Mastering Posterior Cervical Spine: Applied Surgical Anatomy

Key Takeaway
For anyone wondering about Mastering Posterior Cervical Spine: Applied Surgical Anatomy, Understanding the cervical spine applied surgical anatomy for a posterior subaxial approach is crucial. This safe, midline technique involves identifying landmarks like C2 and C7 spinous processes. Dissection proceeds through the ligamentum nuchae, separating paracervical muscle layers including the trapezius, splenius capitis, and semispinalis capitis, ensuring minimal disturbance to vital structures during surgical access.
Mastering Posterior Cervical Spine: Applied Surgical Anatomy
Introduction & Epidemiology
The posterior approach to the subaxial cervical spine (C3-C7) is a fundamental technique in spine surgery, employed for a spectrum of pathologies including degenerative conditions, trauma, deformity, and oncologic processes. Its versatility lies in providing direct access to the posterior neural elements, laminae, lateral masses, and facet joints, allowing for decompression, stabilization, and deformity correction.
Cervical myelopathy, often resulting from multi-level degenerative changes or ossification of the posterior longitudinal ligament (OPLL), is a primary indication for posterior decompression and/or fusion. Its prevalence increases with age, affecting an estimated 1 in 100,000 individuals annually, with a peak incidence in the sixth decade. Traumatic injuries, such as unstable fractures, dislocations, or facet disruptions, also frequently necessitate posterior stabilization to restore spinal column integrity and protect neural structures. Cervical deformities, particularly kyphosis or sagittal imbalance, can lead to progressive myelopathy and axial neck pain, often requiring complex posterior osteotomies and fusion for correction.
While anterior cervical approaches are typically favored for single-level anterior compression, the posterior approach excels in addressing multi-level compression, posterior pathology, or achieving global cervical alignment restoration. Contemporary understanding of cervical biomechanics and advanced instrumentation has expanded the indications for posterior cervical surgery, emphasizing meticulous surgical planning and anatomical comprehension to optimize patient outcomes and minimize complications.
Surgical Anatomy & Biomechanics
The posterior approach to the subaxial cervical spine necessitates a precise understanding of the layered musculature, ligamentous structures, bony morphology, and critical neurovascular elements. The inherent safety of the midline posterior approach stems from its relatively avascular and internervous plane, minimizing disruption to vital structures.
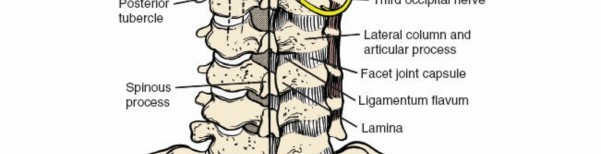
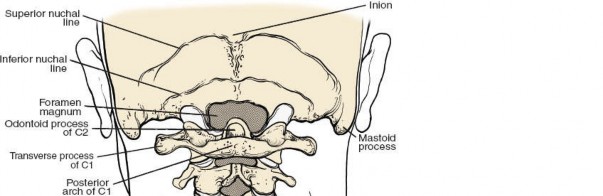
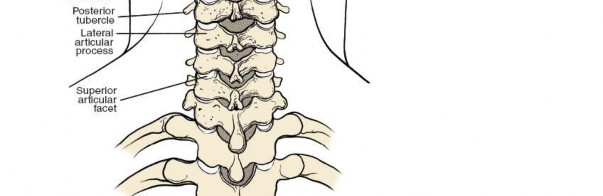
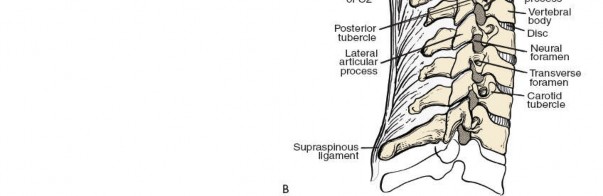
Bony Anatomy and Landmarks
The cervical spinous processes serve as crucial anatomical landmarks for incision planning and intraoperative orientation.
*
C2:
The largest and most prominent bifid spinous process in the upper cervical spine, readily palpable and serving as a key superior reference point.
*
C3-C6:
These spinous processes are typically bifid and relatively small, often less prominent than C2 or C7. Their caudal and posterior orientation provides attachment sites for the cervical musculature.
*
C7:
Characterized by its long, thick, and non-bifid spinous process, which often terminates in a distinct tubercle. It is the most prominent spinous process at the cervicothoracic junction, frequently referred to as the "vertebra prominens," making it an easily palpable distal landmark.

*
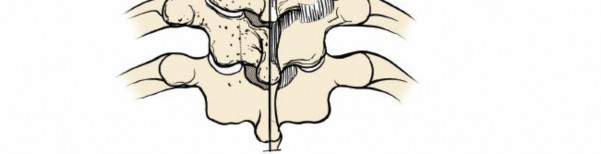
Laminae:
Flat, broad segments forming the posterior arch, connecting the spinous process to the lateral masses.
*
Lateral Masses (Articular Pillars):
The robust bony columns formed by the superior and inferior articular processes. They are critical for posterior instrumentation, particularly lateral mass screw placement. The facet joints, formed by these processes, are typically oriented at approximately 45 degrees to the transverse plane, contributing significantly to cervical range of motion and stability.
*
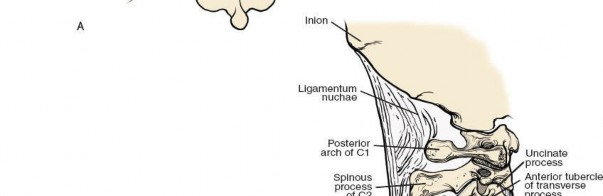
Transverse Processes:
Contain the foramen transversarium, through which the vertebral artery ascends from C6 to C1.
*
Pedicles:
Connect the vertebral body to the posterior elements (laminae and lateral masses). Pedicle screws offer superior pull-out strength but demand precise trajectory due to proximity to the vertebral artery and nerve roots.
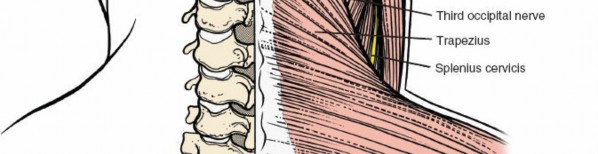
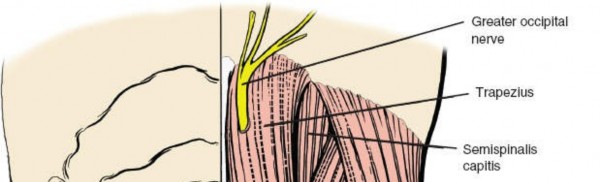
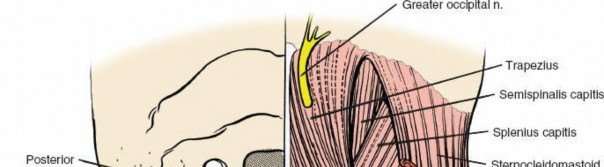
Muscular Anatomy
The muscles covering the posterior aspect of the cervical spine run predominantly longitudinally and are segmentally innervated by the dorsal rami of spinal nerves. A layered understanding is crucial for efficient and minimally disruptive dissection.
*
Superficial Layer:
*
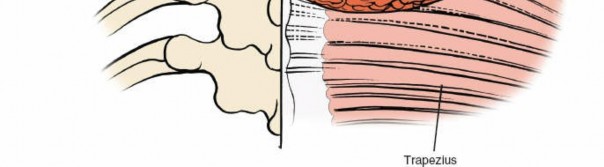
Trapezius:
A large, triangular muscle extending from the occiput to the lower thoracic spine and laterally to the shoulder. Its medial border overlies the cervical paraspinal muscles.
*
Sternocleidomastoid:
Though primarily an anterior muscle, its posterior border forms a significant landmark for the posterior triangle of the neck.
*
Second Layer:
*
Splenius Capitis:
Arises from the lower ligamentum nuchae and upper thoracic spinous processes, inserting into the mastoid process and occiput. Extends the, rotates, and laterally flexes the head.
*
Splenius Cervicis:
Originates from mid-thoracic spinous processes, inserting into C1-C3 transverse processes. Extends and laterally flexes the neck.
*
Third Layer:
*
Semispinalis Capitis:
Lies deep to the splenius capitis, originating from cervical and upper thoracic transverse processes, inserting into the occiput. Extends the head.
*
Semispinalis Cervicis:
Lies deep to the semispinalis capitis, originating from upper thoracic transverse processes, inserting into C2-C5 spinous processes. Extends the neck.
*
Deep Layer (Transversospinalis Group):
These muscles run obliquely from transverse processes to spinous processes, playing a vital role in segmental stability and fine motor control.
*
Multifidus:
Short, thick muscles spanning 2-4 segments.
*
Rotatores:
Even shorter, spanning 1-2 segments.
*
Levator Scapulae:
While primarily a shoulder girdle muscle, it lies laterally to the posterior cervical musculature.
*
Erector Spinae Group (Iliocostalis, Longissimus, Spinalis):
While prominent in the thoracic and lumbar spine, their cervical components (Longissimus Cervicis) are present.
Minimizing muscle stripping and maintaining the midline avascular plane within the ligamentum nuchae helps preserve muscle integrity, reduce postoperative pain, and potentially mitigate the risk of post-laminectomy kyphosis.
Ligamentous Anatomy
- Ligamentum Nuchae: A thick, fibrous, midline septum extending from the external occipital protuberance to the C7 spinous process, serving as an attachment for various muscles and blending with the supraspinous ligament. It is incised in the midline during the posterior approach.
- Supraspinous Ligament: Connects the tips of the spinous processes from C7 caudally.
- Interspinous Ligaments: Connect adjacent spinous processes.
- Ligamentum Flavum: A strong, elastic ligament connecting the laminae of adjacent vertebrae. It is a critical structure removed during laminectomy or laminoplasty to decompress the spinal cord and nerve roots.
- Facet Joint Capsules: Enclose the synovial facet joints, providing stability and limiting excessive motion.
Neurovascular Anatomy
- Spinal Cord: Situated within the vertebral canal, protected by the meninges (dura mater, arachnoid mater, pia mater) and cerebrospinal fluid (CSF). Decompression aims to relieve direct pressure on the cord.
- Cervical Nerve Roots: Exit through the intervertebral foramina. Each subaxial nerve root exits above its corresponding vertebral body (e.g., C5 nerve root exits between C4 and C5). The dorsal rami innervate the deep paraspinal muscles and provide sensory innervation to the posterior neck. Injury to these roots during screw placement or decompression can lead to radiculopathy.
- Vertebral Artery: Courses superiorly through the transverse foramina of C6-C1. It is particularly vulnerable during C1-C2 instrumentation and lateral mass screw placement in the subaxial spine, as its medial aspect is in close proximity to the lateral mass. Understanding the typical trajectory for lateral mass screws (e.g., An, Magerl, Roy-Camille techniques) is paramount to avoid injury.
- Venous Plexuses: Extensive epidural and paraspinal venous plexuses can lead to significant bleeding if not managed meticulously. The midline approach through the ligamentum nuchae minimizes encounter with these structures until deeper dissection.
Biomechanics
The posterior cervical column, comprising the spinous processes, laminae, facet joints, and associated ligaments and muscles, contributes significantly to axial load bearing, flexion-extension, and rotational stability. Disruption of these posterior elements, either traumatically or iatrogenically, can lead to instability or progressive kyphosis. For example, extensive laminectomy without fusion can result in post-laminectomy kyphosis due to the loss of posterior tension band effect and muscle integrity. Fusion constructs aim to restore stability and sagittal balance by rigidly connecting the posterior elements, preventing motion across affected segments. Lateral mass screws primarily resist flexion and extension forces, while pedicle screws offer superior three-column fixation.
Indications & Contraindications
The decision for posterior cervical spine surgery is multifactorial, balancing the patient's symptoms, neurological status, imaging findings, and overall health with the goals of decompression, stabilization, and deformity correction.
Indications for Operative Management
-
Cervical Myelopathy:
- Multi-level compression (typically three or more levels), especially with normal or lordotic sagittal alignment where laminoplasty or laminectomy and fusion can adequately decompress the spinal cord without compromising lordosis.
- Ossification of the Posterior Longitudinal Ligament (OPLL) involving multiple segments, where anterior decompression carries higher risk.
- Myelopathy secondary to posterior pathology (e.g., hypertrophied ligamentum flavum, posterior osteophytes).
- Myelopathy that has failed anterior decompression or recurrence after previous anterior surgery.
-
Cervical Radiculopathy:
- Multi-level radiculopathy where anterior surgery is not feasible or has failed.
- Radiculopathy associated with significant kyphosis requiring posterior correction.
-
Trauma:
- Unstable cervical fractures or fracture-dislocations (e.g., bilateral facet dislocations, burst fractures with significant posterior element involvement).
- Posterior ligamentous complex disruption leading to instability.
- Cervical spondyloptosis.
-
Deformity:
- Cervical kyphosis or severe sagittal imbalance, particularly after previous laminectomy.
- Global cervical deformity requiring multi-level fusion and/or osteotomies.
-
Other:
- Cervical tumors or infections requiring posterior decompression and stabilization.
- Pseudoarthrosis following prior anterior cervical fusion, particularly if associated with instability or progressive deformity.
- Revision surgery for failed anterior instrumentation or inadequate decompression.
Contraindications for Operative Management
-
Absolute Contraindications:
- Severe, uncontrolled systemic infection (e.g., sepsis).
- Uncorrectable coagulopathy.
- Severe medical comorbidities that preclude safe anesthesia and surgery (e.g., unstable angina, severe uncontrolled cardiac failure).
-
Relative Contraindications:
- Predominantly anterior spinal cord compression without significant posterior pathology, especially in a kyphotic spine, where an anterior approach might be more direct for decompression.
- Active local infection at the surgical site.
- Prior extensive posterior cervical surgery with significant scarring, which may increase surgical complexity and risk.
- Severe osteoporosis, which may compromise screw purchase (though newer cement augmentation techniques may mitigate this).
- Morbid obesity, which can increase the technical difficulty of exposure and fixation.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Degenerative Conditions | Multi-level cervical myelopathy, symptomatic multi-level radiculopathy (failed conservative care), significant OPLL. | Physical therapy, cervical orthoses (soft collar), NSAIDs, neuropathic pain medications, epidural steroid injections (for radiculopathy, short-term). |
| Trauma | Unstable fractures (e.g., bilateral facet dislocations, hangman's fractures Type II/III), posterior ligamentous disruption. | Stable compression fractures, minimally displaced fractures without neurological deficit, stable single-column injuries managed with collar immobilization. |
| Deformity | Progressive cervical kyphosis, sagittal imbalance leading to myelopathy or intractable pain. | Bracing (for mild, flexible deformities), physical therapy, postural correction exercises. |
| Infection/Tumor | Spinal cord compression, instability, intractable pain due to tumor/infection. | Antibiotics (for infection), chemotherapy/radiation therapy (for tumors), observation (for stable, asymptomatic lesions). |
| Failed Surgery | Pseudoarthrosis with instability/pain, recurrent myelopathy/radiculopathy after previous surgery, instrumentation failure. | Observation for asymptomatic pseudoarthrosis, pain management for minor symptoms. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and optimal patient positioning are paramount for a safe and effective posterior cervical approach.
Pre-Operative Planning
-
Detailed Imaging Review:
- Plain Radiographs: Anteroposterior, lateral, and flexion-extension views to assess overall alignment, sagittal balance, segmental motion, and gross bony pathology.
- Computed Tomography (CT) Scan: Essential for evaluating bony anatomy in detail, including the morphology of laminae, spinous processes, lateral masses, and pedicles. Crucially, it delineates the course of the vertebral artery within the transverse foramina, which is critical for planning screw trajectories. 3D reconstructions are valuable for complex cases.
- Magnetic Resonance Imaging (MRI): Indispensable for assessing neural element compression (spinal cord, nerve roots), extent of myelomalacia, ligamentous integrity, disc pathology, and any intrinsic spinal cord lesions.
- Screw Templating: Pre-operative CT can be used for virtual templating of screw length, diameter, and trajectory, especially for pedicle screws or cases with aberrant anatomy. This aids in selecting appropriate hardware and minimizing intraoperative risks.
- Neurological Assessment: A thorough pre-operative neurological examination establishes a baseline for monitoring and detecting any post-operative changes.
- Patient Optimization: Medical comorbidities should be optimized. Patients on antiplatelet agents or anticoagulants typically require cessation according to institutional protocols to minimize bleeding risk.
- Informed Consent: Detailed discussion with the patient regarding the surgical plan, potential benefits, risks, and alternatives.
Patient Positioning
The posterior cervical approach is performed with the patient in a prone position.
*
Induction:
Anesthesia is typically induced with the patient supine. Endotracheal intubation is performed, often with a reinforced tube that can tolerate neck manipulation. Baseline neuromonitoring leads are applied.
*
Prone Positioning:
The patient is carefully turned prone onto a specialized surgical table (e.g., Jackson table, Wilson frame, or chest rolls). The key objective is to maintain a lordotic cervical curve while ensuring adequate neck flexion for exposure and preventing abdominal compression.
*
Abdominal Free:
The abdomen must be free to prevent increased intra-abdominal pressure, which can lead to engorgement of the epidural venous plexus, resulting in increased intraoperative bleeding and reduced visibility.
*
Head Fixation:
The head is secured in a rigid skull clamp (e.g., Mayfield three-pin head holder). The head holder allows for precise positioning and stabilization of the cervical spine throughout the procedure. The degree of neck flexion is critical: excessive flexion can exacerbate cord compression in myelopathic patients, while insufficient flexion may hinder exposure. The goal is often a neutral or slightly flexed position to facilitate exposure and maintain lordosis.
*
Shoulder Taping:
The shoulders are pulled caudally with adhesive tape applied to the shoulders and secured to the foot of the bed. This maneuver depresses the shoulders, improving fluoroscopic visualization of the lower cervical spine and cervicothoracic junction (C7-T1).
*
Arm Positioning:
Arms are tucked at the sides or positioned on arm boards in a safe, padded manner, ensuring no pressure points.
*
Neuromonitoring:
Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs) are continuously monitored throughout the positioning and surgical phases to detect potential intraoperative neural compromise. Electromyography (EMG) is also utilized to monitor nerve root function.
*
Fluoroscopy:
The C-arm fluoroscopy unit should be positioned to allow for immediate anteroposterior and lateral imaging to confirm levels and assist with instrumentation.
Detailed Surgical Approach / Technique
The posterior approach to the subaxial cervical spine is characterized by its midline trajectory, minimizing vital structure disruption.
Incision
The skin on the back of the neck is thicker and less mobile than anterior cervical skin. It is intimately attached to the underlying fascia.
*
Marking:
The incision length is determined by the number of levels requiring treatment. It typically extends from the C2 spinous process superiorly to the C7/T1 level inferiorly, spanning the required segments. The incision runs perpendicular to the skin tension lines for optimal wound healing.
*
Skin Incision:
A sterile marking pen is used to delineate the incision line, which is then infiltrated with local anesthetic (e.g., lidocaine with epinephrine) for hemostasis and postoperative pain control. The skin and subcutaneous tissue are incised precisely along the midline.

Subcutaneous Dissection
- Electrocautery: The dissection proceeds through the subcutaneous fat layer using electrocautery, aiming for the deep cervical fascia and the ligamentum nuchae in the midline. Careful hemostasis is maintained.
-
Deep Fascia:
The superficial layer of deep cervical fascia is incised along the midline, exposing the underlying ligamentum nuchae.

Muscle Dissection
- Ligamentum Nuchae Incision: The key to a bloodless and anatomically correct posterior cervical approach is to incise the ligamentum nuchae in the exact midline. This is an avascular plane.
-
Subperiosteal Dissection:
Using Cobb elevators or similar instruments, the paraspinal muscles are meticulously stripped subperiosteally off the spinous processes and laminae. The dissection is extended laterally to expose the facet capsules and the lateral masses.
- It is crucial to stay directly on the bone to avoid muscle injury and excessive bleeding.
- For multi-level fusions, adequate exposure of the lateral masses from C3 to C7 is essential for screw placement.
- For laminoplasty, the muscle attachments may be preserved on one side (hinge side) or carefully reattached after decompression.
- Modern techniques, such as the "C-arm muscle flap" or muscle-sparing approaches, aim to minimize muscle stripping and preserve the integrity of the posterior cervical musculature, potentially reducing postoperative axial neck pain and risk of kyphosis.
-
Self-retaining retractors are carefully placed to maintain exposure.





Identification of Levels
-
Fluoroscopic Confirmation:
After exposure, a radiopaque marker (e.g., needle, clamp) is placed on a known spinous process (e.g., C2 or C7), and a lateral fluoroscopic image is obtained to confirm the correct surgical levels. This step is critical to prevent wrong-level surgery.


Decompression Techniques
Laminectomy
- Procedure: Resection of the spinous processes, laminae, and ligamentum flavum to decompress the spinal cord.
-
Steps:
- Remove spinous processes at the target levels using ronguers.
- Use a high-speed burr or kerrison ronguers to thin and resect the laminae, starting at the caudal and cephalad ends of the laminectomy extent.
- Carefully dissect the ligamentum flavum from the dura, typically starting from the midline and progressing laterally.
- The lateral extent of the laminectomy should be medial to the facet capsules to preserve stability and avoid nerve root injury at the foramen.
- Ensure complete decompression of the spinal cord by visualizing the pulsatile dura.
Laminoplasty
- Concept: Enlarges the spinal canal by creating a hinge on one side and cutting the lamina on the other, or by splitting the lamina in the midline. The opened laminar arch is then held open with small plates. This technique maintains posterior bony elements, theoretically reducing the risk of post-laminectomy kyphosis.
-
Types:
- Open-Door (Unilateral Hinge): A trough is created on one side (the hinge side) with a high-speed burr, maintaining the integrity of the outer cortical bone. The lamina on the contralateral side is cut completely. The opened door is then elevated and fixed in an expanded position with mini-plates and screws.
- French-Door (Midline Split): A midline split is created through the spinous processes and laminae. Hinges are created bilaterally at the junction of the lamina and lateral mass. The "doors" are then opened and secured with plates.
-
Key Steps:
-
Confirm levels.

-
Create the hinge and cut lines with a high-speed burr.

-
Carefully elevate the lamina, ensuring the dura is free.

-
Insert and secure laminoplasty plates.


-
Confirm levels.
Posterior Cervical Fusion (PCF)
PCF involves decompression (if needed), preparation of bony surfaces, bone graft placement, and rigid internal fixation using screws and rods.
-
Preparation for Fusion:
- Decortication: The lateral masses, laminae, and facet joints at the fusion levels are decorticated using a high-speed burr or ronguers to create a bleeding bed, promoting osteointegration.
- Graft Placement: Autograft (e.g., local autograft from spinous processes/laminae, iliac crest bone graft) or allograft (e.g., cancellous chips) is packed into the decorticated beds, particularly over the lateral masses and across the facet joints.
-
Instrumentation:
-
Lateral Mass Screws (C3-C7):
These are the most common screws used in subaxial posterior cervical fusion due to their relative safety and good biomechanical stability.
-
Entry Points and Trajectories:
- Roy-Camille Technique: Entry point at the center of the lateral mass. Trajectory 30 degrees lateral and 30-45 degrees superior.
- Magerl Technique: Entry point at the intersection of the midpoint of the lateral mass and a line bisecting the inferior facet. Trajectory 20-30 degrees lateral and 30-45 degrees superior. This aims towards the anterior-superior corner of the lateral mass.
- An/Anderson Techniques: Variations emphasizing different entry points or angles. Generally, an upward and outward trajectory is preferred to avoid nerve root injury (inferior and medial) and vertebral artery injury (lateral and anterior).
-
Technique:
- Mark the entry point on the lateral mass.
- Use a small burr or awl to create a cortical breach.
- Drill a pilot hole (typically 2.0 mm) to the appropriate depth (14-18 mm) using a drill guide and stop.
- Probe the screw tract with a ball-tipped probe to confirm complete bony containment. No violation of the anterior or medial cortex should be detected.
- Tap the hole (if non-self-tapping screws).
- Insert the appropriately sized polyaxial screw.
-
Entry Points and Trajectories:
-
C3-C7 Pedicle Screws:
Offer superior pullout strength and three-column fixation but carry a higher risk of vertebral artery or nerve root injury due to their complex and variable anatomical trajectory. Pre-operative CT planning and navigation systems are highly recommended.
- Entry Point: Typically at the junction of the lamina, lateral mass, and transverse process.
- Trajectory: Varies significantly by level. Generally, a medial and superior trajectory is required.
- Technique: Similar to lateral mass screws, but meticulous attention to trajectory and probing is critical.
-
Occipital-Cervical Fusion (OCF):
For instability or deformity involving the occiput and upper cervical spine.
- Occipital Screws: Placement within the thickest part of the occipital bone, often lateral to the midline and superior to the nuchal ridge.
- C1 Lateral Mass Screws: Entry point typically at the midpoint of the C1 posterior arch, trajectory toward the anterior arch. Care must be taken to avoid the vertebral artery, which wraps around the lateral mass.
- C2 Pedicle/Pars Screws: Excellent fixation. C2 pedicle screws are similar to subaxial pedicle screws. C2 pars interarticularis screws follow a path through the pars.
-
Rods:
Contoured to match the desired sagittal alignment (typically lordotic) and connected to the screws with locking caps. Distraction or compression may be applied to achieve reduction or aid lordosis.





-
Lateral Mass Screws (C3-C7):
These are the most common screws used in subaxial posterior cervical fusion due to their relative safety and good biomechanical stability.
Wound Closure
- Hemostasis: Thorough irrigation and meticulous hemostasis are critical to prevent postoperative hematoma.
- Drain Placement: A closed suction drain is often placed deep to the muscle fascia to manage postoperative bleeding and reduce the risk of hematoma formation.
- Layered Closure: The deep fascia (including the ligamentum nuchae) is meticulously reapproximated to restore the muscle envelope. The subcutaneous tissue is closed, and finally, the skin is closed with sutures or staples.
Complications & Management
Despite advancements in surgical techniques, complications can occur with posterior cervical spine surgery. Anticipation and prompt management are crucial for optimal outcomes.
Intraoperative Complications
-
Dural Tear and CSF Leak:
- Incidence: 1-5%. More common with revision surgery, OPLL, or severe canal stenosis.
- Management: Immediate recognition is paramount. Small tears can often be repaired primarily with 6-0 Prolene sutures. Larger tears may require a dural patch (autologous fascia, muscle, or allograft/synthetic patch) with fibrin sealant. A lumbar drain may be considered postoperatively in persistent leaks or high-risk cases.
-
Nerve Root Injury:
- Incidence: 1-3%. Can occur during decompression, especially with lateral dissection, or during screw placement if trajectory is incorrect (e.g., medial violation of foramen).
- Management: Prevention through careful surgical technique and neuromonitoring. If identified intraoperatively, assess the cause (e.g., misplaced screw, direct trauma). Malpositioned screws require immediate revision. Postoperatively, observation, neuropathic pain medications (gabapentin, pregabalin), and physical therapy.
-
Spinal Cord Injury:
- Incidence: <1%. A devastating complication, often due to direct trauma during decompression, excessive manipulation, or acute loss of spinal alignment.
- Management: Prevention through meticulous technique, intraoperative neuromonitoring (SSEP/MEP changes warrant immediate attention: check blood pressure, remove instrumentation, ensure adequate decompression, consider awakening patient for neurological exam). If a significant deficit is noted, immediate post-operative imaging (MRI) and medical management (e.g., high-dose steroids, though controversial) are initiated.
-
Vertebral Artery Injury (VAI):
- Incidence: <0.5% with pedicle screws; extremely rare with lateral mass screws. Higher risk during C1-C2 fixation.
- Management: Direct compression for several minutes often controls bleeding. If persistent, local packing with hemostatic agents may be needed. Definitive treatment can range from observation to surgical repair, or endovascular embolization in selected cases. Consultation with vascular or interventional radiology is essential.
-
Excessive Bleeding:
- Incidence: Variable, often related to epidural venous plexus engorgement (due to prone positioning with abdominal compression) or extensive muscle dissection.
- Management: Meticulous hemostasis throughout the case with electrocautery, bipolar cautery, bone wax, and hemostatic agents. Optimize patient positioning to free the abdomen. Transfusion support as needed.
Postoperative Complications
-
Surgical Site Infection (SSI):
- Incidence: 1-4%.
- Management: Superficial infections typically respond to oral antibiotics. Deep infections require aggressive debridement, intravenous antibiotics, and potentially hardware removal if persistent or associated with osteomyelitis.
-
Hematoma:
- Incidence: 1-2%. Can cause delayed neurological deficit due to spinal cord compression.
- Management: Close monitoring for neurological decline or significant wound drainage. Evacuation of the hematoma is indicated for neurological compromise. Drains are routinely used to prevent this.
-
C5 Palsy:
- Incidence: 3-10% after posterior decompression (laminectomy or laminoplasty). Presents as deltoid and/or biceps weakness.
- Management: The etiology is likely multifactorial (reverberation injury, reperfusion injury, spinal cord shift, nerve root tethering). Often self-limiting, typically resolving over 6-12 months. Management includes observation, physical therapy, and neuropathic pain medications.
-
Pseudoarthrosis (Non-Union):
- Incidence: 5-15% after fusion. Higher in smokers, multi-level fusions, and patients with poor bone quality.
- Management: Asymptomatic pseudoarthrosis may be observed. Symptomatic pseudoarthrosis (persistent pain, instability) often requires revision surgery with additional bone grafting and potentially supplemental fixation.
-
Instrumentation Failure:
- Incidence: 2-5%. Includes screw pullout, rod fracture, or screw breakage.
- Management: If symptomatic or associated with pseudoarthrosis/instability, revision surgery is indicated to replace or augment the instrumentation.
-
Proximal or Distal Junctional Kyphosis (PJK/DJK):
- Incidence: 5-10% after long segment fusions or extensive laminectomies. Occurs due to stress shielding at the adjacent segment or continued degeneration.
- Management: Prevention involves careful attention to sagittal balance and selecting appropriate fusion levels. Symptomatic PJK/DJK (pain, myelopathy) may require extension of the fusion or osteotomy to restore alignment.
-
Axial Neck Pain:
A common complaint after posterior surgery, thought to be related to muscle stripping and denervation. Can be chronic.
- Management: Physical therapy, NSAIDs, muscle relaxants. Techniques to minimize muscle damage (e.g., C-arm muscle flap) are increasingly utilized.
Complications and Management Strategies
| Complication | Incidence (approx.) | Salvage/Management Strategy |
|---|---|---|
| Dural Tear / CSF Leak | 1-5% | Primary repair, dural patch, fibrin sealant. Lumbar drain for persistent/high-output leaks. Bed rest. |
| Nerve Root Injury | 1-3% | Observation, neuropathic pain medications, physical therapy. Revision hardware if malposition identified. |
| Spinal Cord Injury | <1% | Immediate evaluation (imaging, neurological exam), correction of mechanical factors, medical management (e.g., blood pressure control). |
| Vertebral Artery Injury | <0.5% | Direct compression, hemostatic agents, packing. Surgical repair or endovascular embolization if bleeding is uncontrolled. |
| Surgical Site Infection | 1-4% | IV antibiotics. Surgical debridement and irrigation for deep infections. Hardware removal in chronic/refractory cases. |
| Hematoma | 1-2% | Close neurological monitoring. Urgent surgical evacuation if causing neurological compromise. |
| C5 Palsy | 3-10% | Observation, neuropathic pain medications, physical therapy. Spontaneous recovery common. |
| Pseudoarthrosis | 5-15% | Observation (if asymptomatic). Revision surgery with re-grafting/augmentation of fixation if symptomatic. |
| Instrumentation Failure | 2-5% | Revision surgery with hardware replacement or augmentation if symptomatic or unstable. |
| Junctional Kyphosis | 5-10% | Observation (if asymptomatic). Extension of fusion or corrective osteotomy if symptomatic or progressive. |
| Chronic Axial Neck Pain | Up to 50% | Physical therapy, NSAIDs, muscle relaxants, ergonomic modifications. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional recovery, managing pain, and ensuring successful integration of the surgical construct. Protocols vary depending on the extent of surgery (laminectomy/laminoplasty vs. fusion), patient comorbidities, and surgeon preference.
Immediate Post-Operative Period (Day 0-7)
- Pain Management: Multimodal analgesia (opioids, NSAIDs, acetaminophen, muscle relaxants) to control incisional pain and muscle spasm.
- Mobilization: Early mobilization is encouraged, typically within 24 hours. Patients are assisted out of bed for ambulation.
-
Cervical Orthosis:
- Laminectomy/Laminoplasty: Often managed with a soft cervical collar for comfort and proprioceptive input for 2-4 weeks.
- Fusion: Typically a rigid cervical collar (e.g., Miami J, Aspen) is prescribed for 6-12 weeks to provide external support, limit motion, and protect the fusion construct during the initial healing phase.
- Wound Care: Instructions on dressing changes and signs of infection.
Early Rehabilitation (Weeks 2-6)
-
Physical Therapy (PT):
Initiated based on surgeon protocol.
- Laminectomy/Laminoplasty: Gentle range of motion exercises, postural re-education, scapular stabilization. Avoidance of extreme neck flexion/extension.
- Fusion: Continued rigid collar wear. Gentle, non-weight-bearing exercises for extremities. Emphasis on core stability and maintaining good posture. Avoid any active cervical range of motion.
- Activity Restrictions: No heavy lifting (>10-15 lbs), pushing, pulling, or overhead activities. Avoid driving (especially with rigid collar). Avoid prolonged sitting.
Mid-Phase Rehabilitation (Weeks 6-12)
- Cervical Orthosis Weaning: For fusion patients, gradual weaning from the rigid collar is typically initiated around 6-8 weeks, transitioning to a soft collar, then off, based on radiographic evidence of fusion and clinical stability.
-
Progressive PT:
- Fusion: Once radiographic signs of fusion are evident, a gradual increase in active cervical range of motion exercises, gentle isometric strengthening, and proprioceptive training.
- Laminectomy/Laminoplasty: Continued strengthening of cervical musculature, improving endurance and flexibility.
- Activity Progression: Gradual return to light activities of daily living. Continued restrictions on strenuous activities.
Late Rehabilitation & Return to Activity (Months 3-6+)
- Radiographic Assessment: Fusion status is assessed with dynamic radiographs and/or CT scan.
- Advanced PT: Focus on progressive resistance exercises for neck and shoulder girdle, functional movement patterns, and sport-specific training (if applicable).
- Return to Work/Sport: Phased return based on fusion status, neurological recovery, and functional capacity. High-impact sports or heavy manual labor are typically restricted until 6-12 months post-fusion, with clear radiographic evidence of solid arthrodesis.
- Patient Education: Emphasis on ergonomic principles, proper lifting techniques, and maintaining an active lifestyle to prevent future issues.
Summary of Key Literature / Guidelines
The body of literature guiding posterior cervical spine surgery is extensive, evolving with technological advancements and biomechanical understanding.
-
Laminectomy vs. Laminoplasty vs. Fusion for Myelopathy:
- For multi-level cervical myelopathy with a preserved cervical lordosis, laminoplasty is often favored over laminectomy for its potential to maintain cervical motion and reduce the incidence of post-operative kyphosis, while providing equivalent neurological outcomes. Studies by Hirabayashi et al. and results from the Japanese Orthopaedic Association have largely established laminoplasty's efficacy.
- Laminectomy alone, especially for three or more levels, carries a significant risk of post-laminectomy kyphosis (PLK) and should generally be combined with posterior cervical fusion, particularly in patients with pre-existing kyphosis or compromised posterior ligamentous complex.
- Posterior cervical fusion is indicated for multi-level myelopathy with significant kyphosis, instability, or where correction of sagittal balance is paramount. Long-segment fusions can effectively restore lordosis but carry a risk of junctional problems.
-
Instrumentation:
- Lateral Mass Screws: Biomechanically stable and generally safe for C3-C7 fixation. The Roy-Camille and Magerl techniques are widely accepted with reported vertebral artery injury rates below 1%.
- Pedicle Screws: Offer superior biomechanical pull-out strength and three-column fixation but pose a higher risk to the vertebral artery and nerve roots. Their use is often reserved for specific indications (e.g., revision surgery, high-grade instability, deformity correction) and increasingly relies on navigation systems (fluoroscopy-based, CT-based, or robotic) to enhance accuracy and safety. Systematic reviews highlight their efficacy but underscore the importance of precision.
- Occipito-Cervical Fusion: A critical technique for craniocervical instability, often combining occipital plates with C1 lateral mass and C2 pedicle/pars screws.
- Minimally Invasive Approaches: While challenging, muscle-sparing approaches and percutaneous screw placement techniques are being explored to reduce soft tissue dissection, postoperative pain, and potentially enhance recovery, though long-term data on their superiority over open techniques is still emerging.
- Neuromonitoring: Intraoperative SSEP, MEP, and EMG monitoring are standard of care, providing real-time assessment of neural function and acting as an early warning system for impending neurological injury, significantly improving safety.
- Guidelines: Organizations like the North American Spine Society (NASS) and AOSpine publish evidence-based guidelines and clinical commentaries that serve as valuable resources for surgical decision-making and technique. These emphasize comprehensive patient assessment, appropriate surgical indications, and meticulous execution. The growing evidence base continually refines surgical practices, aiming to improve neurological outcomes, reduce complication rates, and enhance patient quality of life.
Clinical & Radiographic Imaging

You Might Also Like

