterolateral stability. Disruption of these capsules and the associated ligamentum flavum, interspinous, and supraspinous ligaments can lead to significant instability.
The ligamentous structures of the cervical spine provide crucial passive stability. The anterior longitudinal ligament (ALL) resists extension, while the posterior longitudinal ligament (PLL) resists flexion. The ligamentum flavum, interspinous, and supraspinous ligaments, along with the nuchal ligament, offer posterior tensile strength. The capsular ligaments of the facet joints are critical for resisting shear forces and distraction. Injury to these structures, particularly multi-ligamentous disruption, often results in clinical instability.
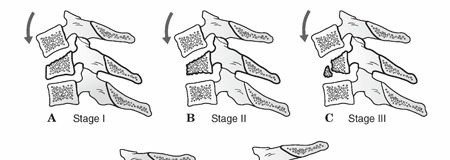
Biomechanics of the C3-C7 region are defined by the range of motion and load-bearing capacity. Each segment contributes to overall cervical motion. Normal cervical motion at each level has been extensively described using kinematic studies. This knowledge is important in assessing spinal stability. Pathological instability is defined by excessive motion, often exceeding physiological limits under normal physiological loads. The concept of the three-column model (Denis) is highly relevant: the anterior column (anterior longitudinal ligament, anterior two-thirds of the vertebral body and annulus), middle column (posterior one-third of the vertebral body and annulus, posterior longitudinal ligament), and posterior column (pedicles, laminae, spinous processes, facet joints, and associated ligaments). Involvement of two or more columns often signifies instability.
White and Panjabi criteria
provide quantitative radiographic parameters for diagnosing instability:
* Anterior displacement of one vertebra on another >3.5 mm.
* Angulation >11 degrees between adjacent vertebrae.
* Cervical kyphosis >20 degrees.
* Facet subluxation >50% overlap.
* Increased interspinous distance.
* A
"stretch" test
(Panjabi and White) may be performed with longitudinal cervical traction in a willing, conscious, and cooperative patient without neurological compromise. An abnormal test is indicated by a >1.7-mm interspace separation or a >7.5-degree change in angulation between vertebrae, though the clinical utility and safety of this test are debated and it is rarely performed in acute trauma.
The spinal cord occupies a significant portion of the canal at this level. The nerve roots exit above their corresponding pedicle (e.g., C5 nerve root exits above the C5 pedicle). The vertebral arteries ascend through the transverse foramina from C6 to C1, making them vulnerable to injury in fractures involving the transverse processes or facet dislocations.
Indications & Contraindications
Radiographic Evaluation
Initial radiographic evaluation consists of AP, lateral, and odontoid views of the cervical spine. A true lateral view that visualizes all seven cervical vertebrae and the C7-T1 junction is essential; if not obtained, a swimmer's view or CT scan is mandatory.

This image likely depicts a lateral cervical spine radiograph, essential for initial assessment of alignment, disc space height, and bony integrity.
If cervical spine instability is suspected and not definitively ruled out by static imaging, flexion/extension views may be obtained in a willing, conscious, and cooperative patient without neurological compromise. These views are performed under fluoroscopic guidance with extreme caution, halting if pain or neurological symptoms develop.
CT scans with reconstructions
are routinely obtained to characterize fracture patterns and the degree of canal compromise more clearly. This is particularly valuable for complex fractures, facet injuries, and assessing vertebral artery foraminal integrity.

This image likely represents a CT reconstruction, providing detailed bony anatomy and fracture characterization.
MRI
may be undertaken to delineate spinal cord, disc, and canal abnormalities further, especially in the presence of neurological deficits, normal radiographs ("SCIWORA" in children, or spinal cord injury without radiographic abnormality), or to assess ligamentous injury and intervertebral disc herniation potentially contributing to canal compromise.

This image likely shows an MRI sequence, vital for soft tissue evaluation, spinal cord integrity, and ligamentous assessment.
Decision-Making for Operative vs. Non-Operative Management
The decision to proceed with operative or non-operative management for C3-C7 cervical spine injuries is complex and multifactorial, considering neurological status, spinal stability, patient comorbidities, and fracture morphology. The Subaxial Cervical Spine Injury Classification (SLIC) system is widely used to guide treatment by assigning scores based on morphology, disc/ligamentous complex integrity, and neurological status.
TABLE: Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Neurological Status | - Progressive neurological deficit | - Neurologically intact |
| - Acute neurological deficit with significant spinal cord compression (e.g., incomplete SCI, ASIA C or D) | - Stable complete SCI (ASIA A or B) where stability is paramount and no further decompression is expected to improve function | |
| - Irreducible neurological deficit due to mechanical impingement | ||
| Spinal Stability | - Mechanical instability (e.g., White & Panjabi criteria met, >3.5mm translation, >11° angulation) | - Stable fractures without ligamentous injury (e.g., isolated spinous process fractures, stable compression fractures <25% loss of height, lamina fractures) |
| - Bilateral facet dislocations | - Unilateral facet dislocations that are successfully reduced and remain stable | |
| - Burst fractures with significant canal compromise (>25-30% on CT) | - Stable unilateral facet fractures without significant displacement or instability | |
| - Ligamentous injury with instability (e.g., complete disruption of ALL, PLL, or posterior ligamentous complex on MRI) | - Sprains without demonstrable instability on dynamic imaging | |
| - Irreducible dislocations or fracture-dislocations | ||
| Fracture Morphology | - Unstable fracture patterns (e.g., tear drop fractures, highly comminuted fractures, severe distraction injuries) | - Minimally displaced or non-displaced fractures without neurological compromise or instability |
| - Fractures with vertebral artery injury leading to neurological symptoms (rarely direct indication, but considered) | ||
| Patient Factors | - High functional demands in a cooperative patient | - Significant medical comorbidities precluding surgery |
| - Persistent mechanical pain despite adequate bracing/conservative care | - Non-ambulatory patients with limited life expectancy |
Contraindications for Surgery:
*
Absolute:
Medically unstable patient (e.g., severe coagulopathy, septic shock, uncontrolled systemic infection) where surgical intervention poses a greater immediate risk than the untreated spinal injury.
*
Relative:
Severe underlying comorbidities that significantly increase anesthetic or surgical risk (e.g., severe cardiopulmonary disease, end-stage renal disease, poor nutritional status), severe osteoporosis precluding adequate hardware fixation, active infection at the surgical site. In such cases, optimization of medical status is paramount, and alternative, less invasive stabilization methods or prolonged external immobilization may be considered if feasible.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for successful outcomes and to mitigate potential complications.
Pre-Operative Planning
-
Comprehensive Patient Assessment:
- Neurological Evaluation: Detailed motor, sensory, reflex, and sphincter examination, documented using the ASIA Impairment Scale. Frequent re-evaluation is crucial for detecting progressive deficits.
- Medical Optimization: Assessment and optimization of cardiac, pulmonary, renal, and nutritional status. Coagulation profiles, electrolyte balance, and blood transfusions should be addressed.
- Psychosocial Factors: Evaluation of patient's understanding, expectations, and social support.
-
Detailed Imaging Review:
- Review all radiographic studies (plain films, CT with multiplanar reconstructions, MRI) to fully understand the injury pattern, stability, canal compromise, and any pre-existing degenerative changes.
- Assess for vertebral artery injury, especially in cases of lateral mass fractures, facet dislocations, or severe rotational injuries, using CTA or MRA if indicated.
- Careful measurement of sagittal balance, kyphosis, and lordosis, particularly for multi-level fusions.
-
Surgical Strategy Development:
- Determine the optimal approach (anterior, posterior, or combined) based on the injury characteristics (e.g., anterior column compression/retropulsion mandates anterior decompression; posterior column tension band failure mandates posterior stabilization).
- Identify levels for decompression and fusion.
- Select appropriate instrumentation (plates, screws, rods, cages, grafts) and ensure availability. Plan for potential need for autograft harvest (e.g., iliac crest).
- Anticipate potential challenges (e.g., difficult reduction, significant blood loss, anatomical anomalies).
- Anesthesia Consultation: Discuss the anesthetic plan, anticipated blood loss, neuromonitoring (SSEP, MEP, EMG), and airway management (e.g., awake fiberoptic intubation for unstable necks).
Patient Positioning
Appropriate patient positioning is critical for surgical access, maintenance of spinal alignment, and prevention of iatrogenic injury. Neuromonitoring (SSEP/MEP) leads are placed and baseline readings obtained prior to positioning maneuvers.
-
For Anterior Cervical Approaches:
- Supine Position: The patient is positioned supine on the operating table.
- Head Support: A firm headrest or doughnut is used to stabilize the head. Slight neck extension is often desired to facilitate exposure, but excessive extension should be avoided, especially in cases of acute spinal cord injury, to prevent further neural compromise.
- Shoulder Roll: A small roll placed transversely between the scapulae can assist with gentle neck extension and allow the shoulders to drop posteriorly, aiding visualization of the lower cervical spine and C7-T1 junction.
- Traction (Optional): Gardner-Wells tongs or a halo ring may be in place pre-operatively to maintain reduction or provide gentle distraction during surgery. Traction weight should be carefully monitored.
- Arms: Tucked to the sides or extended on arm boards.
- Fluoroscopy: Ensure unobstructed access for lateral fluoroscopy.
-
For Posterior Cervical Approaches:
- Prone Position: The patient is carefully turned prone using log-roll technique, ensuring spinal alignment is maintained with adequate personnel.
- Spinal Frame: A specialized spinal frame (e.g., Jackson table, Wilson frame) or bolsters are used to support the chest and pelvis, allowing the abdomen to hang free. This reduces epidural venous pressure and minimizes blood loss.
- Head Positioning: The head is secured in a Mayfield clamp or similar skull fixation device. This allows for precise control of cervical flexion/extension and rotation, crucial for exposure and reduction. The head should be neutral or slightly flexed, maintaining a lordotic curve where possible. Care must be taken to avoid excessive flexion, which can stretch the spinal cord or restrict venous outflow.
- Eyes and Face: Meticulous care to protect eyes and face from pressure. Regular checks of pupillary dilation and conjunctival swelling.
- Arms: Padded and positioned on arm boards, often in a "superman" position or abducted, ensuring no compression of brachial plexus or ulnar nerves.
- Knees: Flexed with pillows to prevent peroneal nerve compression.
- Fluoroscopy: Ensure unobstructed access for lateral fluoroscopy.
Detailed Surgical Approach / Technique
Surgical intervention for C3-C7 cervical spine injuries typically involves decompression of neural elements and stabilization through fusion. The choice between an anterior, posterior, or combined approach is dictated by the injury morphology, location of compression, and the need for immediate and long-term stability.
Anterior Cervical Approaches (ACDF / ACCF)
The anterior approach is generally favored for anterior column compression (e.g., burst fractures with retropulsed fragments), disc herniation causing cord compression, and in many cases of kyphotic deformity or single-level instability.
-
Incision and Dissection:
- A transverse skin incision within a skin crease (C4-C6) or a longitudinal incision along the medial border of the sternocleidomastoid (SCM) for multi-level pathology.
- Subplatysmal dissection.
- Identify and retract the SCM laterally. The carotid sheath (containing carotid artery, internal jugular vein, vagus nerve) is identified and retracted laterally.
- Identify the trachea and esophagus, retracting them medially.
- The prevertebral fascia is incised longitudinally. The longus colli muscles are identified and carefully elevated subperiosteally to expose the anterior vertebral bodies and discs.
-
The recurrent laryngeal nerve is typically on the left, making a right-sided approach safer for many surgeons.

This image may represent a critical anatomical landmark or a step in the anterior cervical dissection, such as retraction of the sternocleidomastoid or carotid sheath.
-
Level Identification:
- Confirmation of the correct spinal level is paramount using fluoroscopy. A needle can be inserted into the disc space for localization.
-
Decompression (Discectomy/Corpectomy):
- For ACDF (Anterior Cervical Discectomy and Fusion) : The anterior annulus is incised, and the intervertebral disc material is removed using curettes and rongeurs. Cartilaginous endplates are removed to expose bleeding bone. Posterior osteophytes are removed, and the posterior longitudinal ligament (PLL) is carefully inspected and typically excised to ensure complete neural decompression.
-
For
ACCF (Anterior Cervical Corpectomy and Fusion)
: If a vertebral body is severely fractured or causes significant canal compromise, a corpectomy is performed. The disc spaces above and below the fractured body are removed first. Then, using high-speed burrs and osteotomes, the vertebral body is carefully resected, exposing the dura. Pulsation of the dura indicates adequate decompression. Lateral decompression should also address uncinate process hypertrophy.

This image might illustrate the decompression phase, showing the removal of disc material or a vertebral body, perhaps with instrumentation for stabilization already prepared.
-
Reduction:
- In cases of dislocation or significant angulation, reduction is performed carefully using cervical traction or distractor devices placed in the adjacent vertebral bodies. Intraoperative fluoroscopy confirms alignment.
-
Graft Placement and Fixation:
- After decompression and reduction, a structural graft (autograft from iliac crest, allograft, or PEEK/titanium cage) is inserted into the prepared defect. The size and contour of the graft are crucial to restore disc height, lordosis, and provide stability.
-
An anterior cervical plate is then applied to the anterior aspect of the vertebral bodies, spanning the fused segments. Screws are placed bicortically or unicortically into the vertebral bodies to secure the plate and graft. The plate acts as a tension band, providing immediate stability and promoting fusion.




These images likely depict various stages of anterior plating and graft insertion, showing different views of the hardware in place, possibly fluoroscopic or direct intraoperative views.
-
Closure:
- Hemostasis is achieved. A drain may be placed. Longus colli muscles are allowed to fall back into place. Platysma is reapproximated, and skin is closed.
Posterior Cervical Approaches (PCF / Laminectomy / Laminoplasty)
The posterior approach is indicated for posterior tension band injuries (e.g., bilateral facet dislocations, spinous process fractures), irreducible posterior elements, posterior compression (e.g., posterior osteophytes, ossification of PLL, epidural hematoma), or global instability requiring multi-column stabilization.
-
Incision and Dissection:
- A midline longitudinal incision from the nuchal ligament down to the relevant spinous processes.
- Deepen the incision through the subcutaneous tissue to the nuchal ligament.
-
Subperiosteal dissection of the paraspinal muscles (trapezius, rhomboids, splenius capitis, semispinalis cervicis) from the spinous processes and laminae using electrocautery and Cobb elevators. Careful attention is paid to maintaining a bloodless field and preserving the muscle attachments where possible for later re-approximation.

This image likely depicts the posterior surgical field after subperiosteal dissection, exposing the laminae and facet joints.
-
Level Identification:
- Fluoroscopy with a needle placed on a spinous process is used for accurate level identification.
-
Decompression (Laminectomy/Laminoplasty):
- Laminectomy: Complete removal of the lamina and spinous process at the affected level(s) to decompress the spinal cord. This is typically performed for focal posterior compression (e.g., epidural hematoma, tumor).
- Laminoplasty: A motion-preserving decompression technique, often chosen for multi-level cervical myelopathy without instability. The laminae are cut on one side (hinge) and partially on the other (opening), allowing the laminae to be "opened" like a door, increasing canal diameter. The opened laminae are then secured with small plates.
-
Reduction (for Dislocations):
- For facet dislocations, reduction can be performed with cranial traction and manual manipulation, often with the patient awake for neurological monitoring or under deep sedation with neuromonitoring. Open reduction involves careful disarticulation and realignment of the facets, sometimes requiring partial facetectomy.
-
Instrumentation and Fusion:
- Lateral Mass Screws: Most commonly used for C3-C6 fusion. Screws are placed into the lateral masses (inferior articular processes) in a divergent trajectory (e.g., Magerl or Anteromedial technique) to avoid nerve root injury and vertebral artery.
- Pedicle Screws: For C7, pedicle screws offer superior biomechanical stability due to their engagement of all three vertebral columns. Pedicle screw placement requires precise technique, often with navigation or intraoperative CT guidance, to avoid neural or vascular injury.
- Rods are contoured to restore or maintain cervical lordosis and then secured to the screws.
-
Decortication of the posterior elements (laminae, facet joints) is performed, and autograft (local bone graft from spinous processes/laminae or iliac crest) or allograft is applied to promote arthrodesis.


These images likely show posterior instrumentation, possibly demonstrating lateral mass screws, pedicle screws, and rods in place, perhaps with a post-operative radiograph.
-
Closure:
- After achieving hemostasis, the paraspinal muscles are reapproximated over the instrumentation and fusion bed. This provides a biological closure, helps contain the bone graft, and reduces dead space. Fascia and skin are closed in layers. A drain may be inserted.
Combined Anterior-Posterior Approaches
A combined approach may be necessary for severe three-column injuries, highly unstable fracture-dislocations, marked kyphotic deformity, or when both anterior and posterior decompression/stabilization are required. This can be performed as a single-stage procedure (often posterior first, then anterior, or vice versa, depending on the primary pathology) or staged.
Complications & Management
Cervical spine surgery, despite advances, carries inherent risks. Understanding common complications and their management is crucial.
TABLE: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Salvage Strategies | - ** Anterior C5-C7
-
Posterior C3-T1
-
Combined C4-C7
-
Spondylolisthesis at C6-7
-
Vertebral Body fractures C5, C6, C7**
A

shows a sagittal view likely of an MRI, revealing significant disc herniation at C5-C6 and C6-C7, causing spinal cord compression. Such a finding in a neurologically compromised patient would be a strong indication for anterior decompression.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional recovery, promoting fusion, and preventing complications. Protocols vary based on the surgical approach, stability of fixation, and patient's neurological status.
-
Immobilization:
- Soft Cervical Collar: Often used for 6-12 weeks following single-level ACDF with stable plating.
- Rigid Cervical Collar (Philadelphia, Miami J): Typically used for 8-12 weeks for multi-level fusions, corpectomies, posterior fusions, or less stable constructs.
- Halo Vest: Rarely used in C3-C7 trauma post-operatively unless there is gross instability, inadequate surgical fixation, or a need for external immobilization to facilitate healing in specific injury patterns.
- The duration of immobilization is determined by radiographic evidence of fusion and clinical stability.
-
Pain Management:
- Aggressive multi-modal pain management is essential in the early post-operative period to facilitate mobilization and participation in therapy.
-
Early Mobilization (as tolerated):
- Out-of-bed activity typically begins on post-operative day 1, with assistance as needed. Emphasis on safe transfers and gait.
- Avoidance of heavy lifting, twisting, and prolonged neck flexion/extension during the initial healing phase.
-
Physical Therapy (Phased Approach):
-
Phase 1 (0-6 weeks – Protection Phase):
- Focus on pain control, wound care, and maintaining spinal precautions.
- Gentle range of motion (ROM) for shoulders and elbows.
- Patient education on proper posture, body mechanics, and avoiding cervical strain.
- Isometric neck exercises may begin gradually under supervision if permitted by the surgeon.
-
Phase 2 (6-12 weeks – Early Strengthening/Mobility Phase):
- Initiate gentle active cervical ROM exercises as permitted by surgeon and fusion status.
- Begin strengthening exercises for scapular stabilizers (rhomboids, trapezius) and deep neck flexors.
- Progressive ambulation and cardiovascular conditioning.
- Continue posture and ergonomic education.
-
Phase 3 (3-6 months – Advanced Strengthening/Return to Activity):
- Progress to more aggressive strengthening of neck musculature (isotonic exercises).
- Proprioceptive and balance training.
- Gradual return to light activities of daily living and work.
- Radiographic assessment for fusion (dynamic X-rays, CT).
-
Phase 4 (6 months+ – Maintenance/Sport-Specific):
- Full return to work and recreational activities, as approved by the surgeon based on clinical and radiographic evidence of solid fusion.
- Sport-specific training and gradual progression to higher impact activities.
- Long-term focus on maintaining core and neck strength.
-
Phase 1 (0-6 weeks – Protection Phase):
-
Neurological Recovery:
- For patients with spinal cord injuries, intensive inpatient rehabilitation focusing on functional independence, assistive device training, and addressing secondary complications (e.g., spasticity, bladder/bowel management) is initiated as soon as medically stable.
Summary of Key Literature / Guidelines
Management of C3-C7 cervical spine injuries has evolved significantly, guided by landmark studies and consensus guidelines.
- Classification Systems: The Subaxial Cervical Spine Injury Classification (SLIC) system is a widely accepted, prognostically relevant classification that assists in guiding surgical decision-making. It incorporates injury morphology, disco-ligamentous complex integrity, and neurological status to assign a score, with higher scores favoring operative intervention.
- Imaging Modalities: The role of CT with multiplanar reconstructions as the primary imaging modality for bony trauma and MRI for soft tissue and neurological assessment (particularly in cases of neurological deficit or normal radiographs) is well-established. Routine use of dynamic flexion-extension radiographs in the acute setting without neurological compromise remains debated but can be helpful for assessing occult instability in awake and cooperative patients.
- Surgical Timing: While early decompression (within 24-72 hours) for incomplete spinal cord injury (ASIA C/D) has shown improved neurological outcomes in some meta-analyses and the STASCIS trial , the optimal timing for stable injuries without neurological compromise is less clear, with no definitive evidence demonstrating superiority of early versus delayed surgery in these contexts.
-
Anterior vs. Posterior Approaches:
The choice of approach is dictated by the specific injury.
- Anterior Cervical Discectomy and Fusion (ACDF) remains the gold standard for single-level radiculopathy and common in multi-level disc herniations and stable fractures. High fusion rates and good outcomes are reported.
- Anterior Cervical Corpectomy and Fusion (ACCF) is reserved for vertebral body fractures with significant anterior canal compromise or kyphosis. While effective, it is associated with higher rates of complications such as dysphagia and pseudarthrosis compared to ACDF.
- Posterior Cervical Fusion (PCF) with lateral mass or pedicle screws is highly effective for posterior tension band injuries, multi-level instability, and reduction of dislocations. It provides robust fixation but may be associated with increased axial neck pain post-operatively.
- Combined approaches are utilized for severe multi-column injuries or irreducible deformities, offering comprehensive decompression and robust fixation, albeit with increased surgical morbidity.
- Graft and Hardware Considerations: Autograft (e.g., iliac crest) remains the gold standard for promoting fusion due to its osteoconductive, osteoinductive, and osteogenic properties, but is associated with donor site morbidity. Allografts and PEEK/titanium cages are widely used, providing structural support with reduced donor site issues. The role of various plate designs (e.g., constrained vs. semi-constrained) continues to be studied, but rigid fixation is generally aimed for.
- Complication Management: Awareness of specific complications such as dysphagia, recurrent laryngeal nerve palsy, C5 palsy, pseudarthrosis, and adjacent segment disease is crucial for prompt recognition and appropriate management. Long-term follow-up studies highlight the risk of adjacent segment disease following fusion.
The continuous evolution of surgical techniques, instrumentation, and rehabilitation protocols aims to improve patient outcomes and minimize morbidity in the complex management of C3-C7 cervical spine injuries. Adherence to established guidelines, coupled with individualized patient assessment, remains paramount.
Clinical & Radiographic Imaging


You Might Also Like