Optimizing Perioperative Pain Management in Shoulder Surgery: An Academic Review
Key Takeaway
Optimizing perioperative pain management in shoulder surgery is crucial for enhancing recovery, improving functional outcomes, and boosting patient satisfaction. It significantly reduces opioid consumption, mitigating side effects, and facilitates early, active participation in rehabilitation. A deep understanding of surgical anatomy and regional anesthesia techniques is key to achieving these superior patient-centered results.
Optimize Shoulder Surgery Perioperative Pain for Faster Recovery
Introduction & Epidemiology
Adequate perioperative pain management is a cornerstone of modern shoulder surgery, directly influencing patient recovery trajectories, functional outcomes, and satisfaction. Shoulder pathologies are a significant cause of morbidity, with surgical interventions for conditions such as rotator cuff tears, instability, osteoarthritis, and fractures being increasingly common. The global burden of these conditions underscores the need for optimized surgical and perioperative care pathways.
The historical context of regional anesthesia dates back to William Halsted's pioneering use of cocaine for peripheral nerve blockade in 1885. Over the past three decades, there has been a significant surge in the adoption of peripheral nerve blocks for managing postoperative pain, particularly in orthopedic surgery. This shift is driven by a robust evidence base demonstrating numerous benefits:
* Decreased hospital length of stay, facilitating a transition from traditional inpatient to outpatient surgical models where appropriate.
* Significant reduction in opioid consumption, thereby mitigating the incidence and severity of opioid-related side effects such as nausea, vomiting, constipation, pruritus, and respiratory depression. This also contributes to addressing the broader public health crisis of opioid dependency.
* Enhanced patient participation in crucial early rehabilitation protocols by providing superior baseline analgesia.
* Improved functional recovery and higher patient satisfaction scores.
* Demonstrable cost-effectiveness by reducing overall resource utilization and complication rates.
A comprehensive understanding of surgical anatomy, meticulous patient selection, and a thorough grasp of the indications, contraindications, and potential complications associated with regional anesthesia techniques are paramount for orthopedic surgeons and anesthesiologists collaborating in the perioperative setting. This guide aims to provide a high-yield academic review of optimizing perioperative pain management for shoulder surgery, integrating contemporary evidence and best practices.
Surgical Anatomy & Biomechanics
A profound understanding of shoulder anatomy, particularly the neurovascular structures, is indispensable for both safe surgical execution and effective regional anesthesia.
Bony Anatomy
The shoulder complex comprises the scapula, humerus, and clavicle. Key bony landmarks include the glenoid, humeral head, greater and lesser tuberosities, bicipital groove, acromion, coracoid process, and spine of the scapula. The congruity of the glenohumeral joint is inherently unstable, relying heavily on soft tissue restraints.
Ligamentous and Capsular Anatomy
The glenohumeral joint capsule, reinforced by the superior, middle, and inferior glenohumeral ligaments, provides static stability. The coracoacromial ligament forms part of the coracoacromial arch, an important structure in subacromial impingement.
Muscular Anatomy
The rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) are critical for dynamic stability and arm rotation. Other significant muscles include the deltoid, pectoralis major, latissimus dorsi, and biceps brachii.
Neurovascular Anatomy
The brachial plexus is the primary neural supply to the shoulder and upper extremity. It is formed by the ventral rami of spinal nerves C5, C6, C7, C8, and T1.
*
Roots:
C5, C6, C7, C8, T1 merge to form the trunks.
*
Trunks:
Superior (C5, C6), Middle (C7), Inferior (C8, T1).
*
Divisions:
Each trunk divides into anterior and posterior divisions, supplying flexor and extensor compartments, respectively.
*
Cords:
Lateral, Posterior, Medial, named relative to the axillary artery.
*
Terminal Nerves:
Major nerves supplying the shoulder and upper limb include the musculocutaneous, axillary, radial, median, and ulnar nerves.
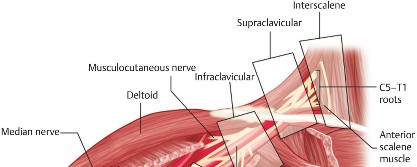
For shoulder surgery, the most relevant nerves for regional anesthesia derive primarily from the C5-C7 roots, including the suprascapular nerve (C5, C6) and the axillary nerve (C5, C6).

Figure 1. Detailed anatomy of the brachial plexus showing roots, trunks, divisions, cords, and terminal branches.
The subclavian artery and its branches, particularly the axillary artery, provide the main arterial supply. Proximity of these vessels to the brachial plexus necessitates careful attention during regional block procedures.
Biomechanics
Shoulder biomechanics are complex, involving coordinated motion of the glenohumeral, scapulothoracic, sternoclavicular, and acromioclavicular joints. Pathologies often disrupt this intricate balance, leading to pain, weakness, and restricted motion. Understanding normal kinematics is crucial for surgical planning and rehabilitation.
Indications & Contraindications
Indications for shoulder surgery are broad and depend on the underlying pathology, patient symptoms, functional deficits, and response to non-operative management. Effective pain control is crucial for all operative indications to facilitate recovery.
Indications for Shoulder Surgery
| Operative Indications | Non-Operative Indications / Initial Management |
|---|---|
| Rotator Cuff Pathology | Acute, small, traumatic tears (often amenable to conservative care) |
| * Symptomatic full-thickness tears (acute or chronic) | Partial-thickness tears without significant functional deficit |
| * Large/massive irreparable tears (for superior capsule reconstruction or tendon transfer) | Degenerative tears without significant pain/dysfunction |
| * Failed conservative management for partial-thickness tears | Impingement with mild symptoms, no structural damage |
| Shoulder Instability | First-time traumatic dislocations without significant bone loss |
| * Recurrent anterior/posterior instability | Atraumatic multidirectional instability (physical therapy focus) |
| * Significant glenoid/humeral bone loss (e.g., Bankart, Hill-Sachs lesions) | Subluxation episodes without frank dislocation |
| * Failed non-operative management | |
| Arthritis | Mild to moderate glenohumeral or acromioclavicular osteoarthritis (NSAIDs, injections, PT) |
| * Severe glenohumeral osteoarthritis (total shoulder arthroplasty, hemiarthroplasty, reverse shoulder arthroplasty) | |
| * Severe acromioclavicular osteoarthritis (distal clavicle excision) | |
| Fractures | Stable, non-displaced humeral head/neck fractures |
| * Displaced humeral head/neck fractures | Scapular fractures (usually treated non-operatively) |
| * Glenoid fractures with significant articular step-off or instability | |
| * Clavicle fractures with significant displacement, shortening, or neurovascular compromise | |
| Other | |
| * Adhesive capsulitis (failed conservative management) | Initial management for adhesive capsulitis (PT, injections) |
| * Superior labrum anterior-posterior (SLAP) lesions (Type II-IV) | Type I SLAP lesions (degenerative fraying) |
| * Infection, tumors |
Contraindications to Regional Anesthesia
While highly beneficial, regional anesthesia is not without contraindications. These can be absolute or relative:
*
Absolute Contraindications:
* Patient refusal.
* Infection at the injection site.
* Coagulopathy or anticoagulation that cannot be safely reversed (risk of hematoma, though relative for some blocks).
* Local anesthetic allergy.
* Pre-existing neurological deficit in the operative limb that could be exacerbated or masked.
*
Relative Contraindications:
* Severe pulmonary disease (e.g., severe COPD, due to risk of phrenic nerve palsy with interscalene block).
* Uncooperative patient.
* Anatomical distortion or scarring from prior surgery/radiation.
* Significant anatomical variations of the brachial plexus.
Pre-Operative Planning & Patient Positioning
Comprehensive pre-operative planning is essential for optimizing pain management and facilitating a smooth surgical course.
Multimodal Analgesia Strategy
A multimodal approach to pain management is recognized as the gold standard. This involves combining multiple analgesic agents and techniques with different mechanisms of action to achieve synergistic pain relief, minimize side effects, and reduce opioid requirements. Key components include:
*
Regional Anesthesia:
Central to perioperative pain control in shoulder surgery.
*
NSAIDs/COX-2 Inhibitors:
Administered pre-emptively, when not contraindicated (e.g., renal insufficiency, active ulcer disease).
*
Acetaminophen:
Routinely given pre-operatively and continued post-operatively.
*
Gabapentinoids (Gabapentin/Pregabalin):
May reduce acute postoperative pain and opioid consumption, though evidence is somewhat mixed regarding routine use.
*
Corticosteroids:
A single dose of dexamethasone intraoperatively may reduce post-operative nausea and vomiting (PONV) and pain.
*
Opioids:
Used as a rescue medication or for breakthrough pain, minimized as much as possible.
Regional Anesthesia Planning
The selection of the specific brachial plexus block depends on the extent of surgery, expected duration of pain, patient comorbidities, and surgeon/anesthesiologist preference and expertise. The primary goal is to achieve adequate analgesia while minimizing potential complications.
Brachial Plexus Blocks for Shoulder Surgery
-
Interscalene Brachial Plexus Block (ISB):
- Anatomy: Targets the brachial plexus at the level of the roots/trunks between the anterior and middle scalene muscles. Provides excellent analgesia for the shoulder joint, proximal humerus, and lateral clavicle.
- Technique: Traditionally performed using nerve stimulation, now predominantly guided by ultrasound. The transducer is placed transversely at the level of the cricoid cartilage to visualize the sternocleidomastoid, anterior scalene, and middle scalene muscles. The brachial plexus components appear as hypoechoic ovoid structures within the interscalene groove. Local anesthetic is injected around these structures.
- Advantages: Superior pain control for shoulder surgery. Can be performed as a single shot or continuous catheter for prolonged analgesia.
-
Disadvantages/Complications:
- Phrenic nerve palsy: Most common complication (nearly 100% with ISB), leading to ipsilateral hemidiaphragmatic paresis. Clinically significant in patients with pre-existing severe pulmonary compromise (e.g., severe COPD, sleep apnea). Careful patient selection and lower volume/concentration blocks may reduce its impact.
- Hoarseness (recurrent laryngeal nerve block): Due to local anesthetic spread.
- Horner's syndrome (stellate ganglion block): Ptosis, miosis, anhydrosis. Transient.
- Vascular puncture: Risk of hematoma.
- Intrathecal/epidural injection: Rare but serious.
-
Consideration:
For highly respiratory-compromised patients, alternative blocks or lower volume ISB with careful titration may be preferred.

Figure 2. Ultrasound view of an interscalene block showing the brachial plexus components between the anterior and middle scalene muscles.
-
Supraclavicular Brachial Plexus Block (SCB):
- Anatomy: Targets the brachial plexus at the level of the divisions, superior to the clavicle, lateral to the subclavian artery. Often referred to as the "spinal of the arm."
- Technique: Ultrasound-guided. Transducer placed in the supraclavicular fossa, visualizing the subclavian artery and the brachial plexus (often appearing as a "bunch of grapes" or "honeycomb" superior and lateral to the artery).
- Advantages: Provides dense block of the entire upper extremity distal to the shoulder. Lower incidence of phrenic nerve palsy compared to ISB as the phrenic nerve exits higher.
-
Disadvantages/Complications:
- Pneumothorax: Although rare with ultrasound guidance, proximity to the pleura makes it a significant risk.
- Horners syndrome: Possible.
- May spare C5/C6 branches leading to incomplete shoulder analgesia.
- Consideration: More suitable for procedures involving the distal upper extremity, but can provide good shoulder analgesia, especially if C5/C6 coverage is ensured.
-
Suprascapular Nerve Block (SSNB):
- Anatomy: Targets the suprascapular nerve (C5, C6) as it passes through the suprascapular notch or spinoglenoid notch. This nerve supplies the supraspinatus and infraspinatus muscles and provides sensory innervation to the superior and posterior shoulder capsule and glenohumeral joint.
- Technique: Can be performed with ultrasound or landmark-based. Ultrasound guidance is preferred, targeting the nerve at the suprascapular notch or the spinoglenoid notch.
- Advantages: Targets specific pain pathways of the shoulder joint, especially useful for chronic shoulder pain or as an adjunct. Spares motor function of deltoid and biceps, avoids phrenic nerve palsy. Can be combined with an axillary nerve block for more comprehensive shoulder analgesia.
- Disadvantages: Does not provide comprehensive analgesia for extensive shoulder surgery alone. Primarily sensory.
-
Axillary Nerve Block:
- Anatomy: The axillary nerve (C5, C6) arises from the posterior cord and wraps around the surgical neck of the humerus. It innervates the deltoid and teres minor muscles and provides sensory innervation to the lateral shoulder (regimental badge area).
- Technique: Ultrasound-guided, targeting the nerve in the quadrangular space or more proximally in the axilla.
- Advantages: Targets specific shoulder innervation, avoids phrenic nerve palsy.
- Disadvantages: Limited coverage for comprehensive shoulder surgery. Best used in combination with SSNB or as part of a multimodal strategy.
Patient Positioning for Surgery
The most common positions for shoulder surgery are the beach chair position and lateral decubitus position. Each has implications for regional anesthesia and surgical access.
*
Beach Chair Position:
*
Advantages:
Allows for easy conversion to open procedures if needed, generally better visualization of anterior and superior structures. Easier access for interscalene block prior to positioning.
*
Disadvantages:
Risk of cerebral hypoperfusion (stroke, vision loss), particularly in hypotensive patients. Careful blood pressure monitoring and management are critical. Access to posterior shoulder is limited.
*
Lateral Decubitus Position:
*
Advantages:
Excellent visualization of posterior, inferior, and superior structures, particularly for arthroscopic procedures. Avoids cerebral hypoperfusion risks associated with beach chair.
*
Disadvantages:
Potential for brachial plexus traction injury, especially with excessive traction. Risk of peripheral nerve compression (e.g., ulnar nerve at elbow, peroneal nerve at fibular head). Requires careful padding and positioning. Access for regional blocks may be slightly more challenging post-positioning but can be performed pre-positioning.
For regional blocks, it's often preferable to perform them before final surgical positioning, with the patient in a comfortable supine or semi-recumbent position, allowing optimal access and patient cooperation.
Detailed Surgical Approach / Technique
While this guide focuses on pain management, an understanding of surgical techniques is crucial as they influence pain generation and the efficacy of pain control strategies. The following outlines general principles applicable to common shoulder procedures.
General Surgical Principles
- Anesthesia: General anesthesia is typically employed, often combined with regional anesthesia for a "fast-track" or "enhanced recovery after surgery" (ERAS) approach.
- Tourniquet: Not generally used for shoulder surgery.
- Approach: Arthroscopic approaches are increasingly common, minimizing soft tissue disruption. Open approaches are reserved for specific complex cases (e.g., large rotator cuff repairs, total shoulder arthroplasty, complex fracture fixation).
Arthroscopic Shoulder Surgery (e.g., Rotator Cuff Repair, Labral Repair)
- Patient Positioning: Beach chair or lateral decubitus. Arm is typically suspended with traction.
-
Portal Placement:
- Posterior Portal: Primary viewing portal, approximately 2 cm inferior and 1 cm medial to the posterior-lateral corner of the acromion.
- Anterior Portal(s): Working portals, typically located anterior to the acromion, lateral to the coracoid.
- Lateral Portal(s): Accessory portals for specialized instruments, often for rotator cuff repair.
- Diagnostic Arthroscopy: Systematic evaluation of glenohumeral joint and subacromial space.
- Debridement/Preparation: Resection of inflamed tissue, debridement of torn labrum or rotator cuff edges. Acromioplasty may be performed for impingement.
-
Repair/Fixation:
- Rotator Cuff Repair: Mobilization of torn tendon, preparation of bony footprint (debridement, decortication), anchor placement (suture anchors or all-suture anchors) into the greater tuberosity, and re-attachment of tendon.
- Labral Repair: Suture anchor placement into the glenoid rim, re-tensioning and repair of the labral tissue.
-
Closure:
Portals are closed with sutures or steristrips.

Figure 3. Arthroscopic view of a shoulder joint, illustrating typical working portals and scope placement.
Open Shoulder Surgery (e.g., Total Shoulder Arthroplasty, Complex Fracture Fixation)
- Incision: Often a deltopectoral approach for total shoulder arthroplasty, or a more direct deltoid-splitting approach for certain fracture fixations.
- Dissection: Careful dissection through internervous planes to expose the surgical site, minimizing muscle and nerve damage. For deltopectoral approach, interval between deltoid (axillary nerve innervation) and pectoralis major (medial and lateral pectoral nerve innervation). Cephalic vein is identified and preserved.
- Exposure: Retraction of muscles (e.g., subscapularis for total shoulder arthroplasty) to access the joint.
-
Procedure-Specific Steps:
- Arthroplasty: Humeral head resection, glenoid preparation, prosthetic implantation.
- Fracture Fixation: Reduction of fracture fragments, internal fixation with plates and screws.
- Closure: Meticulous layered closure, ensuring anatomical repair of muscles and capsule.
Intraoperative Pain Management Considerations
- Local Anesthetic Infiltration: Liberal infiltration of surgical tissues (capsule, subacromial space, portal sites) with long-acting local anesthetics (e.g., bupivacaine, ropivacaine) can provide supplemental analgesia. Liposomal bupivacaine (Exparel) can offer prolonged local analgesia.
- Continuous Regional Catheters: For cases with anticipated severe or prolonged pain (e.g., total shoulder arthroplasty, large rotator cuff repairs), a continuous interscalene or suprascapular nerve catheter can be placed intraoperatively or pre-operatively to provide several days of analgesia.
Complications & Management
Complications in shoulder surgery can be related to the surgical procedure itself or the perioperative pain management strategies. A proactive approach to identifying and managing these is critical.
Surgical Complications
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Rotator Cuff Re-Tear (Post-repair) | 10-50% |
Non-operative: activity modification, NSAIDs, injections, physical therapy.
Operative: revision rotator cuff repair (direct, augmentation, superior capsule reconstruction), tendon transfer, reverse shoulder arthroplasty (for cuff tear arthropathy). |
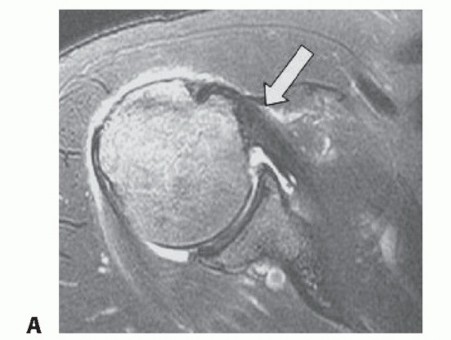
Clinical & Radiographic Imaging

You Might Also Like