Adult Idiopathic Scoliosis: Comprehensive Surgical Management Guide
Key Takeaway
Adult idiopathic scoliosis (AIS) presents unique biomechanical and clinical challenges compared to adolescent forms. Management requires a profound understanding of global sagittal balance, rigid deformity correction, and robust lumbosacral fixation. This guide details evidence-based surgical indications, advanced osteotomy techniques, pelvic fixation strategies, and postoperative protocols to optimize patient outcomes and mitigate complications like proximal junctional kyphosis and pseudarthrosis.
Adult Idiopathic Scoliosis: Pathophysiology and Clinical Paradigm
The management of adult spinal deformities, particularly adult idiopathic scoliosis (AIS) and degenerative scoliosis, necessitates a distinct clinical and surgical paradigm compared to adolescent idiopathic scoliosis. Adult idiopathic scoliosis is fundamentally defined as a scoliotic curve exceeding 10 degrees in the coronal plane with associated structural changes, diagnosed in an individual older than 20 years of age. These curves are typically sequelae of adolescent idiopathic scoliosis, where the diagnosis was either delayed, non-operative management failed, or the curve progressed insidiously into adulthood.
The prevalence of adult scoliosis, encompassing both idiopathic and de novo degenerative forms, ranges from 4% to 6% in the general population. While AIS exhibits a female-to-male ratio similar to its adolescent counterpart, late-onset degenerative scoliosis demonstrates a marked female predominance, affecting approximately 60% of patients. Degenerative curves are characteristically shorter, primarily localized to the lumbar spine, and generally less severe in coronal magnitude than those observed in AIS. Patients with degenerative scoliosis frequently present with symptoms of spinal stenosis, and any myelographic defects are typically confined within the primary curve.
The overarching therapeutic objective for degenerative scoliosis is the alleviation of axial back pain and neurogenic claudication. In stark contrast, the treatment goals for adult idiopathic scoliosis are significantly broader, encompassing intractable pain control, prevention of neurological compromise, comprehensive three-dimensional deformity correction, and a paramount emphasis on restoring global spinal balance.
Sagittal Balance: The Cornerstone of Spinal Alignment
A profound understanding of normal sagittal plane relationships is indispensable in the evaluation and surgical treatment of adult spinal deformities. The human spine exhibits primary kyphotic curvatures in the thoracic and sacral regions, which are inherent from fetal development. Secondary lordotic curvatures, developing in the cervical and lumbar spine between 5 and 15 years of age, emerge as adaptations to upright posture.
Sagittal balance refers to the intricate alignment that optimally centers the head over the pelvis or hips in both the sagittal and coronal planes, minimizing muscular energy expenditure for upright posture. A critical radiographic parameter is the sagittal vertical axis (SVA), determined by a plumb line dropped from the center of the C7 vertebral body. On a lateral long-cassette radiograph, this plumb line should normally fall through or slightly behind the posterosuperior corner of the S1 endplate. Normal SVA values are typically reported as −3.2 ± 3.2 cm.
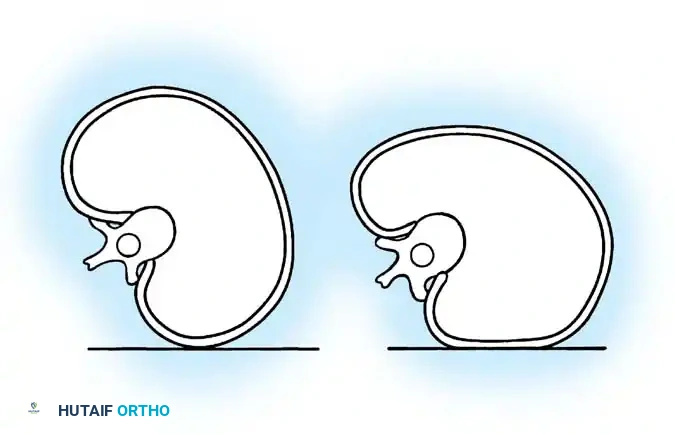
Fig. 41-12 Segmental sagittal measures of thoracic and lumbar spine. Note the critical contribution of the L4-5 and L5-S1 discs to overall lumbar lordosis (67%). (From Bernhardt M, Bridwell KH: Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction, Spine 14:717, 1989.)
Segmental and Regional Interrelationships
The thoracolumbar junction (T10-L2) represents a critical transitional zone where the thoracic kyphosis transitions into lumbar lordosis. The first lordotic disc is typically observed at L1-2. Normal thoracolumbar alignment, measured from the cephalad T12 endplate to the caudal L2 endplate, ranges from 0 to −10 degrees.
The lumbar spine is characterized by its lordotic curvature, with maximal segmental lordosis concentrated at the L4-5 and L5-S1 disc levels. The sagittal apex of the lumbar spine is usually located at L3. It is noteworthy that over 60% of total lumbar lordosis is generated by the L4-5 and L5-S1 discs, contributing approximately −20 degrees and −28 degrees, respectively, to the regional lordotic measurement. The maintenance of these normal segmental and regional interrelationships is paramount for preserving global spinal balance and preventing iatrogenic flatback syndrome.
Clinical Pearl: Bridwell's "sagittal clock" provides a highly useful intraoperative and radiographic heuristic. On a lateral radiograph with the patient facing the surgeon's right, the apical L3 disc or endplate should point towards the 3 o'clock position, L4 towards 4 o'clock, and L5 towards 5 o'clock. Strict adherence to this regional alignment significantly mitigates the risk of postoperative flatback deformity.
Dynamic Compensation and Global Balance
Static normal values for kyphosis and lordosis, while informative, are less useful in isolation due to the dynamic nature of spinal curves. A truly "normal" spine is a balanced spine. Compensatory changes occur throughout the spine to maintain global balance; for instance, increased cervical or lumbar lordosis often correlates with increased thoracic kyphosis.
The fundamental principle of deformity correction is that normal thoracic kyphosis must be adequately balanced by lordosis in the lumbar and cervical spines to ensure the C7 plumb line falls appropriately. A practical guideline, derived from the Schwab-SRS classification, suggests that Lumbar Lordosis (LL) should be within 9 degrees of Pelvic Incidence (PI), expressed as PI - LL < ±9°.
Epidemiology and Natural History of Curve Progression
Adult idiopathic scoliosis most commonly presents clinically in patients in their late 30s to 50s. Population studies indicate a prevalence of 2% to 4% for curves greater than 10 degrees, with an estimated 500,000 adults in the United States alone exhibiting coronal curves exceeding 30 degrees.
The classic longitudinal data by Weinstein and Ponseti on the natural history of adult scoliosis highlights the relentless progressive nature of these curves. Thoracic curves greater than 50 degrees typically progress at approximately 1 degree per year until they reach about 75 degrees, after which the progression rate decelerates to roughly 0.3 degrees per year, eventually stabilizing around 90 degrees.
Lumbar curves, however, demonstrate a more aggressive and clinically symptomatic progression, advancing at a rate of 0.4 to 0.5 degrees per year once they exceed 30 degrees. This accelerated progression in lumbar curves, coupled with the high incidence of associated degenerative changes, often warrants a more proactive surgical management approach.
Predictors of lumbar curve progression include:
* L5 positioned above the intercristal line.
* Apical vertebral rotation exceeding 30% (Nash-Moe Grade III or IV).
* An unbalanced or decompensated curve (significant trunk shift).
* A concomitant thoracic curve greater than 50 degrees.
* A thoracolumbar or lumbar curve greater than 30 degrees.
Importantly, significant pulmonary complications are rare in patients with AIS, even with curves exceeding 100 degrees, unless severe thoracic lordosis is present. Therefore, surgical intervention is generally not indicated solely to maintain or improve pulmonary function in adults.
Comprehensive Clinical Evaluation
Symptomatology and Pain Generators
Back pain is a prevalent symptom, affecting 60% to 80% of patients with scoliosis. However, 25% to 80% of patients with adult idiopathic curvatures present with pain as their chief complaint, distinguishing them from the adolescent population. Pain characteristics include mechanical axial back pain (often on the convexity of the curve due to muscle fatigue), buttock pain, and radiculopathy or neurogenic claudication.
Neurogenic claudication occurs in approximately 13% of patients and typically results from degenerative changes (facet hypertrophy, ligamentum flavum buckling) within or distal to the primary lumbar curve. Radiculopathy, affecting about 4% of patients, is usually due to nerve root entrapment within the narrowed foramina on the concavity of the curve or lateral recess stenosis on the convexity due to rotatory subluxation.
Physical Examination and Neurological Assessment
Physical examination must be meticulous and systematic:
* Skin Inspection: Examine for pathological lesions (café-au-lait spots, hairy patches) suggesting underlying intraspinal anomalies.
* Neurological Assessment: A comprehensive neurological examination, including documentation of reflexes, motor strength, and sensory perception, is mandatory to establish a baseline and identify subtle deficits.
* Deformity Assessment:
* Forward Bending Test (Adam's Test): Evaluates structural rib and lumbar paraspinal prominence. If rib prominence exceeds 3 cm, a thoracoplasty should be considered during surgical correction.
* Trunk Shift: Identified by dropping a plumb line from the C7 spinous process; measure the deviation from the gluteal cleft.
* Shoulder Balance: Assess clavicle angle and T1 tilt. Instrumentation of a structural upper thoracic curve must extend to T2 or T3 to prevent postoperative shoulder imbalance.
* Limb-Length Inequality: Must be assessed using blocks to level the pelvis, as this can artificially exacerbate coronal decompensation.
Anatomy, Biomechanics, and Bone Quality Considerations
Adult idiopathic scoliosis shares anatomical features with AIS but is uniquely complicated by diminished elasticity of ligamentous structures, facet arthropathy, and progressive narrowing of disc spaces. These factors collectively contribute to profound stiffness and rigidity, making surgical correction significantly more challenging and often necessitating advanced osteotomy techniques.
Osteopenia and osteoporosis are critical considerations in older patients. Compromised bone quality directly impacts the biomechanics of the bone-implant interface, increasing the risk of pedicle screw pullout, proximal junctional kyphosis (PJK), and pseudarthrosis. Preoperative DEXA scanning is highly recommended; patients with a T-score < -2.0 may require preoperative anabolic bone optimization (e.g., Teriparatide) for 3-6 months prior to elective deformity surgery.
Surgical Warning: The lumbosacral junction presents a formidable biomechanical challenge due to the long lever arm created by extensive thoracolumbar instrumentation and the inherently poor cancellous bone quality in the sacrum. Stopping a long construct at L5 is historically associated with a high rate of adjacent segment disease and L5-S1 disc degeneration. If fusing to the sacrum, robust pelvic fixation is an absolute requirement to prevent construct failure.
Diagnostic Imaging and Preoperative Planning
Standard Radiography and Flexibility Assessment
Standard, full-length (36-inch) standing anteroposterior (AP) and lateral radiographs of the entire spine are mandatory.

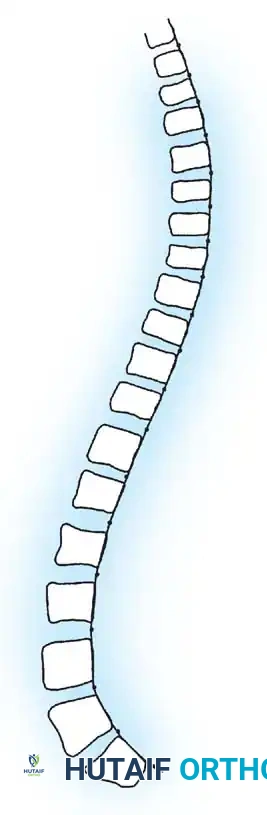
Fig. 41-13 Preoperative standing AP radiograph demonstrating a severe, decompensated adult idiopathic scoliotic curve. Note the significant coronal translation and rotatory subluxation at the lumbar levels.
- AP View: Used to measure the Cobb angle, assess Nash-Moe vertebral rotation, and identify coronal decompensation (C7 plumb line offset from the central sacral vertical line).
- Lateral View: Essential for evaluating PI, PT, SS, LL, TK, and SVA. The PI-LL mismatch is the most critical calculation for preoperative planning.
- Flexibility Views: Supine side-bending radiographs, or fulcrum bending films, are critical for assessing curve flexibility. Rigid curves that do not correct on bending films will require aggressive posterior column osteotomies or anterior release to achieve balance.
Advanced imaging, including MRI of the entire spine, is required for any patient with neurological symptoms, severe pain, or prior to any planned osteotomy to evaluate for central canal stenosis, foraminal narrowing, or tethered cord. CT myelography is an excellent alternative for patients with pacemakers or severe artifact from previous instrumentation.
Indications for Surgical Intervention
Surgical management of adult idiopathic scoliosis is a major undertaking and should be reserved for patients who have failed exhaustive conservative measures (physical therapy, NSAIDs, targeted epidural steroid injections).
Primary Surgical Indications:
1. Documented Curve Progression: Progression of >5 degrees over a 1-2 year period, particularly in lumbar curves >30 degrees or thoracic curves >50 degrees.
2. Intractable Pain: Severe, mechanically reproducible axial back pain or radicular pain that significantly impairs activities of daily living and is refractory to non-operative care.
3. Neurological Deficit: Progressive motor weakness, myelopathy, or severe neurogenic claudication.
4. Severe Sagittal or Coronal Imbalance: SVA > 5 cm, PI-LL mismatch > 10 degrees, or significant coronal decompensation leading to postural fatigue and inability to maintain horizontal gaze.
Surgical Management: Approaches and Techniques
The surgical strategy must be individualized based on curve rigidity, sagittal parameters, and the presence of neurological compression. The modern gold standard is a posterior-only approach utilizing pedicle screw instrumentation and various grades of osteotomies, though anterior/posterior combined approaches remain valuable for rigid lumbar curves.
Patient Positioning and Neuromonitoring
Patients are positioned prone on a Jackson spinal table. The abdomen must hang completely free to decrease intra-abdominal pressure, thereby reducing epidural venous engorgement and intraoperative blood loss. The hips are extended to maximize lumbar lordosis during instrumentation. Multimodal intraoperative neuromonitoring (IONM), including Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is mandatory. Baseline signals are obtained prior to positioning and monitored continuously.
Spinal Osteotomies and Thoracoplasty
To mobilize a rigid adult spine, posterior osteotomies are frequently required. The choice of osteotomy depends on the degree of correction needed:
- Smith-Petersen Osteotomy (SPO) / Ponte Osteotomy: Involves resection of the facet joints and ligamentum flavum. Provides approximately 5-10 degrees of sagittal correction per level and significant coronal flexibility.
- Pedicle Subtraction Osteotomy (PSO): A three-column closing wedge osteotomy through the pedicles and vertebral body. Indicated for sharp, angular kyphotic deformities or severe fixed sagittal imbalance. Provides 25-35 degrees of lordosis at a single level.
- Vertebral Column Resection (VCR): Complete resection of one or more vertebral segments. Reserved for the most severe, rigid, and complex multiplanar deformities.
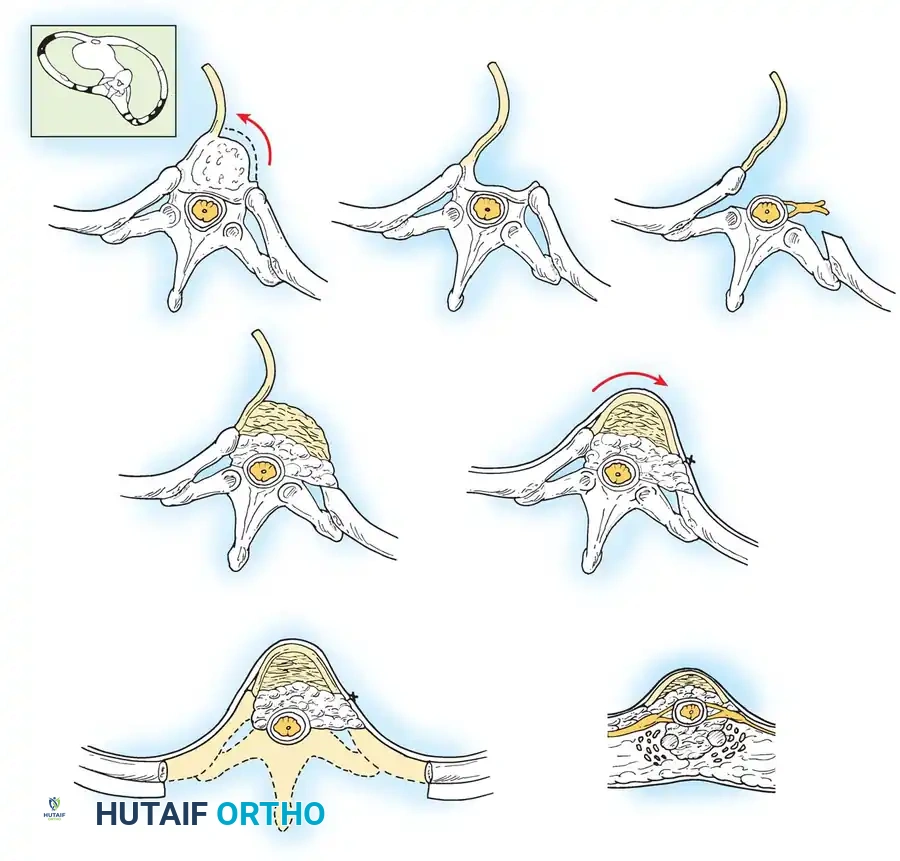
Fig. 41-14 Schematic representation of a posterior column osteotomy and concurrent thoracoplasty. Resection of the prominent rib segments on the convexity not only improves cosmetic appearance but provides excellent autograft for the fusion bed.
Posterior Spinal Fusion and Instrumentation
A meticulous subperiosteal exposure is performed out to the tips of the transverse processes bilaterally. Facetectomies are performed at all levels to be fused to ensure a robust posterior fusion mass.
Pedicle screws are the anchor of choice due to their superior biomechanical pullout strength and ability to control the spine in all three planes. Screws are placed using freehand anatomic landmarks, fluoroscopy, or modern robotic/navigation assistance.
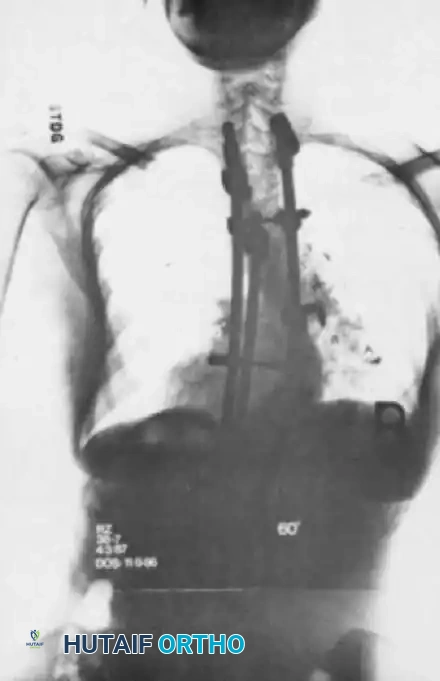
Fig. 41-15 Postoperative AP radiograph demonstrating a long posterior spinal fusion construct utilizing high-density pedicle screw fixation to correct a severe coronal deformity.
Rod contouring is the most critical step in executing the preoperative plan. The rods (typically 5.5mm or 6.0mm Cobalt Chrome or Titanium) must be contoured to the desired sagittal profile, not the patient's current deformed state. Reduction maneuvers include cantilever reduction, rod derotation, and in-situ compression/distraction.
Pelvic Fixation Strategies
When the fusion construct extends to the sacrum, supplemental pelvic fixation is mandatory to protect the S1 screws from catastrophic failure and to promote lumbosacral arthrodesis.

Fig. 41-16 Postoperative lateral radiograph showing restoration of lumbar lordosis and global sagittal balance. Note the robust pelvic fixation utilizing iliac screws extending distal to the sacrum.
Modern techniques primarily utilize:
* Iliac Screws: Placed through the PSIS down the iliac shaft towards the sciatic notch. Requires offset connectors to link to the main rod.
* S2-Alar-Iliac (S2AI) Screws: The current preferred technique. The starting point is midway between the S1 and S2 foramina, crossing the SI joint into the ilium. S2AI screws are in-line with the main lumbar rod, eliminating the need for offset connectors and reducing implant prominence.
Interbody Fusion Techniques
To achieve high fusion rates at the lumbosacral junction and to provide powerful anterior column support and lordosis, interbody fusion is frequently employed at L4-L5 and L5-S1.
* ALIF (Anterior Lumbar Interbody Fusion): Provides the largest footprint for grafting and the most powerful lordotic correction (using hyperlordotic cages).
* TLIF (Transforaminal Lumbar Interbody Fusion): Performed through the posterior approach, allowing for simultaneous interbody work and posterior instrumentation, though it provides less lordotic correction than ALIF.
* LLIF (Lateral Lumbar Interbody Fusion): Excellent for correcting coronal deformity and indirect foraminal decompression, though L5-S1 is typically inaccessible due to the iliac crest.
Postoperative Protocols and Complication Management
Rehabilitation and Follow-up
Postoperatively, patients are typically monitored in the Intensive Care Unit (ICU) for 24-48 hours for hemodynamic monitoring and pain control. Early mobilization is a cornerstone of modern Enhanced Recovery After Surgery (ERAS) protocols. Patients are mobilized with physical therapy on postoperative day 1.
Rigid orthoses (TLSO) are rarely used in modern practice if rigid pedicle screw fixation and adequate bone quality are present, as they restrict respiration and hinder core muscle rehabilitation. Clinical and radiographic follow-up is conducted at 6 weeks, 3 months, 6 months, 1 year, and 2 years to assess for fusion mass consolidation and maintenance of alignment.
Complications: PJK and Pseudarthrosis
Adult spinal deformity surgery carries a high complication profile, approaching 40% in some series.
* Proximal Junctional Kyphosis (PJK): Defined as a kyphotic angle >10 degrees between the Upper Instrumented Vertebra (UIV) and the two vertebrae above it. Risk factors include overcorrection of sagittal balance, poor bone quality, and disruption of the posterior tension band at the UIV. Mitigation strategies include prophylactic vertebroplasty at the UIV/UIV+1, use of transition rods, and meticulous preservation of the supraspinous ligament.
* Pseudarthrosis: Failure of fusion, most commonly occurring at the thoracolumbar junction or lumbosacral pivot point. Presents as recurrent pain, loss of correction, or rod fracture. Prevention relies on meticulous decortication, generous use of autograft and biologics (rhBMP-2), and robust interbody support at the base of the construct.
Meticulous preoperative planning, respect for global sagittal parameters, and rigorous execution of biomechanically sound surgical techniques are imperative to achieving durable, successful outcomes in the complex management of adult idiopathic scoliosis.
📚 Medical References
- adult idiopathic scoliosis: a 20-year follow-up, Thorax 46:474, 1991.
- Pehrsson K, Larsson S, Oden A, et al: Long-term follow-up of patients with untreated scoliosis: a study of mortality, causes of death, and symptoms, Spine 17:191, 1992.
- Perdriolle R, Vidal J: Thoracic idiopathic scoliosis curve evolution and prognosis, Spine 10:785, 1985.
- Picault C, deMauroy JC, Mouilleseaux B: Natural history of idiopathic scoliosis in girls and boys, Spine 11:777, 1986.
- Poitras B, Mayo NE, Goldberg MS, et al: The Ste-Justine adolescent idiopathic scoliosis cohort study. IV. Surgical correction and back pain, Spine 19:1582, 1994.
- Ponseti IV, Friedman B: Prognosis in idiopathic scoliosis, J Bone Joint Surg 32A:381, 1950.
- Renshaw TS: Screening school children for scoliosis, Clin Orthop 229:26, 1988.
- Robin GC, Span Y, Steinberg R, et al: Scoliosis in the elderly: a follow-up study, Spine 7:355, 1982.
- Saunders JO, Little DG, Richard S: Prediction of the crankshaft phenomenon by peak height velocities, Spine 22:1352, 1997.
- Scoles PV, Salvagno R, Villalba K, et al: Relationship of iliac crest maturation to skeletal and chronologic age, J Pediatr Orthop 8:639, 1988.
- Shands AR, Eisberg HBL: The incidence of scoliosis in the state of Delaware: a study of 50,000 minifi lms of the chest made during a survey for tuberculosis, J Bone Joint Surg 37A:1243, 1955.
- Shannon DC, Roseborough EJ, Valenca LM, et al: The distribution of abnormal lung function in kyphoscoliosis, J Bone Joint Surg 52A:131, 1979.
- Shuren N, Kasser JR, Emans JB, et al: Reevaluation of the use of the Risser sign in idiopathic scoliosis, Spine 17:359, 1992.
- Smyrnis T, Antoniou D, Valavanis J, et al: Idiopathic scoliosis: characteristics and epidemiology, Clin Orthop Relat Res 10:921, 1987.
- Sponseller PD, Cohen MS, Nachemson AL, et al: Results of surgical treatment of adults with scoliosis, J Bone Joint Surg 69A:667, 1987.
- Stagnara P: Examen du scoliotique. In Deviations laterales du rachis: scolioses, excyclopedic mediocochirurgicale , vol 7, Paris, 1974, Appareil Locomoteur. Suh PB, MacEwen GD: Idiopathic scoliosis in males: a natural history study, Spine 13:1091, 1988.
- Suk SI, Song HS, Lee CK: Scoliosis induced by anterior and poster rhizotomy, Spine 14:692, 1989.
- Taylor TKF, Ghosh P, Bushnell GR: The contribution of the intervertebral disk to the scoliotic deformity, Clin Orthop Relat Res 156:79, 1981.
- Torell G, Nordwall A, Nachemson A: The changing pattern of scoliosis treatment due to effective screening, J Bone Joint Surg 63A:337, 1981.
- Veraart BEEMJ, Jansen BJ: Changes in lung function associated with idiopathic thoracic scoliosis, Acta Orthop Scand 61:235, 1990.
- Visscher W, Lonstein JE, Hoffman DA, et al: Reproductive outcomes in scoliosis patients, Spine 13:1096, 1988.
- Weinstein SL: Idiopathic scoliosis: natural history, Spine 11:780, 1986.
- Weinstein SL: The natural history of scoliosis in the skeletally mature patient. In Dickson JH, ed: Spinal deformities, vol 1, no. 2. State of the art reviews. Spine, Philadelphia, 1987, Hanley & Belfus. Weinstein SL: Adolescent idiopathic scoliosis: prevalence and natural history, Instr Course Lect 38:115, 1989.
- Weinstein SL, Dolan LA, Spratt KF, et al: Natural history of adolescent idiopathic scoliosis: back pain at 50 years. Paper presented at the annual meeting of the Scoliosis Research Society, New York, Sept 1998.
- Weinstein SL, Ponseti IV: Curve progression in idiopathic scoliosis, J Bone Joint Surg 65A:447, 1983.
- Weinstein SL, Zavala DC, Ponseti IV: Idiopathic scoliosis: longterm follow-up and prognosis in untreated patients, J Bone Joint Surg 63A:702, 1981.
- Willner S: Prospective prevalence study of scoliosis in southern Sweden, Acta Orthop Scand 53:233, 1982.
- Willner S: Prevalence study of trunk asymmetries and structural scoliosis in 10-year-old school children, Spine 9:644, 1984.
- Wynne-Davies R: Familial (idiopathic) scoliosis: a family survey, J Bone Joint Surg 50B:24, 1968.
- Xiong B, Sevastik J, Hedlund R, et al: Sagittal confi guration of the spine and growth of the posterior elements in early scoliosis, J Orthop Res 12:113, 1994.
- Yamauchi Y, Yamaguchi T, Asaka Y: Prediction of curve progression in idiopathic scoliosis based on initial roentgenograms: a proposal of an equation, Spine 13:1258, 1988.
- Yarom R, Blatt J, Gorodetsky R, et al: Microanalysis and x-ray fl uorescence spectrometry of platelets in diseases with elevated muscle calcium, Eur J Clin Invest 10:143, 1980.
- Yarom R, Robin GC: Studies on spinal and peripheral muscles from patients with scoliosis, Spine 4:12, 1979.
- Yekutiel M, Robin GC, Yarom: Proprioceptive function in children with adolescent idiopathic scoliosis, Spine 6:560, 1981.
- Patient Evaluation in Adolescent Idiopathic Scoliosis Aaro S, Dahlborn M: Vertebral rotation: estimation of vertebral rotation and spinal and rib cage deformity in scoliosis by computerized tomography, Spine 6:460, 1981.
- Asher MA: Scoliosis evaluation, Orthop Clin North Am 19:805, 1988.
- Barsanti CM, deBari A, Covino BM: The torsion meter: a critical review, J Pediatr Orthop 10:527, 1990.
- Bernhardt M: Normal spinal anatomy: normal sagittal plane alignment. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, 2nd ed, Philadelphia, 1997, Lippincott-Raven. Bernhardt M, Bridwell KH: Segmental analysis of the sagittal plane alignment of the normal thoracic lumbar spines and thoracolumbar junction, Spine 14:717, 1989.
- Bunnell WP: Vertebral rotation: a simple method of measurement in routine radiographs, Orthop Trans 9:114, 1985.
- Carman DL, Browne RH, Birch JG: Measurement of
You Might Also Like