Mastering the Rectus Abdominis Muscle in Lumbar Anterior Approach
Key Takeaway
We review everything you need to understand about Mastering the Rectus Abdominis Muscle in Lumbar Anterior Approach. The rectus abdominis muscle is encountered during the superficial dissection of the anterior approach to the lumbar spine. After incising the skin and subcutaneous tissue, the linea alba is cut, exposing this muscle, particularly in the lower abdomen. It is then separated by finger pressure to access the posterior rectus sheath and peritoneum, facilitating the surgical procedure.
Mastering the Rectus Abdominis Muscle in Lumbar Anterior Approach
Introduction & Epidemiology
The anterior lumbar interbody fusion (ALIF) approach represents a critical surgical corridor to the ventral lumbar spine, predominantly utilized for L4-L5 and L5-S1 pathologies. Its utility extends across various indications including degenerative disc disease, spondylolisthesis, pseudoarthrosis, and certain spinal deformities requiring sagittal balance correction. The anterior approach offers several advantages over posterior methods, such as direct access to the disc space allowing for larger cage insertion, superior biomechanical load sharing, reduced muscle dissection (specifically paraspinal musculature), and potentially lower rates of epidural fibrosis.
Epidemiologically, the adoption of ALIF has seen fluctuations but remains a significant component of the lumbar fusion armamentarium. The prevalence of degenerative disc disease continues to rise with an aging population, driving demand for reconstructive spinal procedures. While the overall incidence of ALIF is less than posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF), its specific indications and favorable biomechanical profile ensure its sustained relevance. Critical to the success of the anterior approach is a meticulous understanding and execution of the abdominal wall dissection, particularly concerning the rectus abdominis muscle, its associated fascial planes, and neurovascular supply. Preservation of abdominal wall integrity and function is paramount to minimize iatrogenic morbidity and optimize patient recovery.
Surgical Anatomy & Biomechanics
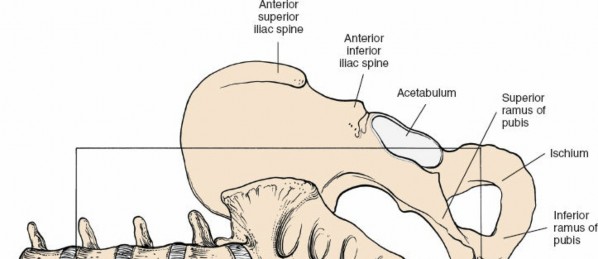
The anterior approach to the lumbar spine necessitates a staged dissection through the abdominal wall, traversing superficial, intermediate, and deep compartments. The superficial stage, which directly involves the rectus abdominis muscle and its sheath, is critical for establishing the initial surgical corridor.
Superficial Anatomy:
- Skin and Subcutaneous Tissues: The initial incision penetrates these layers. The thickness varies significantly with patient habitus.
-
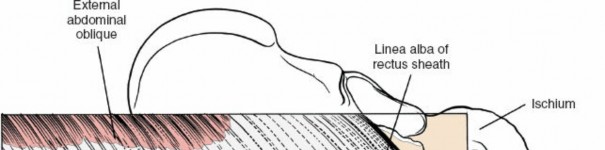
Linea Alba:
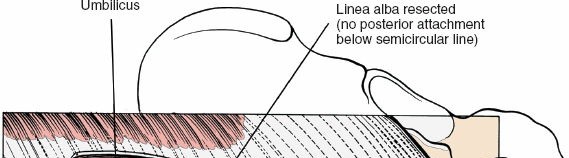
This fibrous raphe, formed by the decussation of aponeuroses of the external oblique, internal oblique, and transversus abdominis muscles, runs in the midline from the xiphoid process to the pubic symphysis. It is avascular and provides a relatively straightforward entry point for midline incisions. The umbilicus typically lies superficial to the linea alba, serving as a key anatomical landmark, usually positioned midway between the pubic symphysis and the infrasternal notch, though its position can vary, particularly in obese individuals.

Incision over the Linea Alba:

-
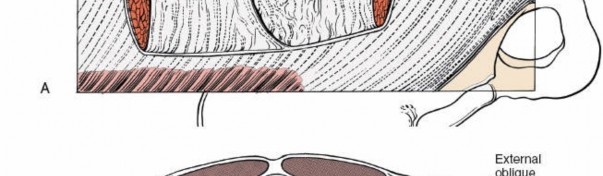
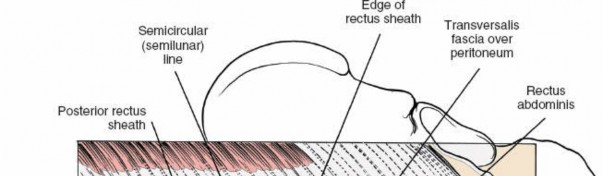
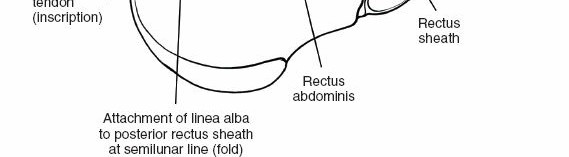
Rectus Abdominis Muscle (RA):
Paired muscles running vertically on either side of the linea alba, from the pubic crest and symphysis to the costal cartilages of the 5th, 6th, and 7th ribs and the xiphoid process. They are segmented by three to four tendinous intersections, which are typically adherent to the anterior rectus sheath.
-
Rectus Sheath:
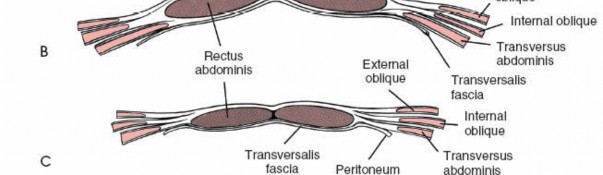
This strong fibrous compartment encloses the rectus abdominis muscles. Its composition varies significantly above and below the arcuate line (linea semicircularis), which typically lies halfway between the umbilicus and the pubic symphysis.
- Above the Arcuate Line: The anterior rectus sheath is formed by the aponeuroses of the external oblique and the anterior lamina of the internal oblique. The posterior rectus sheath is formed by the posterior lamina of the internal oblique and the transversus abdominis aponeurosis.
-
Below the Arcuate Line:
All three abdominal muscle aponeuroses (external oblique, internal oblique, and transversus abdominis) pass anterior to the rectus abdominis, forming a robust anterior rectus sheath. Posteriorly, only the transversalis fascia and peritoneum cover the rectus abdominis. This anatomical distinction is crucial as it dictates the integrity of the posterior abdominal wall and the approach to the preperitoneal space.

Incision of the Anterior Rectus Sheath:
-
Neurovascular Supply of the Rectus Abdominis:
- Innervation: The rectus abdominis is innervated by the ventral rami of the lower six or seven thoracic spinal nerves (T7-T12), also known as the thoracoabdominal nerves. These nerves course between the internal oblique and transversus abdominis muscles, piercing the posterior rectus sheath to enter the deep surface of the rectus muscle.
-
Blood Supply:
The primary blood supply comes from the superior epigastric artery (terminal branch of the internal thoracic artery) superiorly, and the inferior epigastric artery (branch of the external iliac artery) inferiorly. These vessels anastomose within the rectus muscle. Segmental perforating branches also contribute to the supply. Preservation of these neurovascular bundles, particularly the inferior epigastric vessels when approaching the lower lumbar spine, is critical to maintain rectus abdominis viability and minimize the risk of muscle atrophy or denervation.



Rectus Muscles Separated:
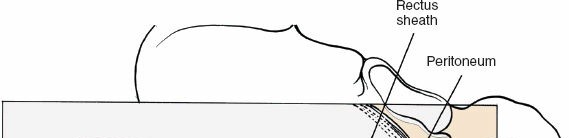
Posterior Rectus Sheath and Peritoneum:
-
Rectus Sheath:
This strong fibrous compartment encloses the rectus abdominis muscles. Its composition varies significantly above and below the arcuate line (linea semicircularis), which typically lies halfway between the umbilicus and the pubic symphysis.
Intermediate Stage Anatomy:
The intermediate stage involves entry into the preperitoneal space and displacement of the peritoneum and its contents. While not directly involving the rectus abdominis, the extent of peritoneal mobilization can influence the retraction required of the rectus muscle. Key structures include:
*
Preperitoneal Fat:
A layer of adipose tissue separating the posterior rectus sheath (or transversalis fascia) from the parietal peritoneum.
*
Peritoneum:
A thin, serous membrane lining the abdominal cavity. Its integrity must be preserved where possible, and if incised, meticulously repaired.
*
Bowel:
Small and large intestines, which are gently mobilized and packed away.
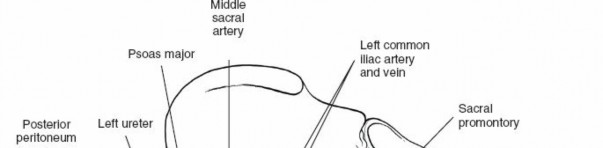
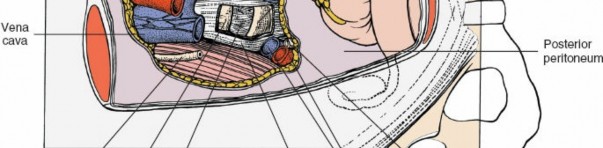
Deep Stage Anatomy (Retroperitoneal):
The deep stage of dissection focuses on mobilizing retroperitoneal structures to access the anterior lumbar spine. These include:
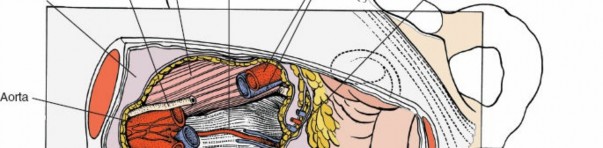
*
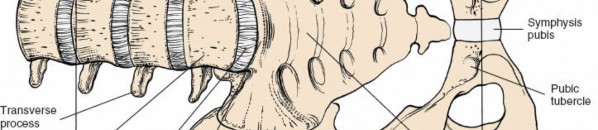
Great Vessels:
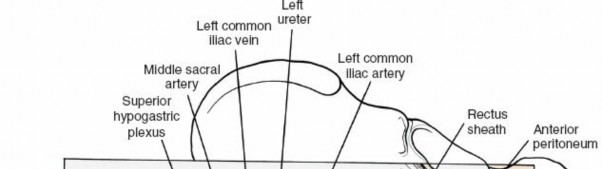
Aorta, inferior vena cava, common iliac arteries and veins. Their precise anatomical variations and relationships to the target disc levels (L4-5, L5-S1) are crucial for safe dissection.
*
Lumbar Vessels:
Segmental lumbar arteries and veins typically cross anterior to the lumbar vertebral bodies. These must be identified and ligated or cauterized to prevent hemorrhage.
*
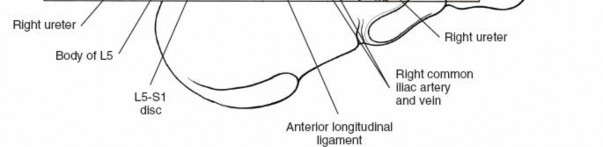
Ureter:
Courses retroperitoneally and must be identified and protected, typically along the medial aspect of the psoas muscle.
*
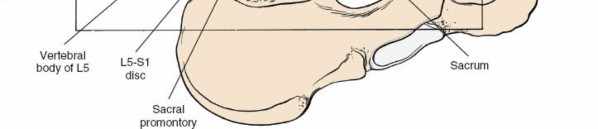
Presacral Plexus (Superior Hypogastric Plexus):
Lies anterior to the L5-S1 disc space and sacral promontory. Injury to this plexus can lead to retrograde ejaculation in males.




Biomechanics of Rectus Abdominis Dissection:
The integrity of the anterior abdominal wall, heavily reliant on the rectus abdominis and its fascial sheaths, is fundamental for core stability and preventing incisional herniation.
*
Midline vs. Paramedian Incisions:
*
Midline (Linea Alba):
This approach directly separates the rectus muscles via an incision through the linea alba. While avascular, excessive retraction can stretch or damage the tendinous intersections or the rectus muscles themselves. Closure of the linea alba is critical for integrity.
*
Paramedian:
This approach involves incising the anterior rectus sheath lateral to the linea alba and either splitting the rectus muscle longitudinally or retracting it laterally. Longitudinal splitting, especially in the inferior abdomen where tendinous intersections are less robust, carries a risk of denervation if the thoracoabdominal nerve branches are transected. Lateral retraction, a more common contemporary technique, aims to preserve the muscle fibers and their innervation by creating a plane between the rectus muscle and the posterior rectus sheath. However, aggressive or prolonged retraction can still lead to muscle injury, hematoma, or nerve neuropraxia.
*
Prevention of Hernia and Diastasis:
Meticulous closure of the rectus sheath is paramount. Failure to adequately reapproximate the anterior rectus sheath can lead to rectus diastasis or incisional hernia, impacting core strength and patient comfort.
Indications & Contraindications
The anterior lumbar approach is a versatile tool in spinal surgery, but careful patient selection is critical.
Indications (Operative)
| Category | Specific Conditions | Rationale for ALIF |
|---|---|---|
| Degenerative | Single or multi-level degenerative disc disease (DDD) refractory to conservative management, L4-S1 levels. | Direct discectomy, large cage for enhanced stability, restoration of disc height and foraminal decompression. |
| Spondylolisthesis | Low-grade degenerative or isthmic spondylolisthesis (Grade I-II). | Restoration of sagittal alignment, direct anterior column support for stability. |
| Spinal Deformity | Adult degenerative scoliosis requiring sagittal balance correction (e.g., lordosis restoration at L4-S1). | Significant anterior column lengthening and lordosis creation, often combined with posterior fixation. |
| Pseudoarthrosis | Failed posterior fusion requiring revision, particularly at L5-S1. | Access to undisturbed anterior fusion bed, avoids scar tissue from previous posterior surgery. |
| Trauma | Select thoracolumbar fractures with anterior column compromise requiring reconstruction, not primarily a posterior approach. | Restoration of anterior column height and stability. |
| Tumor | Anterior column stabilization or debulking for metastatic disease, primary spinal tumors. | Direct access for tumor resection and reconstruction. |
| Adjacent Segment Disease | Symptomatic adjacent segment disease following previous lumbar fusion. | Direct access to disc without disturbing posterior hardware or scar tissue. |
Contraindications
Absolute Contraindications:
*
Active Intra-abdominal Infection:
Risk of spreading infection.
*
Severe Coagulopathy:
Uncontrolled bleeding risk.
*
Extensive Abdominal Adhesions:
Prior multiple abdominal surgeries, especially those involving the retroperitoneum, can make safe access extremely difficult and increase visceral injury risk.
*
Unrepaired Abdominal Aortic Aneurysm (AAA) or Ilio-Femoral Aneurysm:
Risk of rupture.
*
Significant Vascular Disease:
Severe atherosclerosis of the great vessels, especially if calcified or tortuous, increases risk of injury.
*
Morbid Obesity with difficult vascular anatomy:
May preclude safe access or require excessive retraction, increasing complication risk.
Relative Contraindications:
*
Prior Abdominal Surgery:
History of extensive abdominal surgery, particularly retroperitoneal or pelvic procedures (e.g., appendectomy, hysterectomy, prostatectomy), increases adhesion risk but is not always prohibitive if adhesions are localized.
*
High-grade Spondylolisthesis (Grade III+):
While some surgeons perform ALIF for these, posterior reduction and fixation may be safer and more effective.
*
Pelvic Radiation Therapy:
Can cause significant scarring and altered vascularity, increasing dissection difficulty and complication rates.
*
Severe Osteopenia/Osteoporosis:
Risk of cage subsidence or instrumentation failure.
*
Urological Conditions:
Presence of horseshoe kidney or other significant renal anomalies may alter retroperitoneal anatomy.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is paramount for minimizing complications and optimizing outcomes in anterior lumbar approaches.
Pre-Operative Planning
-
Clinical Evaluation:
- Detailed History and Physical Exam: Assess neurological deficits, abdominal surgical history (adhesions), vascular risk factors, and core strength.
- Surgical Clearance: Obtain medical clearance, particularly from cardiology and anesthesia, given the typically longer operative times and potential for significant blood loss.
-
Imaging Assessment:
- Standard Radiographs: AP, lateral, flexion/extension views to assess alignment, instability, and overall spinal architecture.
- MRI: Essential for evaluating disc pathology, neural element compression, and ruling out other intraspinal pathologies.
- CT Scan: Crucial for bone morphology, osteophyte assessment, and fusion assessment in revisions.
- Vascular Imaging (CT Angiogram/MRA): Absolutely mandatory. This allows detailed mapping of the great vessels (aorta, vena cava, common iliacs) relative to the lumbar spine, identifying tortuosity, aneurysms, anomalies (e.g., left-sided vena cava), and presence of atherosclerotic plaque. It informs incision planning, determines which side provides safer access, and identifies segmental lumbar vessel anatomy.
- Multidisciplinary Consultation: Collaboration with a vascular or general surgeon experienced in anterior retroperitoneal access is highly recommended, especially for fellows and residents. This partnership optimizes safe vessel mobilization and closure.
- Blood Management: Type and cross-match blood. Consider pre-operative autologous donation or cell saver use, though often not necessary for single-level ALIF.
- Patient Education and Consent: Discuss potential risks, including retrograde ejaculation (males), vascular injury, incisional hernia, and bowel injury.
Patient Positioning
The patient is positioned supine on a radiolucent operating table.
*
Arms:
Tucked to the sides to allow full access for the surgical team and fluoroscopy.
*
Legs:
Straight, with a pillow or gel pad under the knees for comfort and to prevent nerve compression. Appropriate padding for heels, elbows, and other pressure points.
*
Support:
A small bolster under the lumbar spine can sometimes be used to accentuate lumbar lordosis for easier cage insertion, or removed to flatten the lumbar spine slightly to aid initial dissection, depending on surgeon preference and sagittal goals.
*
Fluoroscopy:
Ensure adequate fluoroscopic imaging capability in both AP and lateral planes for precise localization of the target levels.
*
Foley Catheter:
Inserted to decompress the bladder and protect the ureters during dissection.
*
Nasogastric Tube:
May be inserted to decompress the stomach and bowel, particularly in cases where extensive retraction is anticipated, though often not strictly necessary for standard ALIF.
*
Sterile Prep:
Wide sterile prep from the sternum to mid-thigh, laterally to both flanks.
Detailed Surgical Approach / Technique
The anterior lumbar approach is typically performed in concert with a general or vascular surgeon assisting with the initial abdominal access and vascular mobilization. The procedure can be divided into distinct stages.
1. Incision and Superficial Dissection
-
Incision Selection:
-
Midline Incision:
Preferred by many surgeons for L5-S1 fusion. A vertical incision is made just above or below the umbilicus, extending inferiorly towards the pubic symphysis. This directly accesses the avascular linea alba, minimizing rectus muscle damage.

-
Paramedian (Left Oblique) Incision:
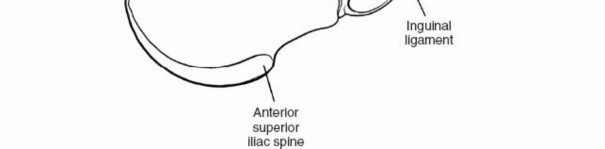
Often favored for L4-L5 access due to the typical right-sided position of the vena cava. A transverse or oblique incision is made inferior and medial to the anterior superior iliac spine (ASIS), usually on the left side, allowing for a retroperitoneal trajectory. This approach requires careful handling of the rectus abdominis.


-
Midline Incision:
Preferred by many surgeons for L5-S1 fusion. A vertical incision is made just above or below the umbilicus, extending inferiorly towards the pubic symphysis. This directly accesses the avascular linea alba, minimizing rectus muscle damage.
-
Skin and Subcutaneous Layers:
Incise skin and subcutaneous fat down to the anterior rectus sheath. Control bleeding meticulously.

-
Anterior Rectus Sheath:
- Midline Approach: Incise the linea alba longitudinally.
-
Paramedian Approach:
Incise the anterior rectus sheath longitudinally, parallel to the rectus fibers.

-
Rectus Abdominis Muscle Management:
- Midline Approach: Once the linea alba is incised, the rectus muscles are identified on either side. These are then retracted laterally using blunt finger dissection or self-retaining retractors. This separates the muscles without violating their integrity or neurovascular supply.
-
Paramedian Approach:
The rectus muscle is encountered beneath the incised anterior rectus sheath. The preferred method is
lateral retraction
of the rectus muscle. This involves carefully developing a plane between the posterior surface of the rectus abdominis and the posterior rectus sheath (or transversalis fascia) and retracting the entire muscle belly medially. Care must be taken to identify and preserve the thoracoabdominal nerves and inferior epigastric vessels entering the posterior aspect of the rectus muscle. Historically, rectus splitting was employed, but this increases the risk of denervation and abdominal wall weakness.

-
Posterior Rectus Sheath and Transversalis Fascia:
Beneath the rectus muscle (or after its lateral retraction), the posterior rectus sheath is encountered (above the arcuate line) or the transversalis fascia (below the arcuate line). This layer is then incised, exposing the preperitoneal fat.

2. Intermediate Stage: Preperitoneal and Peritoneal Dissection
-
Preperitoneal Space:
Using blunt dissection, the preperitoneal fat is entered. This avascular plane is developed, sweeping the peritoneum and its contents medially.

-
Peritoneal Mobilization:
The parietal peritoneum is identified. The goal is to perform a true retroperitoneal dissection, retracting the peritoneum (with the small and large intestines) entirely to one side (typically to the right for a left-sided approach, to the left for a midline approach to L5-S1 if the right common iliac artery is to be mobilized). This keeps the bowel out of the field and minimizes the risk of ileus. In some cases, a small peritoneal tear may occur, which should be repaired meticulously at the end of the case.

3. Deep Stage: Retroperitoneal Exposure of the Lumbar Spine
-
Identification of Key Structures:
-
Great Vessels:
The aorta and vena cava are the most prominent structures. The aorta is typically on the left, the vena cava on the right. Below L4, they typically branch into common iliac vessels. A meticulous dissection identifies the bifurcation and the iliac vessels.
- Ureter: Identified by its peristaltic movements, usually lying over the psoas muscle. It should be gently retracted out of the field.
- Sympathetic Plexus: A fine neural plexus located anterior to the great vessels, particularly important at L5-S1. Damage can cause retrograde ejaculation in males.
-
Great Vessels:
The aorta and vena cava are the most prominent structures. The aorta is typically on the left, the vena cava on the right. Below L4, they typically branch into common iliac vessels. A meticulous dissection identifies the bifurcation and the iliac vessels.
-
Vessel Mobilization:
- For L5-S1: The vessels are typically mobilized to the left. The left common iliac vein crosses anterior to the L5-S1 disc space in a variable fashion. Careful blunt dissection in the plane between the vascular adventitia and the anterior longitudinal ligament allows mobilization. Segmental lumbar arteries and veins crossing the disc space must be identified and ligated with clips or sutures.
-
For L4-L5:
The vessels may be mobilized either to the left or right, depending on the specific anatomy and the side chosen for access. The common iliac vessels branch higher at this level, and direct aortic/IVC mobilization is more common.


- Anterior Longitudinal Ligament (ALL): Once the vessels are safely retracted, the ALL is exposed. A longitudinal incision is made in the ALL to expose the annulus fibrosus and the underlying disc.
- Disc Space Localization: Confirm the correct level using fluoroscopy.
4. Spinal Stage: Discectomy, Fusion, and Fixation
- Discectomy: Incise the annulus. Perform a thorough discectomy, removing all disc material, including the cartilaginous endplates. Preserve the cortical bone of the endplates to optimize fusion.
- Endplate Preparation: Prepare the endplates using curettes and rasps to create a bleeding, cancellous bed for fusion.
- Cage Insertion: Select an appropriately sized interbody cage (titanium, PEEK, or expandable) filled with autograft, allograft, or bone morphogenetic protein (BMP). Impact the cage firmly to restore disc height, stabilize the segment, and potentially provide lordotic correction.
- Supplemental Fixation: Depending on the surgical indication, cage type, and surgeon preference, supplemental anterior plating or screws may be applied for additional stability, particularly in deformity cases or multi-level fusions.
5. Closure
- Hemostasis: Ensure meticulous hemostasis in the retroperitoneal space.
- Vessel Repositioning: Carefully release retraction on the great vessels, ensuring no kinks or compression.
- Peritoneal Repair: If a peritoneal tear occurred, it should be closed with absorbable suture.
- Rectus Sheath Closure: This is a critical step for preventing incisional hernia. The posterior rectus sheath (if incised) and then the anterior rectus sheath (or linea alba) are closed with strong, non-absorbable or slowly absorbable sutures in a running or interrupted fashion. Ensure robust reapproximation of fascial layers.
- Subcutaneous Tissue and Skin: Close the subcutaneous layers and skin in a standard fashion.
Complications & Management
Complications associated with the anterior lumbar approach can be significant, necessitating a comprehensive understanding of their incidence, recognition, and management strategies.
| Complication Category | Specific Complication | Incidence (Approximate) | Salvage Strategies / Management |
|---|---|---|---|
| Vascular | Iliac vein injury | 1-15% | Immediate pressure, vascular surgeon repair (suture/patch), liberal use of clips/sutures for segmental vessels. Urgent laparotomy if unrecognized. |
| Iliac artery injury | <1-5% | Immediate pressure, vascular surgeon repair, urgent control of hemorrhage. | |
| Aorta/Vena Cava injury | <1% | Immediate pressure, vascular surgeon repair. High morbidity/mortality. | |
| Segmental vessel bleeding | 5-10% | Meticulous ligation/cauterization of lumbar vessels during initial dissection. Controlled clipping with appropriate length to avoid clip migration. | |
| Neurological | Retrograde Ejaculation (males) | 0-15% | Careful identification and preservation of the superior hypogastric plexus (presacral plexus) anterior to L5-S1. Generally irreversible. |
| Ureteral injury | <1% | Identification and protection of ureters. If injured, urological consultation for repair (stenting, primary repair). | |
| Femoral Nerve injury | Rare | Careful retraction and positioning. Usually neuropraxia, managed conservatively. | |
| Abdominal Wall | Incisional Hernia | 1-5% | Meticulous closure of rectus sheath/linea alba. Surgical repair (primary or mesh reinforcement) if symptomatic. |
| Abdominal wall weakness/diastasis | 1-3% | Proper rectus muscle retraction (not splitting), careful closure. Core strengthening post-operatively. Repair if severe and symptomatic. | |
| Ileus | 5-20% | Gentle bowel handling, early mobilization, limited oral intake initially. Nasogastric tube for severe cases. Usually self-limiting. | |
| Wound infection | 1-3% | Standard sterile technique, appropriate prophylactic antibiotics. Debridement and antibiotics if superficial; re-exploration if deep. | |
| Hematoma | 2-5% | Meticulous hemostasis during closure. Drains rarely used. Re-exploration for expanding hematoma. | |
| Spinal | Graft migration/subsidence | 5-10% | Proper endplate preparation, appropriately sized cage, supplemental fixation when indicated. Revision surgery if symptomatic. |
| Pseudoarthrosis | 5-15% | Optimize fusion environment (biological augmentation), proper technique. Revision surgery (anterior or posterior) for symptomatic nonunion. | |
| Instrumentation failure | <2% | Proper selection and insertion of hardware. Revision and possible supplemental fixation. | |
| Other | Deep Vein Thrombosis (DVT)/PE | <1% | Standard DVT prophylaxis (pharmacological/mechanical). |
Management Principles:
*
Prevention:
The cornerstone of complication management is meticulous pre-operative planning, precise anatomical identification, and careful surgical technique. Collaborative surgery with a vascular or general surgeon can significantly mitigate vascular and visceral risks.
*
Recognition:
High index of suspicion for complications, especially vascular injury, which can rapidly lead to catastrophic outcomes. Close intraoperative monitoring of vital signs and communication with the anesthesia team.
*
Acute Management:
*
Vascular Injury:
Immediate direct pressure, clear visualization of the injury, and prompt vascular repair by an experienced surgeon. Preparedness with vascular clamps, sutures, and patches.
*
Bowel Injury:
Immediate repair by a general surgeon.
*
Peritoneal Tear:
Meticulous closure with absorbable sutures to prevent evisceration or adhesions.
*
Post-Operative Management:
Close monitoring for signs of ileus, infection, or expanding hematoma. Early recognition and intervention are critical.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following anterior lumbar fusion focuses on pain management, early mobilization, abdominal wall recovery, and gradual return to activity, tailored to the individual patient and fusion construct.
Immediate Post-Operative Period (Days 0-7)
- Pain Management: Multimodal analgesia including opioids, NSAIDs (if no contraindication), acetaminophen, and possibly nerve blocks. Goal is effective pain control to facilitate mobility.
-
Mobilization:
- Day 0-1: Out of bed to chair, short ambulation with assistance. Focus on gentle turning, logrolling, and independent transfers.
- Day 2+: Progressive ambulation, increasing distance and frequency. Avoid prolonged sitting.
-
Abdominal Wall Care:
- Incision Site: Keep clean and dry. Monitor for signs of infection or hematoma.
- Gentle Core Engagement: Instruct patients on gentle, non-straining core activation during transfers and ambulation. Avoid valsalva maneuvers.
- Diet: Advance diet as tolerated, typically starting with clear liquids and progressing to solids once bowel function returns and ileus is ruled out.
- Bracing: Typically, a lumbar orthosis is not required for a single-level ALIF with a stable construct. However, it may be indicated for multi-level fusions, osteoporotic patients, or specific deformity corrections requiring additional support.
-
Activity Restrictions:
- No bending, lifting (more than 5-10 lbs), or twisting (BLT precautions) for the initial 6-12 weeks.
- Avoid prolonged standing or sitting.
Early Rehabilitation Phase (Weeks 2-6)
- Pain Management: Transition from opioid to non-opioid analgesics.
- Activity: Continue progressive ambulation. Stationary cycling (low resistance) or elliptical may be introduced as tolerated.
-
Physical Therapy (PT):
Begin formal outpatient PT.
- Focus: Gentle core stabilization exercises, pelvic tilts, isometric abdominal contractions. Education on proper body mechanics.
- Avoid: Abdominal crunches, sit-ups, or activities that place significant strain on the abdominal incision.
- Incision: Monitor for any signs of incisional hernia or delayed wound healing.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Imaging: Follow-up radiographs at 6 weeks and 3 months to assess fusion progression.
- Activity: Gradually increase activity levels. May introduce light resistance training for extremities.
-
Physical Therapy:
Progress core strengthening, focusing on endurance and stability.
- Introduce exercises such as bird-dog, planks (modified), and controlled leg slides.
- Emphasis on proprioception and neuromuscular control.
- Driving: May be cleared to drive if off opioid pain medication and reaction time is adequate.
- Lifting: Gradually increase lifting restrictions based on fusion status and pain levels.
Advanced Rehabilitation Phase (Months 3-6+)
- Imaging: Follow-up radiographs at 6 months and 1 year to confirm solid fusion.
- Activity: Continue to advance activity levels, incorporating functional movements and return-to-sport specific training for athletes.
- Physical Therapy: Advanced core strengthening, balance training, and sport-specific drills. Focus on restoring full strength and flexibility.
- Return to Work: Gradual return to work, potentially with modified duties, depending on the physical demands of the occupation.
- Full Activity: Generally, patients can return to full unrestricted activity, including contact sports, by 6-12 months post-surgery, assuming solid fusion.
Key Considerations for Rectus Abdominis Recovery:
*
Avoid Early Strain:
The rectus sheath closure is under tension, and excessive strain (e.g., heavy lifting, forceful coughing/straining) in the early post-operative period can lead to dehiscence or hernia formation.
*
Gradual Strengthening:
Abdominal exercises should be introduced gradually and cautiously. Isometric contractions are safer initially than dynamic movements.
*
Diastasis Recti:
While the rectus sheath is closed, patients should be educated on recognizing signs of rectus diastasis, though this is primarily a cosmetic concern unless associated with a fascial hernia.
Summary of Key Literature / Guidelines
The literature on anterior lumbar interbody fusion is extensive, continuously evolving, and offers robust evidence supporting its efficacy and defining best practices.
1. Efficacy and Outcomes:
* Numerous meta-analyses and systematic reviews consistently demonstrate that ALIF is an effective procedure for achieving lumbar fusion, providing pain relief, and improving functional outcomes for degenerative disc disease and spondylolisthesis. Fusion rates typically range from 85-95%, comparable to or sometimes exceeding posterior approaches, particularly at L5-S1.
* ALIF has shown favorable biomechanical properties, allowing for optimal disc height restoration and indirect neural decompression, thereby addressing sagittal imbalance effectively. Studies by authors such as Mummaneni et al. and Pimenta have highlighted the role of ALIF in complex adult spinal deformity correction.
2. Comparison to Other Fusion Techniques:
*
ALIF vs. PLIF/TLIF:
While posterior approaches offer direct decompression of neural elements, ALIF provides superior load-bearing capacity and a larger footprint for interbody devices, potentially leading to higher fusion rates and better restoration of disc space height and lumbar lordosis. The absence of posterior paraspinal muscle dissection is another cited advantage, potentially reducing muscle-related morbidity.
* However, ALIF is associated with a distinct set of complications, particularly vascular and retrograde ejaculation, which are less common with posterior approaches. The choice between ALIF and posterior techniques often depends on the specific pathology, surgeon expertise, and patient comorbidities.
3. Abdominal Wall Considerations:
*
Incision Type and Rectus Management:
Literature supports that careful rectus abdominis handling is critical. Studies comparing midline trans-linea alba incisions with paramedian muscle-splitting or muscle-retracting approaches have generally shown muscle retraction to be superior to muscle splitting in terms of preserving abdominal wall integrity and reducing post-operative pain or weakness. A true retroperitoneal paramedian approach is often preferred for L4-L5 access to avoid excessive peritoneal manipulation and reduce ileus risk.
*
Incisional Hernia:
The incidence of incisional hernia post-ALIF is relatively low but remains a significant concern. Meticulous, layered closure of the rectus sheath/linea alba with strong, often non-absorbable sutures, is consistently recommended in surgical guidelines to minimize this risk. Some authors advocate for mesh reinforcement in high-risk patients, though this is not standard practice for primary ALIF.
4. Vascular Complications:
* Vascular injury, particularly to the iliac veins, remains the most feared complication, with reported incidences varying widely based on surgeon experience and definition. The critical importance of pre-operative CT angiogram/MRA to delineate individual vascular anatomy and identify anomalies (e.g., left-sided vena cava, tortuous atherosclerotic vessels) is universally emphasized in contemporary guidelines.
* The role of a dedicated vascular or general surgeon for exposure and vessel mobilization is strongly advocated in training programs and by experienced spinal surgeons to reduce vascular morbidity.
5. Sympathetic Nerve Injury (Retrograde Ejaculation):
* Injury to the superior hypogastric plexus (presacral plexus) resulting in retrograde ejaculation is a well-documented risk. Meticulous blunt dissection of the ALL directly over the disc space, minimizing lateral sweeping or thermal injury, is key to preserving these delicate nerve fibers. Counseling male patients pre-operatively about this specific risk is standard practice.
6. Long-Term Outcomes:
* Long-term follow-up studies confirm the durability of ALIF in achieving fusion and maintaining clinical improvement. However, adjacent segment disease remains a concern with any fusion procedure, and patient selection and careful construct planning are essential to minimize its occurrence.
In conclusion, mastering the rectus abdominis muscle in the anterior lumbar approach necessitates a deep understanding of abdominal wall anatomy, meticulous surgical technique for muscle and fascial handling, and a commitment to preserving neurovascular structures. Adherence to established guidelines, thorough pre-operative planning including advanced vascular imaging, and often a multidisciplinary surgical approach are foundational to optimizing patient safety and achieving durable clinical success.
Clinical & Radiographic Imaging

You Might Also Like