Adolescent Idiopathic Scoliosis: Comprehensive Evaluation & Surgical Management

Key Takeaway
Adolescent Idiopathic Scoliosis (AIS) is a complex three-dimensional spinal deformity requiring meticulous clinical and radiographic evaluation. Management ranges from observation and bracing to complex surgical correction. This guide details the etiology, natural history, curve progression risk factors, and step-by-step surgical techniques—including posterior spinal fusion and pedicle screw instrumentation—essential for orthopedic residents and practicing spine surgeons to optimize patient outcomes and halt deformity progression.
Introduction to Adolescent Idiopathic Scoliosis
Adolescent Idiopathic Scoliosis (AIS) represents a complex three-dimensional deformity of the spine, characterized by lateral curvature, vertebral rotation, and sagittal plane abnormalities. It is the most common form of pediatric scoliosis, typically presenting in children aged 10 years or older, prior to skeletal maturity. Understanding its intricate etiology, natural history, and meticulous evaluation is paramount for optimal patient management, ranging from observation and bracing to complex surgical intervention.
This comprehensive, evidence-based review is tailored for advanced orthopedic residents, spine fellows, and practicing consultant surgeons preparing for board examinations (FRCS, AAOS) and refining their clinical practice.
Etiology and Pathogenesis
The precise etiology of AIS remains elusive, despite extensive research. The term "idiopathic" underscores this lack of a definitive singular cause. However, current research points towards a multifactorial origin, involving a complex interplay of genetic, biomechanical, neurophysiological, and connective tissue factors.
The hallmark of AIS is a three-dimensional spinal deformity encompassing:
* Lateral curvature: The primary deviation from the sagittal plane.
* Vertebral rotation: Rotation of the vertebral bodies towards the convexity of the curve, often accompanied by rib cage deformity (rib hump).
* Sagittal plane abnormalities: Most idiopathic curves exhibit lordosis or hypokyphosis in the thoracic region, which is considered a significant contributing factor to curve progression and may even be primary to the development of the lateral curve.
Lowe and Peters highlighted several possible causative factors, illustrating their potential interrelationships:
* Genetic Predisposition: A strong hereditary component is widely accepted. Family studies demonstrate a higher incidence among relatives of affected individuals, suggesting polygenic inheritance.
* Neurophysiological Factors: Theories propose a role for abnormal melatonin metabolism, neurotransmitter imbalances affecting spinal muscle tone, and proprioceptive dysfunction leading to abnormal spinal loading.
* Connective Tissue Abnormalities: Subtle defects in collagen or elastin metabolism could affect the mechanical properties of ligaments and intervertebral discs.
* Abnormal Biomechanical Forces: Rapid growth spurts during puberty, coupled with inherent spinal asymmetry, can exacerbate minor deformities via the Hueter-Volkmann principle.
Fig. 1: Possible interrelationships of various factors that have been shown to have a possible role in the cause of idiopathic scoliosis. (From Lowe TG, Edgar M, Margulies JY, et al: Etiology of idiopathic scoliosis: current trends in research).
Clinical Pearl: While the exact cause remains unknown, the consensus points to a hereditary predisposition and a multifactorial etiology. Always take a detailed family history, as the presence of AIS in first-degree relatives significantly increases the risk of curve progression.
Natural History and Curve Progression
A thorough understanding of the natural history and prevalence of AIS is fundamental for determining the necessity and timing of intervention.
Prevalence
The prevalence of AIS varies inversely with the magnitude of the Cobb angle. Smaller curves are more common, with a notable increase in the female-to-male ratio as curve severity increases. Curves >10 degrees have a prevalence of 2-3% (Female:Male ratio of 1.4-2:1), while curves >30 degrees have a prevalence of 0.1-0.3% (Female:Male ratio of 10:1).
Risk Factors for Curve Progression
The likelihood of curve progression is a critical determinant for treatment decisions.
Box 1: Factors Related to Progression of Adolescent Idiopathic Scoliosis.
Key factors strongly correlated with an increased risk of progression include:
* Sex: Girls are significantly more likely to experience curve progression requiring treatment than boys.
* Skeletal Maturity (Risser Sign): The Risser sign assesses the ossification of the iliac crest apophysis. Premenarchal girls or those with a Risser sign of 0-1 have a profoundly higher risk of progression.
Fig. 2: Radiographic evaluation of the Risser sign, demonstrating the progression of ossification along the iliac apophysis.
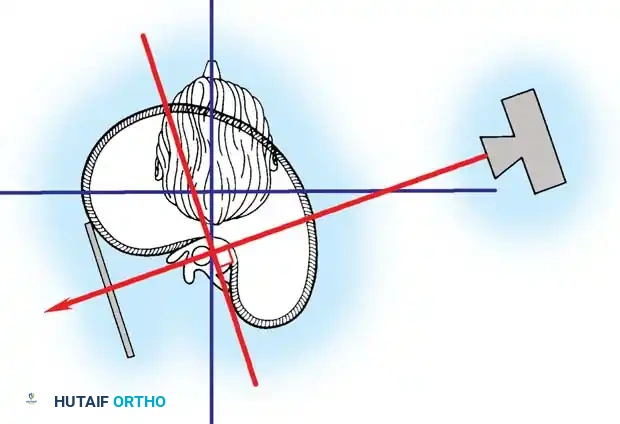
Fig. 3: Additional markers of skeletal maturity, including the status of the proximal humeral and femoral epiphyses.

Fig. 4: Evaluation of the triradiate cartilage. Open triradiate cartilage is a strong predictor of the peak height velocity and impending rapid curve progression.
- Curve Pattern: Double curves tend to be more progressive than single curves. Single thoracic curves are generally more progressive than single lumbar curves.
- Curve Magnitude: The risk of progression increases directly with the initial Cobb angle. A 20-degree curve in a Risser 0 patient has a roughly 20% risk of progression, whereas a 50-degree curve has a >90% risk.
Lonstein and Carlson developed a highly utilized nomogram to predict curve progression at initial presentation, integrating Cobb angle, Risser sign, and chronological age.
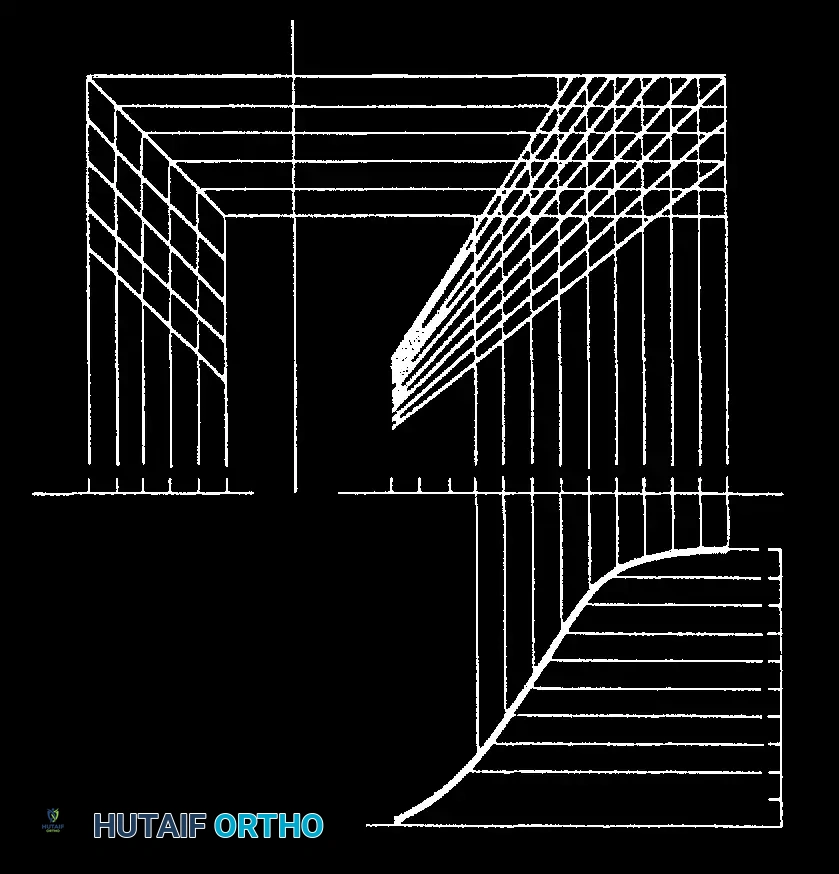
Fig. 5A: Nomogram for prediction of progression of scoliotic curve.
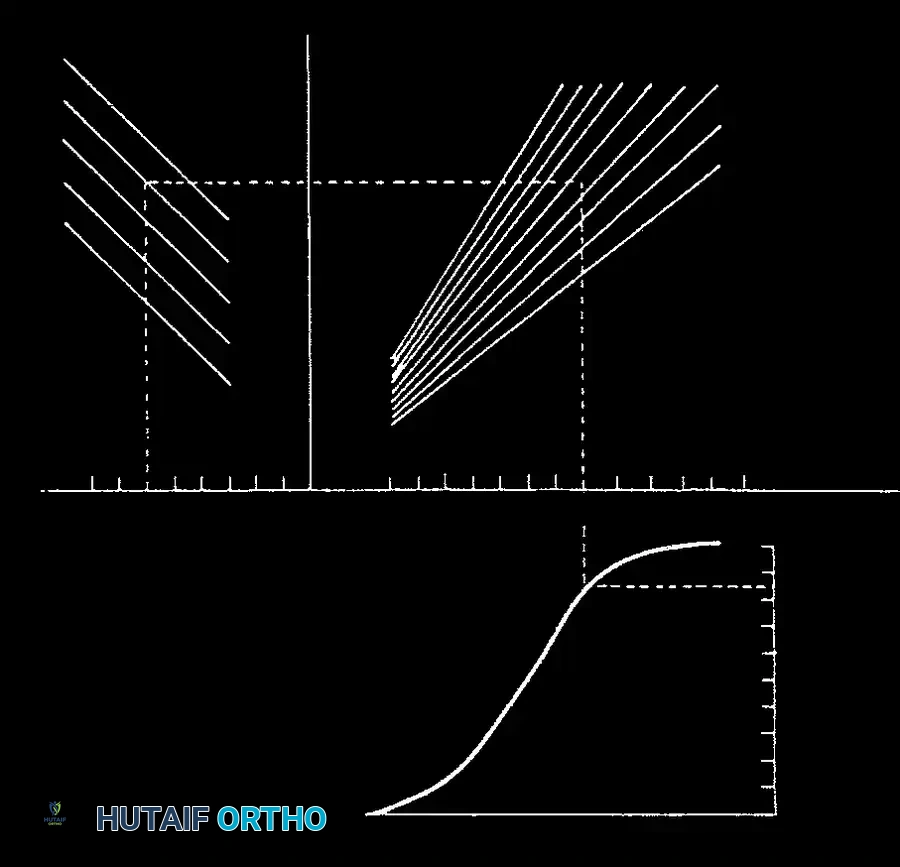
Fig. 5B: Application of the Lonstein and Carlson nomogram for risk stratification.
Long-Term Outcomes in Untreated Adult Scoliosis
Untreated AIS can lead to significant long-term morbidity. Weinstein and Ponseti's landmark studies demonstrated that curves exceeding 50 degrees at skeletal maturity progress at an average rate of 1 degree per year. This can lead to progressive coronal and sagittal imbalance, restrictive pulmonary disease (particularly in thoracic curves >80 degrees), and degenerative back pain.
Comprehensive Clinical Evaluation
The clinical evaluation of a patient with suspected AIS must be systematic and thorough to rule out non-idiopathic causes (e.g., neuromuscular, congenital, or syndromic scoliosis).
Physical Examination
Assessment begins with observing the patient's overall posture, shoulder symmetry, and pelvic tilt.

Fig. 6: Clinical evaluation of global coronal balance and posture.

Fig. 7: Assessment of shoulder height asymmetry, a common cosmetic complaint in thoracic AIS.

Fig. 8: Use of a plumb line dropped from the C7 spinous process to evaluate global coronal decompensation relative to the gluteal cleft.
The Adams Forward Bend Test is the most sensitive clinical screening tool. It highlights the rotational component of the deformity (the rib hump or lumbar prominence).

Fig. 9: The Adams Forward Bend Test demonstrating a right thoracic rib prominence.
The degree of axial rotation is quantified using a Scoliometer. An angle of trunk rotation (ATR) of 5 to 7 degrees correlates with a Cobb angle of approximately 15 to 20 degrees and warrants radiographic evaluation.

Fig. 10: Application of a scoliometer during the forward bend test to measure the Angle of Trunk Rotation (ATR).
Surgical Warning: A meticulous neurological examination is mandatory. Asymmetric abdominal reflexes, hyperreflexia, or cavus foot deformities are red flags for intraspinal anomalies (e.g., syringomyelia, tethered cord, Chiari malformation) and necessitate a total spine MRI prior to any surgical intervention.
Radiographic Evaluation and Classification
Standard radiographic evaluation requires full-length, standing posteroanterior (PA) and lateral radiographs of the spine on a single 36-inch cassette.
Coronal Plane Assessment
The Cobb angle is the gold standard for quantifying the magnitude of the coronal deformity. It is measured by drawing lines parallel to the superior endplate of the most tilted cephalad vertebra and the inferior endplate of the most tilted caudal vertebra.

Fig. 11: Measurement of the Cobb angle on a standing PA radiograph.

Fig. 12: Assessment of coronal balance and the central sacral vertical line (CSVL).

Fig. 13: Measurement of apical vertebral translation from the CSVL.
Vertebral rotation is assessed using the Nash-Moe method, which grades the migration of the pedicles towards the convexity of the curve.

Fig. 14: Nash-Moe grading system for apical vertebral rotation.
Sagittal Plane Assessment
Sagittal balance is equally critical. Thoracic hypokyphosis is a hallmark of AIS. Normal thoracic kyphosis ranges from 20 to 40 degrees, and lumbar lordosis ranges from 40 to 60 degrees.
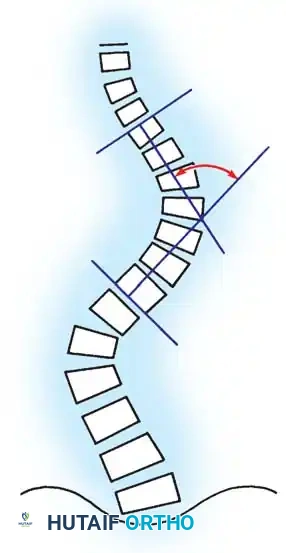
Fig. 15: Evaluation of sagittal alignment, including thoracic kyphosis and lumbar lordosis.
Flexibility Radiographs
To determine curve flexibility and plan surgical fusion levels, dynamic imaging is required. Supine lateral bending films are standard for assessing the structural nature of the curves.
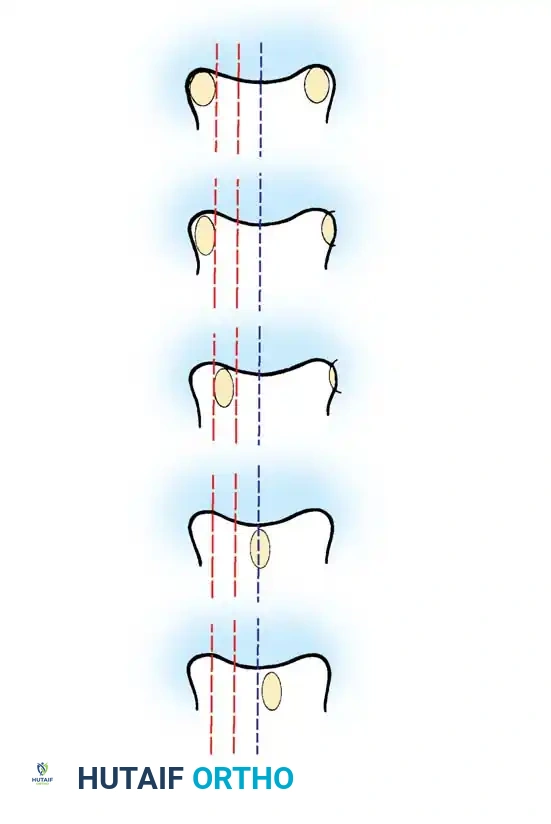
Fig. 16: Supine lateral bending radiographs demonstrating curve flexibility.
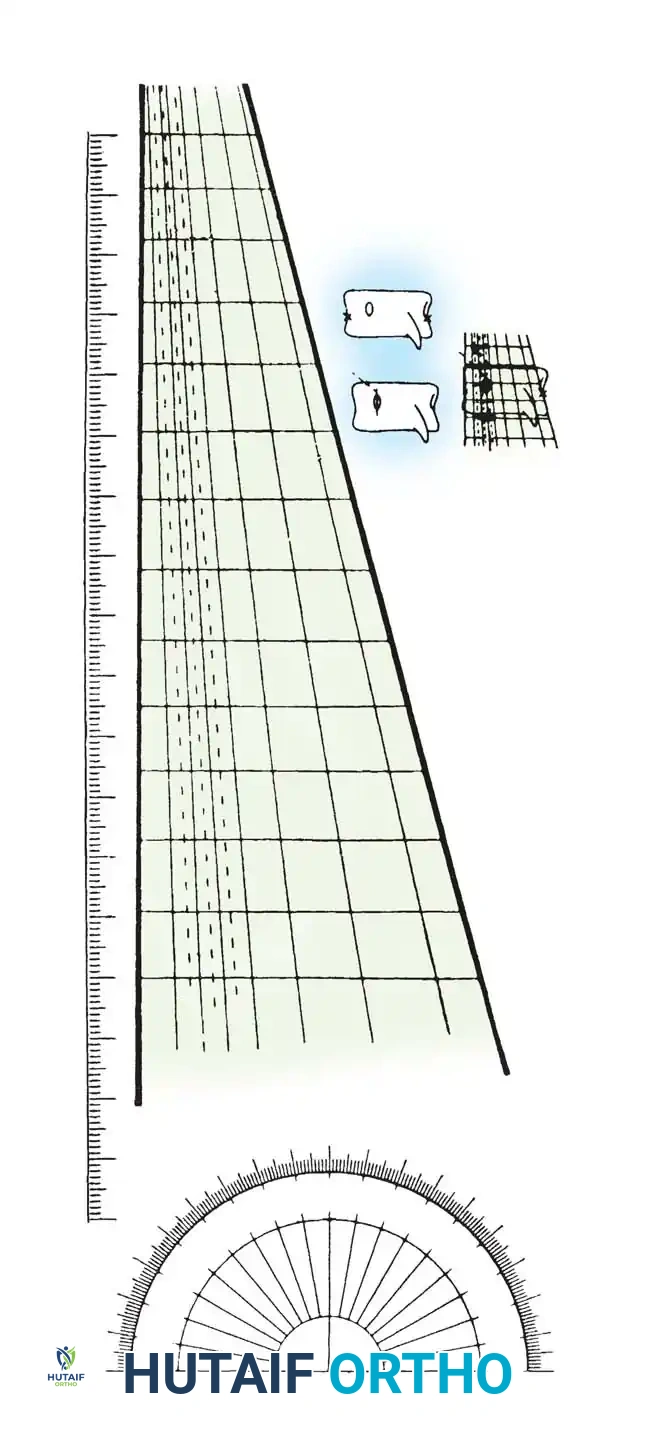
Fig. 17: Push-prone or traction radiographs may be utilized for severe, rigid curves >70 degrees to assess maximum correctability.
The Lenke Classification System
The Lenke classification system is the universal standard for categorizing AIS to guide surgical decision-making. It relies on identifying structural vs. non-structural curves based on bending films (a curve that bends out to <25 degrees is non-structural).
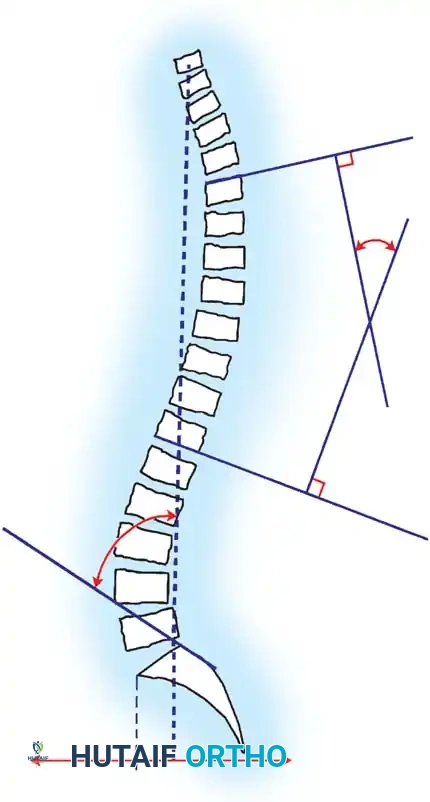
Fig. 18: The six curve types of the Lenke Classification System.
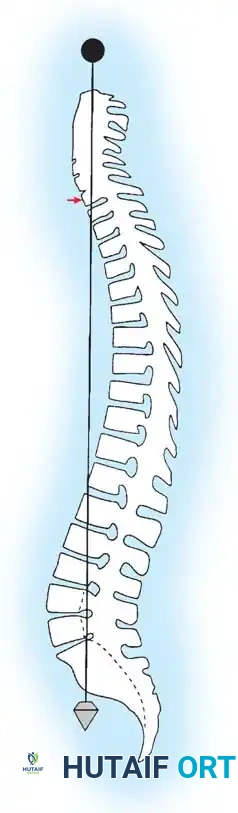
Fig. 19: Lenke lumbar spine modifiers (A, B, C) based on the relationship of the CSVL to the apical lumbar vertebra.
Indications for Treatment
Treatment algorithms are dictated by curve magnitude, skeletal maturity, and documented progression.
1. Observation: Curves <25 degrees in growing children, or <45 degrees in skeletally mature patients.
2. Bracing (TLSO): Indicated for curves between 25 and 45 degrees in skeletally immature patients (Risser 0-2) to halt progression.
3. Surgical Intervention: Indicated for curves >45-50 degrees in growing children, or curves >50 degrees in mature patients, due to the high risk of continued progression into adulthood.
Surgical Management: Posterior Spinal Fusion (PSF)
The primary goals of surgery are to achieve a solid arthrodesis, halt curve progression, safely maximize three-dimensional deformity correction, and restore coronal and sagittal balance. Posterior Spinal Fusion (PSF) with segmental pedicle screw instrumentation is the workhorse procedure for AIS.
Preoperative Planning and Biomechanics
Meticulous preoperative templating is required to select the Upper Instrumented Vertebra (UIV) and Lower Instrumented Vertebra (LIV).

Fig. 20: Preoperative radiographic templating for level selection.
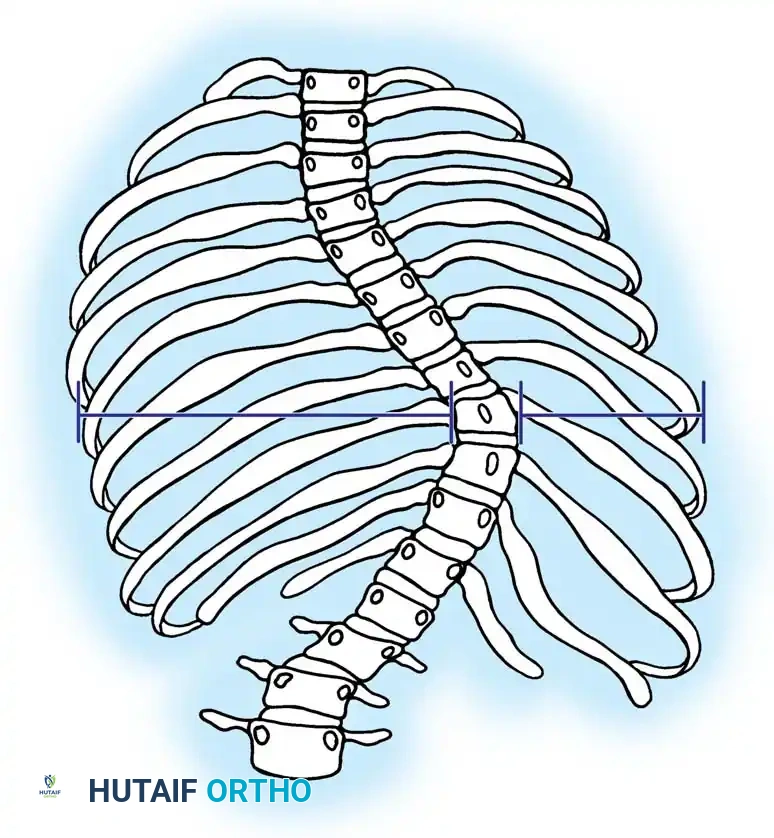
Fig. 21: Detailed assessment of vertebral morphology and pedicle trajectory planning.
- UIV Selection: Must include all structural proximal curves. Stopping short of the stable sagittal vertebra can lead to proximal junctional kyphosis (PJK).
- LIV Selection: The LIV should ideally be the "touched vertebra" (the first vertebra bisected by the CSVL) to ensure a level foundation and prevent distal add-on.
Patient Positioning and Neuromonitoring
- Positioning: The patient is placed prone on a radiolucent Jackson spinal table. The abdomen must hang free to decrease intra-abdominal pressure, thereby reducing epidural venous bleeding.
- Neuromonitoring: Multimodal intraoperative neuromonitoring (IONM) utilizing Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs) is mandatory to detect and prevent iatrogenic spinal cord injury during correction maneuvers.
Surgical Approach and Exposure
- Incision: A midline longitudinal incision is made over the planned fusion levels.
- Dissection: Subperiosteal dissection of the paraspinal musculature is performed bilaterally out to the tips of the transverse processes in the thoracic spine and the facet joints in the lumbar spine.
- Facetectomy: Meticulous bilateral inferior facetectomies (Ponté osteotomies if severe kyphosis/rigidity is present) are performed at every level to increase spinal flexibility and provide a vascularized bed for bone grafting.

Fig. 22: Anatomical landmarks for facetectomy and pedicle entry point identification.
Pedicle Screw Instrumentation
Segmental pedicle screw fixation provides superior biomechanical control, allowing for enhanced three-dimensional correction compared to older hook-and-rod constructs.
- Entry Point: In the thoracic spine, the entry point is typically at the junction of the bisected transverse process and the superior articular facet.
- Preparation: A high-speed burr decorticates the entry point. A pedicle probe (gearshift) is advanced down the cancellous channel of the pedicle into the vertebral body.
- Palpation: A ball-tip probe is used to palpate the five walls of the pedicle tract (medial, lateral, superior, inferior, and anterior) to ensure no cortical breaches.
- Insertion: The tract is tapped, and the appropriate diameter and length pedicle screw is inserted.
Fig. 23: Radiographic confirmation of segmental pedicle screw instrumentation.
Deformity Correction Maneuvers
Once anchors are placed, rods (typically 5.5mm or 6.0mm Cobalt Chrome or Titanium) are contoured to the desired physiological sagittal profile.
Correction techniques include:
* Rod Derotation: The contoured rod is engaged into the screws on the concave side and rotated 90 degrees to convert the scoliotic coronal deformity into normal sagittal kyphosis.
* Direct Vertebral Rotation (DVR): Derotation tubes are attached to the pedicle screws at the apex to actively derotate the vertebral bodies, correcting the rib hump.
* Translation and Compression/Distraction: The spine is translated to the rod. Compression is applied on the convexity and distraction on the concavity to level the vertebrae and correct the coronal curve.
Fig. 24: Biomechanics of rod derotation and direct vertebral translation maneuvers.
Pitfall: Over-distraction on the concavity can stretch the spinal cord, leading to a loss of MEP signals. If signals drop, immediately release distraction, raise mean arterial pressure (MAP > 85 mmHg), and ensure adequate oxygenation.
Arthrodesis and Closure
Achieving a solid fusion is the ultimate goal to prevent hardware failure.
1. Decortication: The lamina, transverse processes, and facet joints are aggressively decorticated using a high-speed burr or gouge.
2
📚 Medical References
- adolescent idiopathic scoliosis curves between 70 degrees and 100 degrees: is anterior release necessary? Spine 30:2061, 2005.
- Maenza RA: Juvenile and adolescent idiopathic scoliosis: magnetic resonance imaging evaluation and clinical indications, J Pediatr Orthop B , 12:295, 2003.
- Mannherz RE, Betz RR, Clancy M, et al: Juvenile idiopathic scoliosis followed to skeletal maturity, Spine 13:1087, 1988.
- Mardjetko SM. Infantile and juvenile scoliosis. In Bridwell KH, DeWald RL, eds: The textbook of spinal surgery, 2nd ed, Philadelphia, 1997, Lippincott-Raven. Mardjetko SM, Hammerberg KW, Lubicky JP, et al: The Luque trolley revisited: review of 9 cases requiring revision, Spine 17:582, 1992.
- Mau H: Etiology of idiopathic scoliosis, Reconstr Surg Traumatol 13:184, 1972.
- McCarthy RE, McCullough FL: Growing instrumentation for scoliosis. Paper presented at the 28th annual meeting of the Scoliosis Research Society, Dublin, Sept 1993.
- McMaster MJ: Infantile idiopathic scoliosis: can it be prevented? J Bone Joint Surg 65B:612, 1983.
- McMaster MJ, Macnicol MF: The management of progressive infantile idiopathic scoliosis, J Bone Joint Surg 61B:36, 1979.
- Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis, J Bone Joint Surg 54B:230, 1972.
- Moe JH, Kharrat K, Winter RB, et al: Harrington instrumentation without fusion plus external orthotic support for the treatment of diffi cult curvature problems in young children, Clin Orthop Relat Res 185:35, 1984.
- Morin MR: Pediatric Cotrel-Dubousset instrumentation system. In Bridwell KH, DeWald RL, eds: Spinal surgery, Philadelphia, 1991, JB Lippincott. Parent S, Labelle H, Skalli W, et al: Thoracic pedicle morphometry in vertebrae from scoliotic spines, Spine 29:239, 2004.
- Patterson JF, Webb JK, Burwell RG: The operative treatment of progressive early onset scoliosis: a preliminary report, Spine 15:809, 1990.
- Pehrsson K, Nachemson A, Olofson J, et al: Respiratory failure in scoliosis and other thoracic deformities, Spine 17:714, 1992.
- Rinsky LA, Gamble JG, Bleck EE: Segmental instrumentation without fusion in children with progressive scoliosis, J Pediatr Orthop 5:687, 1985.
- Roberts S, Menage J, Eisenstein SM: The cartilage end-plate and intervertebral disc in scoliosis: calcifi cation and other sequelae, J Orthop Res 11:747, 1993.
- Sanders JO, Herring JA, Browne RH: Behavior of the immature (Risser 0) spine in idiopathic scoliosis following posterior spinal instrumentation and fusion. Paper presented at the 28th annual meeting of the Scoliosis Research Society, Dublin, Sept 1993.
- Shuffl ebarger HL, Clark CE: Prevention of the crankshaft phenomenon, Spine 16:S409, 1991.
- Thompson SK, Bentley G: Prognosis in infantile idiopathic scoliosis, J Bone Joint Surg 62B:151, 1980.
- Tolo VT, Gillespie R: The characteristics of juvenile idiopathic scoliosis and results of its treatment, J Bone Joint Surg 60B:181, 1978.
- Vanlommel E, Fabry G, Urlus M, et al: Harrington instrumentation without fusion for the treatment of scoliosis in young children, J Pediatr Orthop 11:116, 1992.
- Winter RW: Scoliosis and spinal growth, Orthop Rev 7:17, 1977.
- Wynne-Davies R: Infantile idiopathic scoliosis: causative factors, particularly in the fi rst six months of life, J Bone Joint Surg 57B: 138, 1975.
- Natural History of Aaro S, Ohlund C: Scoliosis and pulmonary function, Spine 9:220, 1984.
- Apter A, Morein G, Munitz H, et al: The psychosocial sequelae of the Milwaukee brace in adolescent girls, Clin Orthop Relat Res 131:156, 1978.
- Arai S, Ohtsuka Y, Moriya H, et al: Scoliosis associated with syringomyelia, Spine 18:1591, 1993.
- Archer IA, Dickson RA: Stature and idiopathic scoliosis: a prospective study, J Bone Joint Surg 67B:185, 1985.
- Ascani E, Bartolozzi P, Logroscino CA, et al: Natural history of untreated idiopathic scoliosis after skeletal maturity, Spine 11:787, 1986.
- Bagnall KM, Raso VJ, Hill DL, et al: Melatonin levels in idiopathic scoliosis: diurnal and nocturnal serum melatonin levels in girls with adolescent idiopathic scoliosis, Spine 21:1974, 1996.
- Beals RK: Nosologic and genetic aspects of scoliosis, Clin Orthop 93:23, 1973.
- Berman AT, Cohen DL, Schwentker EP: The effects of pregnancy on idiopathic scoliosis: a preliminary report on eight cases and review of the literature, Spine 7:76, 1982.
- Betz RR, Bunnell WP, Lambrecht-Mulier E, et al: Scoliosis and pregnancy, J Bone Joint Surg 69A:90,1987.
- Biondi J, Weiner DS, Bethem D, et al: Correlation of Risser sign and bone age determination in adolescent idiopathic scoliosis, J Pediatr Orthop 5:697, 1985.
- Bjerkreim I, Hassan I: Progression in untreated idiopathic scoliosis after end of growth, Acta Orthop Scand 53:897, 1982.
- Bjure J, Nachemson A: Nontreated scoliosis, Clin Orthop Relat Res 93:44, 1973.
- Blount WP, Mellencamp DD: The effect of pregnancy on idiopathic scoliosis, J Bone Joint Surg 62A:1083, 1980.
- Branthwaite MA: Cardiorespiratory consequence of unfused idiopathic scoliosis patients, Br J Dis Chest 80:360, 1986.
- Bremberg S, Nilsson-Berggren B: School screening for adolescent idiopathic scoliosis, J Pediatr Orthop 6:564, 1986.
- Bunnell WP: A study of the natural history of idiopathic scoliosis. Paper presented at the 19th annual meeting of the Scoliosis Research Society, Orlando, Fla, 1984.
- Bunnell WP: The natural history of idiopathic scoliosis before skeletal maturity, Spine 11:773, 1986.
- Bunnell WP: The natural history of idiopathic scoliosis, Clin Orthop Relat Res 229:20, 1988.
- Burwell RG, James JN, Johnson F, et al: The rib hump score: a guide to referral and prognosis? J Bone Joint Surg 64B:248, 1982.
- Burwell RG, James NH, Johnson F, et al: Standardized trunk asymmetry scores: a study of back contours in healthy school children, J Bone Joint Surg 65B:453, 1983.
- Byl NN, Gray JM: Complex balance reactions in different sensory conditions: adolescents with and without idiopathic scoliosis. J Orthop Res 11:215, 1993.
- Bylund P, Jansson E, Dahlberg E, et al: Muscle fi ber types in thoracic erector spinae muscles: fi ber types in idiopathic and other forms of scoliosis, Clin Orthop Relat Res 274:305, 1992.
- Carpintero P, Mesa M, Garcia J, et al: Scoliosis induced by asymmetric lordosis and rotation: an experimental study, Spine 22:2202, 1987.
- Carr AJ, Jefferson RJ, Turner-Smith AR: Family stature in idiopathic scoliosis, Spine 18:20, 1993.
- Carr AJ, Ogilvie DJ, Wordsworth BP, et al: Segregation of structural collagen genes in adolescent idiopathic scoliosis, Clin Orthop Relat Res 247:305, 1992.
- Clayson D, Luz-Alterman S, Cataletto MM, et al: Long-term psychological sequelae of surgically versus nonsurgically treated scoliosis, Spine 12:983, 1987.
- Collis DK, Ponseti IV: Long-term follow-up of patients with idiopathic scoliosis, J Bone Joint Surg 51A:425, 1969.
- Cowell HR, Hall JN, MacEwen GD: Genetic aspects of idiopathic scoliosis, Clin Orthop 86:121, 1972.
- Cruickshank JL, Koike M, Dickson RA: Curve patterns in idiopathic scoliosis , J Bone Joint Surg 71B:259, 1989.
- Cummings RJ, Loveless EA, Campbell J, et al: Interobserver reliability and intraobserver reproducibility of the system of King et al. for the classifi cation of adolescent idiopathic scoliosis, J Bone Joint Surg 81A:743, 1999.
- Czeizel A, Bellyei A, Barta O, et al: Genetics of adolescent idiopathic scoliosis, J Med Genet 15:424, 1978.
- Davids JR, Chamberlin E, Blackhurst DW: Indications for magnetic resonance imaging in presumed adolescent idiopathic scoliosis, J Bone Joint Surg 86A:2187, 2004.
- Davies G, Reid L: Effect of scoliosis on growth of alveoli and pulmonary arteries and on right ventricle, Arch Dis Child 46:623, 1971.
- Deacon P, Archer IA, Dickson RA: The anatomy of spinal deformity: a biomechanical analysis, Orthopedics 10:897, 1987.
- Deacon P, Flood BM, Dickson RA: Idiopathic scoliosis in three dimensions: a radiographic and morphometric analysis, J Bone Joint Surg 66B:509, 1984.
- DeGeorge FV, Fisher RL: Idiopathic scoliosis: genetic and environmental aspects, J Med Genet 4:251, 1967.
- Dickson RA: Scoliosis in the community, Br Med J 286:615, 1983.
- Dickson RA: The etiology and pathogenesis of idiopathic scoliosis, Acta Orthop Belg 58(suppl):21, 1992.
- Dickson R, Deacon P: Spinal growth, J Bone Joint Surg 69B:690, 1987.
- Dickson RA, Lawton JO, Archer IA, et al: The pathogenesis of idiopathic scoliosis: biplanar spinal asymmetry, J Bone Joint Surg 66B:8, 1984.
- Dickson JH, Mirkovic S, Noble MS, et al: Results of operative treatment of idiopathic scoliosis in adults, J Bone Joint Surg 77A:513, 1995.
- Dickson RA, Stamper P, Sharp AM, et al: School screening for scoliosis: cohort study of clinical course, Br Med J 281:265, 1980.
- Dobbs MB, Lenke LG, Szymanski DA, et al: Prevalence of neural axis abnormalities in patients with infantile idiopathic scoliosis, J Bone Joint Surg 84A:2230, 2002.
- Dobbs MB, Lenke LG, Walton T, et al: Can we predict the ultimate lumbar curve in adolescent idiopathic scoliosis patients undergoing a selective fusion with undercorrection of the thoracic curve? Spine 29:277, 2004.
- Dubousset J, Machida M: Melatonin: a possible role in the pathogenesis of human idiopathic scoliosis (abstract 3.19). In Proceedings of the Tenth International Philip Zorab Symposium on Scoliosis, Oxford, 1998, Oxford University Press. Duval-Beaupere G: Rib hump and supine angle as prognostic factors for mild scoliosis, Spine 17:103, 1992.
- Duval-Beaupere G, Lamireau TH: Scoliosis of less than 30 degrees: properties of the evolutivity (risk of progression), Spine 10:421, 1985.
- Echenne B, Barneon G, Pages M, et al: Skin elastic fi ber pathology and idiopathic scoliosis, J Pediatr Orthop 8:522, 1988.
- Edgar MA: The natural history of unfused scoliosis, Clin Orthop 10:931, 1987.
- Edgar MA, Mehta M: Long-term follow-up of fused and unfused idiopathic scoliosis, J Bone Joint Surg 70B:712:1988.
- Eliason JM, Richman LC: Psychological effects of idiopathic adolescent scoliosis, Dev Behav Pediatr 5:169, 1984.
- Fallstrom K, Nachemson AL, Cochran TP: Psychologic effect of treatment for adolescent idiopathic scoliosis, Orthop Trans 8:150, 1984.
- Ford DM, Bagnall KM, Clements CA, et al: Muscle spindles in the paraspinal musculature of patients with adolescent idiopathic scoliosis, Spine 13:461, 1988.
- Gazioglu K, Goldstein LA, Femi-Pearse D, et al: Pulmonary function in idiopathic scoliosis: comparative evaluation before and after orthopaedic correction, J Bone Joint Surg 50A:1391, 1968.
- Gibson JN, McMaster MJ, Scrimgeour CM, et al: Rates of muscle protein synthesis in paraspinal muscles: literal disparity in children with idiopathic scoliosis, Clin Sci 75:79, 1988.
- Goldberg CJ, Dowling FE, Fogarty EE: Adolescent idiopathic scoliosis—early menarche, normal growth, Spine 18:529, 1993.
- Goldberg MS, Mayo NE, Poitras B, et al: The Ste-Justine adolescent idiopathic scoliosis cohort study. II. Perception of health, self, and body image and participation in physical activities, Spine 19:1562, 1994.
- Hadley-Miller N, Mims B, Milewicz DM: The potential role of the elastic fi ber system in adolescent idiopathic scoliosis, J Bone Joint Surg 76A:1193, 1994.
- Hamanishi C, Tanaka S, Kasahara Y, et al: Progressive scoliosis associated with lateral gaze palsy, Spine 18:2545, 1993.
- Harrington PR: The etiology of idiopathic scoliosis, Clin Orthop 126:17, 1977.
- Hassan I, Bjerkreim I: Progression in idiopathic scoliosis after conservative treatment, Acta Orthop Scand 54:88, 1983.
- Henderson MH, Rieger MA, Miller F, et al: Infl uence of parental age on degree of curvature in idiopathic scoliosis, J Bone Joint Surg 72A:910, 1990.
- Herman R, Mixon J, Fisher A, et al: Idiopathic scoliosis and the central nervous system: a motor control problem, Spine 10:1, 1985.
- Howell FR, Mahood JK, Dickson RA: Growth beyond skeletal maturity, Spine 17:437, 1992.
- Jackson RP, McManus AC: Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective, controlled clinical study, Spine 19:611, 1994.
- James JIP: Idiopathic scoliosis: the prognosis, diagnosis, and operative indications related to curve pattern and age at onset, J Bone Joint Surg 36B:36, 1954.
- Keessen W, Crowe A, Hearn M: Proprioceptive accuracy in idiopathic scoliosis, Spine 17:149, 1992.
- Kesling KL, Reinker KA: Scoliosis in twins: a meta-analysis of the literature and report of six cases, Spine 22:2009, 1997.
- Kindsfater K, Lowe T, Lawellin D, et al: Levels of platelet calmodulin for the prediction of progression and severity of adolescent idiopathic scoliosis, J Bone Joint Surg 76A:1186, 1994.
- Kolind-Sörensen V: A follow-up study of patients with idiopathic scoliosis, Acta Orthop Scand 44:98, 1973.
- Kostuik JP, Bentivoglio J: The incidence of low-back pain in adult scoliosis, Spine 6:268, 1981.
- Lenke LG, Betz RR, Bridwell KH, et al: Intraobserver and interobserver reliability of the classifi cation of thoracic adolescent idiopathic scoliosis, J Bone Joint Surg 80A:1097, 1998.
- Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls, J Bone Joint Surg 82A:685, 2000.
- Little DG, Sussman MD: The Risser sign: a critical analysis, J Pediatr Orthop 14:569, 1994.
- Lonstein JE: Natural history and school screening for scoliosis, Orthop Clin North Am 19:227, 1988.
- Lonstein JE, Bjorklund S, Wanninger MH, et al: Voluntary school screening for scoliosis in Minnesota, J Bone Joint Surg 64A:481, 1982.
- Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth, J Bone Joint Surg 66A:1061, 1984.
- Low WD, Chew EC, Kung LS, et al: Ultrastructures of nerve fi bers and muscle spindles in adolescent idiopathic scoliosis, Clin Orthop Relat Res 174:217, 1983.
- Machida M, Dubousset J, Imamura Y, et al: Pathogenesis of idiopathic scoliosis: SEPs in chicken with experimentally induced scoliosis and in patients with idiopathic scoliosis, J Pediatr Orthop 14:329, 1994.
- Maguire J, Madigan R, Wallace S, et al: Intraoperative longlatency refl ex activity in idiopathic scoliosis demonstrates abnormal central processing: a possible cause for idiopathic scoliosis, Spine 18:1621, 1993.
- Makley JT, Herndon CH, Inkley S, et al: Pulmonary function in paralytic and nonparalytic scoliosis before and after treatment: a study of sixty-three cases, J Bone Joint Surg 50A:1379, 1968.
- Mankin HJ, Graham JJ, Schack J: Cardiopulmonary function in mild and moderate idiopathic scoliosis, J Bone Joint Surg 46A:53, 1964.
- Mayo NE, Goldberg MS, Poitras B, et al: The Ste-Justine adolescent idiopathic scoliosis cohort study. III. Back pain, Spine 19:1573, 1994.
- McInnes E, Hill DL, Raso VJ, et al: Vibratory response in adolescents who have idiopathic scoliosis, J Bone Joint Surg 73A:1208, 1991.
- Miller NH, Mims B, Child A, et al: Genetic analysis of structural elastic fi ber and collagen genes in familial adolescent idiopathic scoliosis, J Orthop Res 14:994, 1996.
- Montgomery F, Willner S: A natural history of idiopathic scoliosis: a study of the incidence of treatment, Spine 13:401, 1988.
- Muhlrad A, Yarom R: Contractile protein on platelets from patients with idiopathic scoliosis, Haemostasis 11:154, 1982.
- Muirhead A, Conner AN: The assessment of lung function in children with scoliosis, J Bone Joint Surg 67B:699, 1985.
- Nachemson A: A long-term follow-up study of nontreated scoliosis, Acta Orthop Scand 39:466, 1968.
- Nachemson A: A long-term follow-up study of nontreated scoliosis, J Bone Joint Surg 50A:203, 1969.
- Nachemson A: Adult scoliosis and back pain, Spine 4:513, 1979.
- Nash CL Jr, Lorig RA, Schatzinger LA, et al: Spinal cord monitoring during operative treatment of the spine, Clin Orthop 126:100, 1977.
- Nathan SW: Body image of scoliotic female adolescents before and after surgery, Matern Child Nurs J 6:139, 1977.
- Nilsonne U, Lundgren KD: Long-term prognosis in idiopathic scoliosis, Acta Orthop Scand 39:456, 1968.
- O’Beirne J, Goldberg C, Dowling FE, et al: Equilibrial dysfunction in scoliosis—cause or effect? J Spinal Disord 2:184, 1989.
- Oegema TR Jr, Bradford DS, Cooper KM, et al: Comparison of biochemistry of proteoglycans isolated from normal, idiopathic scoliotic and cerebral palsy spine, Spine 8:378, 1983.
- Ogilvie JW, Schendel MJ: Calculated thoracic volume as related to parameters of scoliosis correction, Spine 13:39, 1988.
- Pedrini VA, Ponseti IV, Dohrman SC: Glycosaminoglycans of intervertebral disc in idiopathic scoliosis, J Lab Clin Med 82:938, 1973.
- Pehrsson K, Bake B, Larsson S, et al: Lung function in
You Might Also Like


