Shoulder Osteoarthritis: Epidemiology, Surgical Anatomy, and Biomechanics

Key Takeaway
Shoulder osteoarthritis (OA) is a chronic degenerative condition affecting glenohumeral and AC joints, with increasing prevalence with age. Key anatomical considerations for management involve understanding GH joint surfaces, labrum, rotator cuff, and critical neurovascular structures like the axillary nerve.
Introduction & Epidemiology
Shoulder osteoarthritis (OA) represents a chronic degenerative joint disease characterized by progressive articular cartilage loss, subchondral bone remodeling, osteophyte formation, and synovitis. While the inciting etiology can be multifactorial, primary glenohumeral (GH) OA is largely idiopathic, with secondary forms arising from post-traumatic conditions, inflammatory arthropathies (e.g., rheumatoid arthritis), avascular necrosis, or rotator cuff arthropathy. The acromioclavicular (AC) joint is also a frequent site of osteoarthritic changes, often in isolation or concomitant with GH pathology.
Epidemiologically, GH OA prevalence increases with age, affecting approximately 20-30% of individuals over 60, though only a subset develops symptomatic disease requiring intervention. AC joint OA is even more common, with radiographic evidence in up to 50% of adults over 50. Symptomatic presentation typically involves progressive pain, stiffness, and functional limitation, significantly impacting activities of daily living (ADLs) and quality of life. The progression from initial arthritic degeneration, which may be asymptomatic for months or years, to debilitating symptoms underscores the importance of early recognition and stratification of disease severity for appropriate management. Non-operative modalities are the mainstay for early and moderate disease, but for advanced, refractory cases, surgical intervention, primarily arthroplasty, offers reliable pain relief and functional restoration.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the shoulder complex is paramount for safe and effective surgical management of shoulder OA.
Glenohumeral Joint
The glenohumeral joint is a multiaxial diarthrodial joint, characterized by its inherent instability and vast range of motion.
-
Articular Surfaces:
- Humeral Head: Approximately one-third of a sphere, covered by articular cartilage. Its retroversion averages 30-40 degrees relative to the elbow axis, and inclination is typically 130-145 degrees.
- Glenoid Fossa: A shallow, pear-shaped articular surface on the lateral aspect of the scapula, covered by hyaline cartilage. It is significantly smaller than the humeral head (approximately 25% contact area), contributing to its mobility. Glenoid version (retroversion/anteversion) and inclination are critical surgical considerations, particularly in arthroplasty, with an average of 0-10 degrees of retroversion and 5 degrees of superior inclination. Glenoid erosion patterns (e.g., Walch classification for posterior erosion) directly influence implant choice and surgical technique.
- Glenoid Labrum: A fibrocartilaginous rim that deepens the glenoid fossa and serves as an attachment site for the glenohumeral ligaments and biceps tendon. While crucial for stability, it is often degenerated or detached in advanced OA.
- Capsule and Ligamentous Structures: The fibrous capsule is redundant inferiorly to permit full abduction. The primary static stabilizers are the glenohumeral ligaments (SGHL, MGHL, IGHL complex). The inferior glenohumeral ligament (IGHL) complex, with its anterior and posterior bands and intervening axillary pouch, is the primary restraint to anterior and posterior translation at 90 degrees of abduction. These structures are often contracted or scarred in OA, necessitating release during arthroplasty.
-
Rotator Cuff Muscles:
The dynamic stabilizers of the GH joint:
- Supraspinatus: Originates from the supraspinous fossa, inserts on the superior facet of the greater tuberosity. Initiates abduction.
- Infraspinatus: Originates from the infraspinous fossa, inserts on the middle facet of the greater tuberosity. External rotation.
- Teres Minor: Originates from the lateral border of the scapula, inserts on the inferior facet of the greater tuberosity. External rotation.
-
Subscapularis:
Originates from the subscapular fossa, inserts on the lesser tuberosity. Internal rotation.
These muscles depress and center the humeral head within the glenoid, opposing the superior pull of the deltoid. Rotator cuff integrity is a fundamental determinant in arthroplasty selection (TSA vs. rTSA).
- Deltoid Muscle: The primary abductor of the shoulder, comprising anterior, middle, and posterior heads. Innervated by the axillary nerve. Deltoid function is critical post-arthroplasty, especially for rTSA.
-
Neurovascular Structures:
- Axillary Nerve: Courses inferior to the GH joint capsule, wrapping around the surgical neck of the humerus, approximately 5-7 cm distal to the acromial edge. Supplies the deltoid and teres minor. Vulnerable during inferior capsular release, humeral osteotomy, and component insertion.
- Musculocutaneous Nerve: Pierces the coracobrachialis, supplies biceps and coracobrachialis.
- Radial Nerve: Lies posterior to the humerus, generally not at risk anteriorly.
- Suprascapular Nerve: Courses through the suprascapular notch, supplies supraspinatus and infraspinatus. Can be vulnerable during posterior glenoid exposure or excessive superior retraction.
- Posterior Humeral Circumflex Artery: Accompanies the axillary nerve.
Acromioclavicular (AC) Joint
The AC joint is a small diarthrodial joint with a fibrocartilaginous meniscus, connecting the distal clavicle to the acromion.
- Articular Surfaces: Distal clavicle and medial aspect of the acromion.
- Capsule and Ligaments: A relatively weak capsule is reinforced by the superior and inferior AC ligaments. The primary stabilizers are the coracoclavicular (CC) ligaments (trapezoid and conoid), which span from the coracoid process to the clavicle, providing vertical stability.
- Musculature: The deltoid and trapezius muscles have attachments directly over the AC joint, which must be split or released during open surgical approaches.
Scapulothoracic Articulation
While not a true synovial joint, the scapulothoracic articulation is crucial for overall shoulder function, providing a stable base for GH movement and contributing significantly to full range of motion. Scapular dyskinesis can impact post-operative outcomes.
Biomechanics of Arthroplasty
- Total Shoulder Arthroplasty (TSA): Aims to restore normal anatomy and kinematics, relying on an intact rotator cuff to center the humeral head on the glenoid. Relies on concentric rotation.
- Reverse Total Shoulder Arthroplasty (rTSA): Medializes and distalizes the center of rotation of the GH joint. This allows the deltoid to function more efficiently as an abductor by increasing its lever arm and tensioning the muscle, bypassing the need for a functional rotator cuff. This altered biomechanics inherently imposes increased stress on the glenoid fixation.
Indications & Contraindications
The decision for operative versus non-operative management of shoulder OA is guided by a confluence of factors, including disease severity, patient symptoms, functional limitations, radiographic findings, and patient comorbidities and expectations.
Non-Operative Indications
Non-operative management is the initial approach for most patients with shoulder OA, particularly those with mild to moderate symptoms, or those with significant surgical contraindications.
- Early/Mild Disease: Minimal pain, preserved range of motion, and mild radiographic changes.
- Failed Conservative Therapy: Patients who have not exhausted a minimum of 3-6 months of structured non-operative treatment should generally not proceed to surgery.
- Patient Preference: Patients unwilling or hesitant to undergo surgery.
- High Surgical Risk: Significant uncontrolled medical comorbidities (e.g., severe cardiac disease, poorly controlled diabetes, active smoking).
- Lack of Functional Impairment: Despite radiographic evidence, patients who maintain good function and minimal pain do not require surgery.
- AC Joint OA: Typically managed with activity modification, NSAIDs, and corticosteroid injections initially.
Operative Indications
Surgical intervention is generally reserved for patients with persistent, debilitating symptoms refractory to adequate non-operative management, or those with severe disease and impending functional loss.
- Intractable Pain: Severe, chronic shoulder pain (often with significant night pain disrupting sleep) unresponsive to comprehensive non-operative modalities.
- Significant Functional Impairment: Inability to perform ADLs due to pain and stiffness (e.g., dressing, overhead activities, personal hygiene).
- Progressive Loss of Motion: Significant and progressive limitation in active and passive range of motion.
-
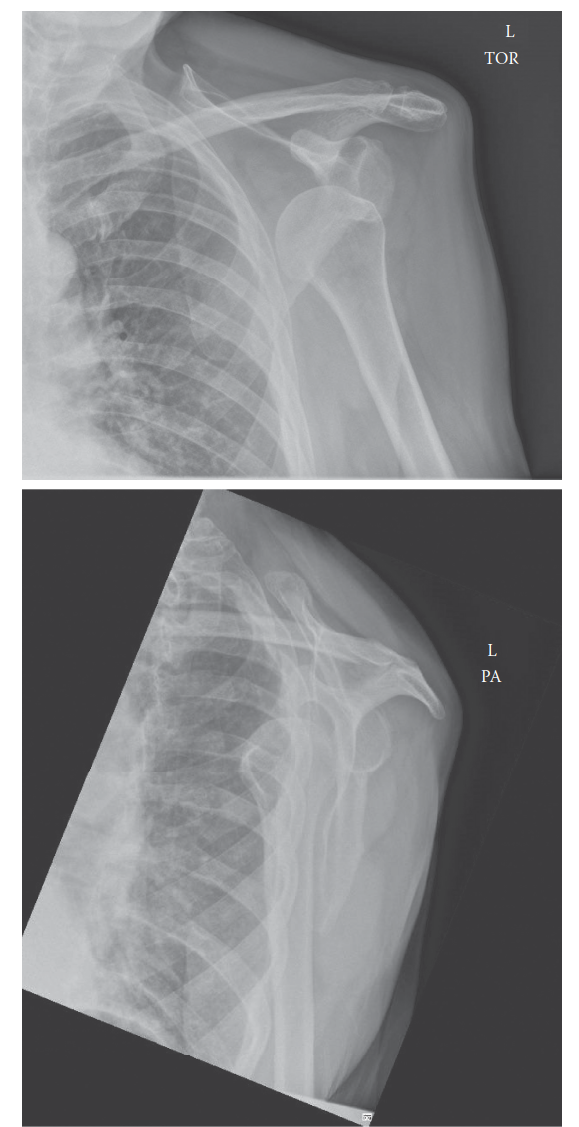
Radiographic Evidence of Advanced Arthropathy:
- GH Joint: Joint space narrowing, osteophyte formation, subchondral sclerosis, cyst formation, and deformity of the humeral head or glenoid. Walch classifications (A1, A2, B1, B2, C) are crucial for glenoid morphology.
- AC Joint: Joint space narrowing, osteophytes, subchondral cysts.
- Rotator Cuff Arthropathy: Glenohumeral OA with concomitant massive, irreparable rotator cuff tear, often with superior migration of the humeral head (pseudoparalysis). This is a specific indication for rTSA.
- Post-Traumatic Arthritis: Often presents with significant pain and stiffness following fractures or dislocations.
- Avascular Necrosis (AVN): Especially late-stage AVN with collapse of the humeral head, often requiring hemiarthroplasty or TSA.
Contraindications
Absolute contraindications are rare but important to identify. Relative contraindications require careful risk-benefit assessment.
-
Absolute Contraindications:
- Active Infection: Current or recent shoulder joint infection (septic arthritis). Must be eradicated prior to arthroplasty.
- Deltoid Dysfunction: Irreparable axillary nerve palsy or complete deltoid paralysis renders rTSA ineffective.
- Irreparable Brachial Plexus Injury: Significant neurological deficits preventing functional use of the limb.
- Uncontrolled Medical Comorbidities: Conditions precluding safe anesthesia and surgical recovery (e.g., recent MI, unstable angina, severe pulmonary dysfunction).
-
Relative Contraindications:
- Smoking: Significantly increases complication rates (infection, wound healing, loosening). Requires cessation pre-operatively.
- Obesity: Increased risk of infection, wound complications, and technical difficulties.
- Uncontrolled Diabetes Mellitus: High HbA1c (e.g., >8%) increases infection risk. Requires glycemic control.
- Prior Shoulder Arthrodesis: Makes arthroplasty technically challenging with limited functional improvement.
- Neurogenic Arthropathy (Charcot Joint): High risk of component loosening.
- Non-compliance: Inability or unwillingness to adhere to post-operative rehabilitation protocols.
Table of Operative vs. Non-Operative Indications for Shoulder OA
| Feature | Non-Operative Management | Operative Management (TSA/Hemi/rTSA) | Operative Management (AC Joint Resection) |
|---|---|---|---|
| Disease Severity | Mild to Moderate OA | Advanced, End-Stage OA (GH Joint) | Symptomatic AC Joint OA refractory to non-operative measures |
| Symptoms | Intermittent pain, mild stiffness, tolerable function | Debilitating chronic pain, significant night pain, pseudoparalysis | Localized superior shoulder pain, pain with cross-body adduction |
| Functional Limitation | Minimal impact on ADLs | Significant impairment of ADLs (dressing, hygiene, overhead reach) | Pain with specific movements (e.g., lifting, reaching across body) |
| Response to Rx | Responsive to NSAIDs, PT, injections | Failure of 3-6 months of comprehensive non-operative therapy | Failure of NSAIDs, PT, steroid injections |
| Radiographic Findings | Mild joint space narrowing, early osteophytes | Severe joint space narrowing, subchondral sclerosis/cysts, deformity, superior migration (rTSA) | Joint space narrowing, osteophytes, geodes at AC joint |
| Rotator Cuff Status | Intact or minor partial tears | Intact/repairable (TSA), irreparable massive tear/arthropathy (rTSA) | N/A (AC joint pathology) |
| Patient Factors | High surgical risk, patient preference, non-compliance | Good health, motivated, compliant with rehab, realistic expectations | Patient preference, absence of other confounding shoulder pathology |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing surgical outcomes and minimizing complications in shoulder arthroplasty.
Pre-Operative Planning
-
Clinical Assessment:
- Thorough history regarding pain characteristics (location, quality, aggravating/alleviating factors, night pain), functional limitations, and prior treatments.
- Physical examination: Range of motion (active and passive), strength of rotator cuff and deltoid, stability, neurovascular status. Specific tests for AC joint (cross-body adduction) and rotator cuff pathology.
-
Imaging Studies:
- Plain Radiographs: Standard series includes true AP (Grashey), axillary lateral, and scapular Y views. Crucial for assessing joint space narrowing, osteophyte formation, subchondral cyst formation, humeral head collapse, glenoid erosion patterns (Walch classification A1, A2, B1, B2, C), and superior humeral head migration (in rotator cuff arthropathy).
- Computed Tomography (CT) Scan: The gold standard for detailed assessment of glenoid bone stock, version (retroversion/anteversion), and inclination. Essential for templating glenoid component size and position, especially in cases of significant posterior erosion (B2, C glenoids). Can also assess humeral head bone loss and morphology. 3D reconstructions are highly valuable.
- Magnetic Resonance Imaging (MRI): Primarily for assessing rotator cuff integrity, labral pathology, and soft tissue quality. While less critical for primary GH OA with intact cuff (where CT is paramount for bone assessment), it is indispensable when rotator cuff arthropathy is suspected or for distinguishing between TSA and rTSA indications. For AC joint OA, MRI can differentiate inflammatory conditions from degenerative changes.
-
Templating:
- Utilizing radiographs and CT scans, specific implant systems are templated to determine optimal humeral head size, glenoid component size and position, and humeral stem length and diameter.
- For TSA: Goals include restoring humeral head retroversion, inclination, and joint line.
- For rTSA: Goals include appropriate glenosphere size and position, baseplate fixation, humeral tray neck-shaft angle, and lateralization/distalization to optimize deltoid tension and impingement-free range of motion.
- Medical Optimization: Comprehensive medical evaluation to identify and manage comorbidities. Smoking cessation, glycemic control in diabetics, and optimization of cardiovascular/pulmonary status are paramount. Pre-operative physiotherapy can improve muscle conditioning and education on post-operative protocols.
- Informed Consent: Detailed discussion with the patient regarding the chosen procedure, expected outcomes, potential complications, and alternative treatments.
Patient Positioning
Two primary positions are utilized for shoulder arthroplasty: the beach chair position and the lateral decubitus position. The choice is often surgeon preference, influenced by the specific procedure and patient factors. AC joint resections can also be performed in either.
-
Beach Chair Position:
- Setup: Patient is semi-recumbent (30-70 degrees elevation), similar to sitting in a beach chair. The head is secured in a well-padded headrest, angled away from the operative shoulder. The torso is secured to the table.
-
Advantages:
- Excellent anatomical orientation, similar to upright examination.
- Familiar for many orthopedic surgeons.
- Allows for easy conversion to an open procedure if started arthroscopically (e.g., AC joint arthroscopy).
- Reduced risk of axillary nerve stretch.
-
Disadvantages:
- Risk of cerebral hypoperfusion (hypotension, cerebral desaturation). Anesthesia must closely monitor blood pressure and consider cerebral oximetry.
- Potential for nerve palsies (brachial plexus stretch if arm traction is excessive, ulnar nerve compression at the elbow).
- Difficulty with inferior glenoid exposure in rTSA due to gravitational pull on the arm.
- Key points: Adequate padding of all pressure points (sacrum, heels, elbows). Ensure head is neutral, and neck is not excessively extended or flexed. A beanbag can help stabilize the torso. The operative arm is draped free in a sterile stockinette.
-
Lateral Decubitus Position:
- Setup: Patient is placed on their non-operative side, secured with a beanbag or bolsters. The operative arm is placed in a traction device, allowing for controlled manipulation and distraction.
-
Advantages:
- Enhanced access to the posterior glenoid and inferior capsule.
- Gravitational assistance for retraction.
- Improved visualization of glenoid in rTSA, especially for inferior baseplate screw placement.
- Lower risk of cerebral hypoperfusion compared to beach chair.
-
Disadvantages:
- Potential for brachial plexus injury from excessive traction.
- Difficult to assess anatomical landmarks in this orientation for some surgeons.
- Risk of pressure sores on the dependent side.
- Positioning takes longer.
- Key points: Axillary roll placed in the axilla of the dependent arm to prevent brachial plexus compression. Ensure stable torso and head support. Avoid excessive traction (limit weight to 10-15 lbs for short periods).
Regardless of position, a sterile field is established, typically from the chin to the iliac crest on the operative side, and circumferentially around the entire arm. The arm is often prepped and draped free in a sterile stockinette, allowing for full range of motion intraoperatively.
Detailed Surgical Approach / Technique
This section will detail the principles of total shoulder arthroplasty (TSA) via the deltopectoral approach, which is the cornerstone for most GH arthroplasties. Adaptations for reverse TSA and a brief overview of distal clavicle excision for AC joint OA will also be provided.
Deltopectoral Approach (for TSA and Hemiarthroplasty)
This is the workhorse approach for most anterior shoulder procedures, including primary and revision shoulder arthroplasty.
- Incision: A curvilinear incision approximately 8-10 cm in length, extending from the anteromedial aspect of the acromion inferiorly along the deltopectoral groove towards the coracoid process, then continuing slightly distally. The incision should allow for adequate exposure of the humeral head and glenoid without excessive skin tension.
-
Dissection of the Deltopectoral Interval:
- Identify the deltopectoral groove, marked by the cephalic vein. This internervous plane separates the deltoid (axillary nerve innervation) laterally from the pectoralis major (medial and lateral pectoral nerve innervation) medially.
- The cephalic vein is identified and typically retracted laterally with the deltoid. In some cases, it may be ligated if retraction is difficult or if it is injured.
- Blunt and sharp dissection are used to separate the deltoid and pectoralis major muscles.
-
Mobilization and Retraction:
- The deltoid is gently retracted laterally.
- The pectoralis major is retracted medially. Care must be taken to avoid excessive traction on the neurovascular structures within the axilla.
- Deep to the pectoralis major, the clavipectoral fascia is incised. This exposes the conjoined tendon (coracobrachialis and short head of biceps) and the underlying musculature.
-
Exposure of the Joint Capsule:
- The clavipectoral fascia is incised, and the conjoined tendon is identified. It can be retracted medially.
- The underlying subscapularis muscle is now visible, running horizontally from the subscapular fossa to the lesser tuberosity. The axillary nerve and posterior humeral circumflex artery lie inferior and posterior, approximately 5-7 cm distal to the acromion, and care must be taken during inferior dissection and capsular release.
-
Subscapularis Management:
This is a crucial step for gaining access to the GH joint.
- Subscapularis Tenotomy: The preferred method in most primary TSA cases. The subscapularis tendon is released from the lesser tuberosity, typically 1 cm medial to its insertion, preserving a cuff of tendon for later repair. Marking sutures are placed at the superior and inferior borders for reattachment. This can also be performed via lesser tuberosity osteotomy for easier repair in some cases.
- Humeral Head Dislocation: With the subscapularis released, the humerus is externally rotated and extended, dislocating the humeral head posteriorly from the glenoid.
-
Capsular Release:
- Anterior and inferior capsular releases are performed as needed to achieve adequate exposure and mobility.
- The interval between the anterior glenoid rim and the base of the coracoid is often tightened (rotator interval), and its release can improve external rotation.
- Care is taken during inferior release to avoid injury to the axillary nerve and posterior humeral circumflex artery.
-
Humeral Preparation:
- Humeral Head Osteotomy: The osteotomy is performed using an oscillating saw, typically at an angle of 30-45 degrees retroversion relative to the epicondylar axis and 130-145 degrees of inclination relative to the humeral shaft. The goal is to resect sufficient bone to achieve appropriate joint line and prosthetic positioning, often guided by pre-operative templating.
- Humeral Canal Reaming: The humeral canal is sequentially reamed to prepare for the prosthetic stem. Trial components are used to determine appropriate stem size, length, and head offset. The stem can be cemented or uncemented.
-
Glenoid Preparation (for TSA):
- Exposure: The glenoid is exposed by posterior retraction of the humeral shaft. Osteophytes around the glenoid rim are resected to define the true glenoid anatomy.
- Reaming/Resurfacing: The glenoid articular surface is prepared by reaming to create a concentric, flat surface for the glenoid component. Specialized reamers are used, often with an eccentric reamer for B2 glenoids to correct posterior erosion. The aim is to restore normal glenoid version and inclination.
- Component Insertion: The glenoid component (usually polyethylene, cemented) is inserted. Pegs or a keel provide primary stability. Bone grafting may be necessary for significant defects. Ensure adequate cement mantle and removal of excess cement.
- Trial Reduction & Range of Motion: Trial components are inserted, and the shoulder is reduced. Range of motion and stability are assessed. Adjustments may be made (e.g., thicker glenoid component, different humeral head size) to optimize fit and function.
- Final Implant Insertion: Once optimal trial parameters are achieved, definitive components are implanted. Cemented components are typically used for the glenoid, and both cemented and uncemented options exist for the humeral stem.
- Subscapularis Repair: The subscapularis tendon is meticulously reattached to the lesser tuberosity or the remaining cuff of tendon on the humerus using strong non-absorbable sutures. This is critical for post-operative stability and function in TSA.
- Closure: Deep tissues are closed, followed by subcutaneous tissue and skin closure.
Reverse Total Shoulder Arthroplasty (rTSA)
The initial approach is similar to TSA via the deltopectoral interval. Key differences arise in glenoid and humeral preparation, and the absence of subscapularis repair.
-
Glenoid Preparation:
- Exposure: The glenoid exposure is often more extensive, especially inferiorly, to accommodate the larger glenosphere. Aggressive inferior capsular release is common.
- Baseplate Fixation: The glenoid is prepared for the baseplate, which is typically secured with multiple screws into the scapular vault (cancellous bone). A central post is usually cemented. Precise placement is crucial to avoid impingement and ensure stability. Lateralization or medialization can be achieved with specific baseplate designs or spacers.
- Glenosphere Placement: The glenosphere (metal ball) is attached to the baseplate. Various sizes and designs are available to optimize deltoid tension and prevent impingement.
-
Humeral Preparation:
- The humeral head osteotomy differs from TSA, aiming to create a surface for the humeral tray.
- The humeral canal is reamed, and a trial stem and metaphyseal tray are inserted. The polyethylene liner, which articulates with the glenosphere, is chosen to optimize tension and stability.
- Trial Reduction: The shoulder is reduced with trial components. Range of motion (especially external rotation and adduction) and impingement are assessed. The goal is a stable construct with appropriate deltoid tension.
- Final Implant Insertion: Definitive components are inserted. The humeral stem is often uncemented, but cemented options exist.
- Subscapularis: The subscapularis is typically not repaired in rTSA, as its function is replaced by the altered biomechanics relying on the deltoid. This allows for increased external rotation post-operatively.
- Closure: Standard wound closure.
Distal Clavicle Excision (for AC Joint OA)
This procedure can be performed open or arthroscopically.
-
Open Approach:
- Incision: A short transverse or longitudinal incision centered over the AC joint.
- Dissection: The deltoid and trapezius muscle attachments are carefully split/detached from the superior aspect of the AC joint and distal clavicle.
- Resection: Approximately 5-10 mm of the distal clavicle is resected using an oscillating saw. Care is taken to maintain the superior AC joint capsule and the integrity of the coracoclavicular ligaments inferiorly, which are vital for clavicular stability.
- Closure: The deltoid and trapezius attachments are repaired, followed by standard soft tissue and skin closure.
-
Arthroscopic Approach:
- Portals: Typically uses posterior and anterolateral portals.
- Technique: A burr or shaver is used to resect the distal clavicle under direct visualization, ensuring adequate bone removal to prevent impingement (typically 8-10 mm) while preserving soft tissue attachments. This approach offers less soft tissue disruption but can be technically more demanding.
Complications & Management
Shoulder arthroplasty, while generally successful, is associated with a range of potential complications. Understanding their incidence and appropriate management is crucial for all orthopedic surgeons.
Table of Common Complications in Shoulder Arthroplasty and Management
| Complication | Incidence (Approximate) | Salvage/Management Strategy |
|---|---|---|
| Infection | 0.5-2.0% | Acute (<6 weeks): Irrigation & debridement, modular component exchange (if possible), IV antibiotics. Chronic (>6 weeks): Two-stage revision (implant removal, spacer, prolonged IV antibiotics, reimplantation) or resection arthroplasty/arthrodesis in recalcitrant cases. |
| Glenohumeral Instability | 2-5% (higher in rTSA) | Subluxation/Dislocation: Closed reduction (often difficult in rTSA). If recurrent: component revision (glenoid/humeral liner thickness, version, offset adjustment), soft tissue procedures (capsular repair, deltoid advancement), or conversion to rTSA if cuff is deficient (for TSA). |
| Periprosthetic Fracture | 1-3% (humeral more common) | Intra-operative: Fixation with cables/cerclage wires or plates, sometimes necessitating longer stem. Post-operative: ORIF with plate and screws, often requiring revision of humeral stem, or conversion to rTSA if fracture compromises deltoid/cuff function. |
| Aseptic Loosening | 5-10% (glenoid > humeral) | Glenoid: Revision glenoid component (often with bone grafting), conversion to rTSA if significant bone loss or cuff deficiency. Humeral: Revision humeral stem (cemented vs. uncemented), usually with bone grafting. |
| Neurological Injury | 1-4% (Axillary, Suprascapular) | Axillary Nerve: Often neuropraxia, recovery possible. Surgical exploration/neurolysis if no recovery at 3-6 months. Brachial Plexus: Careful positioning, avoid excessive traction. Manage symptoms, nerve repair if transection. Musculocutaneous: Less common. |
| Rotator Cuff Failure | 5-10% (post-TSA) | Post-TSA: Often leads to superior migration and secondary cuff arthropathy. Management ranges from conservative to revision arthroplasty (conversion to rTSA) if symptomatic. |
| Stiffness / Limited ROM | 5-15% | Early: Intensive physiotherapy, manipulation under anesthesia. Late: Arthroscopic capsular release, open capsular release, or revision arthroplasty in severe cases of component malposition. Rule out infection/component issues. |
| Scapular Notching (rTSA) | 50-90% (radiographic) | Primarily a radiographic finding; symptomatic notching less common. Prevention: inferior glenosphere overhang, eccentric glenosphere, humeral neck-shaft angle adjustment, lateralized glenoid baseplate. Management of symptomatic notching (pain, limited ROM): glenosphere revision, soft tissue release, or revision to another rTSA design. |
| Deltoid Dysfunction (rTSA) | 1-5% | Damage to the axillary nerve or direct trauma to the deltoid insertion. Management: PT, bracing. If complete paralysis, functional loss of rTSA. |
| AC Joint Pain (post-TSA) | ~10% | If primary AC pathology was not addressed, secondary impingement or OA can develop. Management: corticosteroid injection, activity modification, or distal clavicle excision (open or arthroscopic). |
| Blood Loss / Hematoma | Varies | Intra-operative: Hemostasis, cell saver. Post-operative: Drain placement, monitoring. Evacuation of symptomatic hematoma. |
| Heterotopic Ossification (HO) | ~15% (radiographic) | Prevention: NSAIDs (Indomethacin) or low-dose radiation post-op in high-risk patients. Management of symptomatic HO (stiffness): Excision only after maturity (typically 1 year post-op) and if conservative measures fail. |
General Management Principles
- Prevention: Meticulous surgical technique, appropriate patient selection, medical optimization, prophylactic antibiotics, and careful rehabilitation.
- Early Recognition: Vigilance for signs and symptoms of complications (e.g., fever, increasing pain, wound discharge, neurological changes, sudden instability).
- Multidisciplinary Approach: Collaboration with infectious disease specialists, neurologists, physical therapists, and pain management teams.
- Revision Surgery: Many complications necessitate revision arthroplasty, which is often more complex and carries higher risks than primary surgery. Bone stock loss, infection, and soft tissue compromise are significant challenges.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgery itself for optimizing outcomes following shoulder arthroplasty. Protocols vary based on the type of arthroplasty (TSA vs. rTSA) and surgeon preference, but generally follow a phased, progressive approach. Close collaboration with physical therapists is essential.
General Principles
- Protect the Repair: Especially the subscapularis repair in TSA and the deltoid in rTSA.
- Early Motion: To prevent stiffness, but within prescribed limits.
- Gradual Progression: Exercises are advanced as healing progresses and pain subsides.
- Patient Education: Crucial for adherence and understanding of limitations.
Total Shoulder Arthroplasty (TSA) Rehabilitation Protocol
Phase I: Immediate Post-operative / Protection Phase (Weeks 0-6)
*
Goals:
Pain control, protect subscapularis repair, minimize stiffness, initiate passive range of motion (PROM).
*
Immobilization:
Arm in a sling (often with an abduction pillow) continuously, removing only for exercises and hygiene.
*
PROM:
*
Forward Flexion:
Supine, passive elevation to 90-120 degrees (patient-assisted or therapist-assisted).
*
External Rotation:
Supine, arm abducted to 30 degrees, passive external rotation to 20-30 degrees (respecting subscapularis repair). Internal rotation is typically avoided in this phase.
*
Pendulum Exercises:
Gentle, non-weight bearing.
*
Active Range of Motion (AROM):
Elbow, wrist, and hand AROM. No active GH motion.
*
Scapular Mobilization:
Gentle scapular retraction and protraction.
*
Restrictions:
No active shoulder motion. No lifting, pushing, or pulling. Avoid sudden movements. No weight-bearing through the arm.
Phase II: Early Motion / Deltoid & Rotator Cuff Strengthening Phase (Weeks 6-12)
*
Goals:
Restore full PROM, initiate active-assisted range of motion (AAROM) and AROM, begin gentle rotator cuff and scapular strengthening.
*
Sling Use:
Gradually weaned, typically for comfort or in public.
*
PROM:
Continue to progress to full PROM (forward flexion, external rotation, internal rotation).
*
AAROM:
*
Forward Flexion:
Pulley exercises, wand exercises (supine and standing).
*
External Rotation:
Wand exercises.
*
AROM:
Gradually introduce AROM (initially gravity-assisted, then against gravity) in pain-free ranges.
*
Strengthening:
*
Isometrics:
Gentle rotator cuff (subscapularis, external rotators) and deltoid isometrics.
*
Scapular Stabilizers:
Low-load exercises (e.g., rows, prone extension).
*
Restrictions:
No lifting >1-2 lbs. No sudden or uncontrolled movements. Avoid positions of extreme external rotation + abduction.
Phase III: Moderate Strengthening / Return to Function Phase (Weeks 12-20)
*
Goals:
Achieve full functional AROM, progressive strengthening, improve endurance.
*
AROM:
Progress towards full pain-free AROM.
*
Strengthening:
*
Progressive Resistive Exercises (PREs):
Rotator cuff, deltoid, scapular musculature using resistance bands, light weights.
*
Eccentric Exercises:
Gradually introduce controlled eccentric loading.
*
Proprioception:
Exercises to improve joint position sense.
*
Functional Activities:
Begin light functional activities, gradually increasing resistance and repetition.
*
Restrictions:
Avoid heavy lifting, repetitive overhead activities.
Phase IV: Advanced Strengthening / Return to Activity (Weeks 20+)
*
Goals:
Maximize strength and endurance, return to recreational activities.
*
Advanced PREs:
Progress to higher resistance, sport-specific drills (if applicable).
*
Endurance Training:
For activities requiring sustained arm use.
*
Return to Activity:
Gradual return to desired activities, with proper body mechanics and pain monitoring. Overhead sports are often not recommended due to stress on the implant.
Reverse Total Shoulder Arthroplasty (rTSA) Rehabilitation Protocol
rTSA protocols differ significantly due to the reliance on the deltoid and the typically deficient rotator cuff. Subscapularis repair is usually not performed, allowing for early external rotation. However, deltoid integrity is paramount.
Phase I: Immediate Post-operative / Protection Phase (Weeks 0-6)
*
Goals:
Pain control, protect deltoid insertion and glenoid fixation, minimize stiffness, initiate PROM (often in a different pattern).
*
Immobilization:
Sling for 3-6 weeks, primarily for comfort and protection, less for rotator cuff healing.
*
PROM:
*
Forward Flexion:
Supine, passive elevation to 90-120 degrees.
*
External Rotation:
Often encouraged to 30-45 degrees, as subscapularis is not repaired.
*
Internal Rotation:
Avoided initially, especially behind the back, to prevent impingement.
*
Active Range of Motion (AROM):
Elbow, wrist, and hand AROM. No active GH motion.
*
Scapular Mobilization:
Gentle scapular retraction and protraction.
*
Restrictions:
Crucially, avoid active internal rotation and hyperextension, especially with abduction.
This puts stress on the anterior-inferior glenoid fixation and risks anterior dislocation. No lifting, pushing, or pulling.
Phase II: Early Motion / Gentle Deltoid Activation Phase (Weeks 6-12)
*
Goals:
Achieve functional PROM, initiate gentle AROM focusing on deltoid, improve active elevation.
*
Sling Use:
Gradually weaned.
*
PROM:
Continue to progress to full PROM.
*
AAROM/AROM:
*
Forward Flexion:
Progress to active elevation through deltoid activation.
*
Abduction:
Active abduction (the deltoid's primary role in rTSA).
*
External Rotation:
Continue to progress.
*
Internal Rotation:
Still limited, avoid significant behind-the-back motion.
*
Strengthening:
Gentle deltoid isometrics, scapular stabilization exercises.
*
Restrictions:
No lifting >1-2 lbs. Avoid combined adduction, internal rotation, and extension (high risk of dislocation).
Phase III: Moderate Strengthening / Functional Re-integration (Weeks 12-20)
*
Goals:
Maximize deltoid strength, achieve functional AROM, improve endurance.
*
AROM:
Progress towards functional AROM.
*
Strengthening:
*
Progressive Resistive Exercises (PREs):
Focus on deltoid and scapular stabilizers. Limited rotator cuff strengthening if a small cuff tear was present/repaired.
*
Functional Activities:
Gradually introduce activities of daily living.
*
Restrictions:
Continue to avoid extreme internal rotation, adduction, and extension. No heavy lifting.
Phase IV: Advanced Strengthening / Return to Activity (Weeks 20+)
*
Goals:
Maximize strength and functional capacity within the limitations of the implant.
*
Advanced PREs:
Higher resistance, functional training.
*
Return to Activity:
Gradual return to desired activities. Overhead activities may be limited due to the unique biomechanics of rTSA. Avoid high-impact or contact sports.
Distal Clavicle Excision Rehabilitation
This protocol is typically less intensive.
*
Phase I (Weeks 0-2):
Sling for comfort. AROM for elbow, wrist, hand. Pendulum exercises. Gentle PROM for shoulder.
*
Phase II (Weeks 2-6):
Wean from sling. Progress AROM to full. Initiate light strengthening for rotator cuff and scapular muscles. Avoid heavy lifting and overhead activities.
*
Phase III (Weeks 6+):
Progressive strengthening, return to full activities as tolerated. Return to sports after 3-4 months.
Summary of Key Literature / Guidelines
The body of literature on shoulder osteoarthritis and its surgical management is extensive, with ongoing advancements in implant design, surgical techniques, and rehabilitation protocols. Key literature and guidelines inform evidence-based practice:
-
Total Shoulder Arthroplasty (TSA) Outcomes:
- Long-Term Durability: Numerous studies demonstrate excellent long-term pain relief and functional improvement with TSA, with survivorship rates exceeding 90% at 10 years and 80% at 15 years for aseptic loosening. The glenoid component remains the weak link, with higher rates of aseptic loosening compared to the humeral component.
- Glenoid Bone Loss: The Walch classification for glenoid morphology is widely adopted and guides surgical decision-making, particularly regarding the need for eccentric reaming, augmented glenoid components, or bone grafting in B2 and C glenoids to restore proper version and avoid early failure.
- Cemented vs. Uncemented Humerus: While cemented humeral stems have been the gold standard, uncemented stems have shown comparable results in younger, active patients with good bone quality, potentially reducing operative time and cement-related complications.
- Short Stem vs. Standard Stem: Emerging literature suggests that short-stem or stemless humeral components offer similar short-to-mid-term outcomes to conventional stems for appropriate indications, with advantages such as bone preservation and easier revision.
-
Reverse Total Shoulder Arthroplasty (rTSA) Outcomes:
- Rotator Cuff Arthropathy (RCA): rTSA has revolutionized the treatment of symptomatic RCA and deltoid-deficient shoulders, providing reliable pain relief and significant functional restoration, particularly active elevation. Outcomes are superior to hemiarthroplasty in this population.
- Expanded Indications: Indications have expanded beyond RCA to include revision arthroplasty, complex proximal humeral fractures in the elderly, and severe glenohumeral OA with significant glenoid bone loss and poor soft tissue coverage.
- Complication Profile: While highly effective, rTSA has a distinct complication profile, with higher rates of glenoid-sided complications (notching, baseplate loosening) and potentially higher rates of infection and instability compared to TSA, especially in early series. Modern designs and surgical techniques have significantly reduced these.
- Scapular Notching: Although often radiographic, symptomatic scapular notching remains a concern. Studies have shown that lateralizing the center of rotation (e.g., using lateralized glenoid baseplates or more laterally offset humeral components) can reduce the incidence and severity of notching.
-
AC Joint Osteoarthritis:
- Distal Clavicle Excision: Both open and arthroscopic distal clavicle excision are effective procedures for symptomatic AC joint OA refractory to conservative management. Arthroscopic techniques may offer quicker recovery and less soft tissue dissection, but require specific arthroscopic expertise. Outcomes are generally favorable, with good pain relief.
- Concomitant Pathology: Studies emphasize careful differentiation between primary AC joint pathology and referred pain from other shoulder conditions (e.g., rotator cuff tendinopathy, GH OA) to ensure appropriate intervention.
-
Evidence-Based Guidelines:
- AAOS (American Academy of Orthopaedic Surgeons): Publishes clinical practice guidelines and appropriate use criteria for various orthopedic conditions, including shoulder arthroplasty, providing recommendations based on systematic reviews of the literature. These guidelines typically support arthroplasty for severe pain and functional limitation refractory to non-operative treatment, with specific recommendations for TSA vs. rTSA based on rotator cuff integrity.
- International Societies: European Society for Surgery of the Shoulder and Elbow (ESSSE/SECEC) and ISAKOS (International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine) also contribute to consensus statements and research driving best practices.
In conclusion, the surgical management of shoulder osteoarthritis, primarily through arthroplasty, is a highly effective treatment for debilitating symptoms. Adherence to meticulous surgical technique, evidence-based patient selection, and structured post-operative rehabilitation, all informed by a robust understanding of surgical anatomy and biomechanics, are critical for achieving optimal and durable outcomes.
You Might Also Like