Pediatric Femur Fracture Management in Cerebral Palsy with Osteopenia: Case 37

Key Takeaway
Managing femur fractures in children with GMFCS IV cerebral palsy and osteopenia presents unique challenges. Orthopedic specialists must address weakened, osteopenic bone, pre-existing spasticity, and contractures that complicate alignment and implant stability. Detailed imaging like CT is crucial for surgical planning, ensuring adequate fixation and considering long-term bone health strategies for these complex pediatric patients.
Patient Presentation & History
We present Case 37, an 8-year-old male with a history of spastic quadriplegic cerebral palsy (CP), classified as Gross Motor Function Classification System (GMFCS) Level IV, presenting with an acute right mid-diaphyseal femur fracture. The patient's underlying CP etiology is presumed perinatal anoxic brain injury. His baseline functional status involves wheelchair mobility for all locomotion, requiring extensive assistance for transfers, toileting, and all activities of daily living. He has a history of severe adductor and hamstring spasticity, previously managed with multiple botulinum toxin injections and bilateral adductor longus releases and hamstring lengthenings at age 5, which improved passive range of motion and ease of hygiene, but did not alter his GMFCS level. Known comorbidities include osteopenia secondary to chronic immobility and antiepileptic medication use, as well as a seizure disorder well-controlled on valproic acid.
The mechanism of injury was a low-energy fall during a caregiver-assisted transfer from his wheelchair to a changing table. The caregiver reported a sudden "pop" followed by immediate pain, crying, and obvious deformity of the right thigh. There was no direct impact to the thigh described, suggesting an insufficiency fracture component or high stress on osteopenic bone during a rotational movement. There were no other injuries reported or observed, and no concerns for non-accidental injury were raised.
Clinical Examination
Upon presentation, the patient was alert but distressed, complaining of severe right thigh pain. Vital signs were stable.
General Inspection:
* Right lower extremity held in external rotation and abduction with gross angulation and foreshortening of the mid-thigh.
* Significant swelling and ecchymosis evident over the anterior and lateral aspects of the right thigh. Skin integrity appeared intact, though stretched over the apex of the deformity.
* Pre-existing fixed flexion contractures of both hips (approximately 30 degrees) and knees (approximately 20 degrees) were noted, consistent with his GMFCS Level IV spastic quadriplegia. Significant hamstring and adductor spasticity was evident on passive range of motion of the unaffected limb.
Palpation:
* Exquisite tenderness to palpation circumferentially over the mid-diaphyseal region of the right femur.
* Crepitus was elicited with gentle manipulation.
* No open wounds or signs of compartment syndrome.
* Pulses (dorsalis pedis, posterior tibial) were palpable and strong bilaterally. Capillary refill in the toes was brisk (<2 seconds).
Range of Motion (ROM):
* Active ROM of the right hip and knee was severely limited by pain.
* Passive ROM was cautiously attempted, revealing severe limitation due to the fracture. Pre-existing hip and knee contractures were noted on the contralateral limb, providing a baseline.
Neurological/Vascular Assessment:
* Distal neurological function was difficult to assess precisely due to the patient's baseline CP and lack of voluntary motor control, but sensation to light touch in the L5-S1 dermatomes of the right foot was present, and toe flexion/extension was grossly attempted, indicating preserved motor function beyond the level of injury. No acute neurological deficit attributed to the trauma was identified.
* Distal pulses were 2+/4 bilaterally, and the right foot was warm and well-perfused with no signs of vascular compromise.
Imaging & Diagnostics
Initial Radiographs:
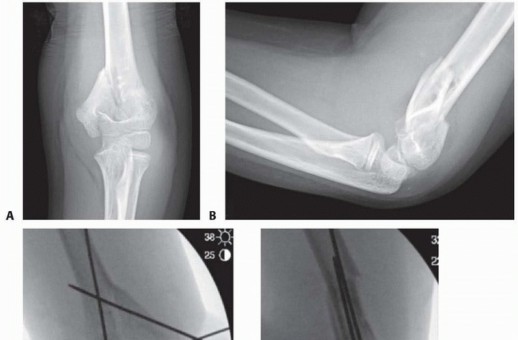
Antero-posterior (AP) and lateral radiographs of the right femur were obtained. These revealed a comminuted, spiral mid-diaphyseal fracture of the right femur with significant overriding, approximately 40 degrees of varus angulation, and 30 degrees of external rotation. The bone cortex appeared thinned, and overall bone density was reduced, consistent with known osteopenia. No evidence of pre-existing lytic or blastic lesions was identified.
Figure 1: Initial AP radiograph of the right femur demonstrating a comminuted mid-diaphyseal fracture with significant angulation and overriding.
Computed Tomography (CT) Scan:
A CT scan of the right femur was performed to precisely characterize the fracture geometry, degree of comminution, and bone quality, aiding in surgical planning. The CT confirmed a long spiral component with a significant butterfly fragment. Cortical thinning was pronounced, raising concerns about implant purchase and potential for delayed union or nonunion. No intra-articular extension was observed. The CT also provided valuable information regarding the pre-existing femoral bowing and rotational alignment, crucial for achieving appropriate post-operative limb alignment in a patient with underlying spasticity-induced deformities.
Other Diagnostics:
* Pre-operative laboratory workup including complete blood count, coagulation profile, and basic metabolic panel were within normal limits.
* Vitamin D levels were obtained, showing insufficiency, which was managed with supplementation post-operatively.
* Dual-energy X-ray absorptiometry (DEXA) scan, while not acutely indicated, was planned post-stabilization to guide long-term management of osteopenia.
Differential Diagnosis
Given the acute presentation of pain and deformity following a low-energy mechanism in a child with pre-existing comorbidities, a comprehensive differential diagnosis was considered.
| Feature | Acute Traumatic Femur Fracture (Case 37) | Pathological Femur Fracture (Osteopenia/Tumor) | Non-Accidental Injury (NAI) / Child Abuse |
|---|---|---|---|
| Patient History | Low-energy fall during transfer in a GMFCS IV CP patient with osteopenia. Specific event reported. | Minimal or no trauma, often repetitive minor stress. Known systemic condition (osteopenia) or new onset constitutional symptoms (tumor). | Vague or inconsistent history. Delay in seeking care. Inconsistent with reported mechanism. |
| Clinical Presentation | Acute pain, gross deformity, swelling, ecchymosis. Caregiver witnessed. | Acute or subacute pain, swelling. Deformity may be less pronounced initially, or progressive. No clear traumatic event. | Bruising/injuries in various stages of healing. Fearful demeanor. History of multiple prior "accidents." |
| Radiographic Findings | Spiral/oblique/comminuted mid-diaphyseal fracture. Signs of osteopenia (cortical thinning, reduced trabecular bone). No other skeletal injuries. | Fracture through an area of pre-existing bone abnormality (lytic lesion, cortical thinning, diffuse osteopenia). Absence of significant trauma. Bone scan may show other areas of increased uptake. | Spiral or metaphyseal fractures in young children. Multiple fractures of varying ages. Rib fractures, skull fractures. Corner fractures, bucket handle fractures. |
| Lab Findings | Typically normal. May show Vitamin D insufficiency. | May show tumor markers, hypercalcemia (tumor), severe Vitamin D deficiency, metabolic bone disease markers. | Labs often normal, but may show anemia, coagulopathy (rare). |
| Risk Factors | Cerebral palsy, GMFCS Level IV, osteopenia, antiepileptic medication. | Underlying systemic condition (e.g., osteogenesis imperfecta, CP with severe osteopenia, malignancy). | Young child, caregiver stress, socioeconomic factors, disability (CP can increase NAI risk). |
| Management Implications | Prompt surgical stabilization to facilitate care, pain control, and rehabilitation. Address osteopenia. | Biopsy may be required for definitive diagnosis if tumor suspected. Address underlying metabolic bone disease. Surgical stabilization often indicated. | Mandated reporting to child protective services. Detailed skeletal survey. Multi-disciplinary team involvement. |
Surgical Decision Making & Classification
The decision for operative intervention was paramount in this case, primarily driven by the patient's underlying cerebral palsy, GMFCS Level IV status, and the inherent challenges of non-operative management in this population.
Rationale for Operative Intervention:
1.
GMFCS Level IV Considerations:
For a non-ambulatory child with severe CP, the primary goals of fracture treatment shift from restoring full ambulatory function to enabling ease of care, pain control, maintaining a functional sitting position, preventing pressure sores, and facilitating ongoing rehabilitation (e.g., transfers, hygiene, seating). Non-operative management with a spica cast would severely hinder these goals, impede caregiver assistance, and exacerbate existing contractures and skin breakdown risks.
2.
Spasticity Management:
The strong, uncoordinated muscle forces in a spastic limb make cast immobilization highly prone to displacement, malunion, or nonunion. Persistent spasticity against a fracture site can cause ongoing pain and further displacement, even within a cast. Surgical fixation provides rigid stability, allowing for earlier mobilization and controlled stretching, which can mitigate the negative impact of spasticity.
3.
Bone Quality:
The patient's osteopenia further complicates non-operative management. Poor bone quality means less reliable cast purchase and higher risk of progressive deformity. It also necessitates robust internal fixation.
4.
Pain Control and Rehabilitation:
Operative stabilization provides superior pain control compared to conservative measures, allowing for a more immediate and effective start to post-operative physical therapy, crucial for maintaining baseline function and preventing secondary complications such as contractures and pressure ulcers.
Fracture Classification:
*
Location:
Mid-diaphyseal femur fracture.
*
Morphology:
Comminuted, long spiral, with a significant butterfly fragment. Based on Winquist and Hansen classification, this could be considered a Type III (25-50% comminution) or Type IV (greater than 50% comminution, segmental) depending on the exact comminution extent, necessitating robust fixation.
*
AO Pediatric Fracture Classification:
32-D/3.1 (femur, diaphyseal, simple/spiral with potential segmental component).
Implant Selection Decision-Making:
Given the patient's age (8 years), bone quality (osteopenia), and GMFCS Level IV status (high spasticity, non-weight-bearing/transfers), the following options were considered:
*
Flexible Intramedullary Nails (TENS):
Generally suitable for younger children (up to 10-12 years) with stable diaphyseal fractures. However, in this case, the significant comminution, osteopenia, and high spasticity forces made TENS unlikely to provide sufficient stability. Risk of shortening, angulation, and delayed union would be high.
*
External Fixation:
While providing rigid stabilization, it carries a high risk of pin site infection, soft tissue complications, and can be cumbersome for a non-ambulatory patient with CP during transfers and hygiene.
*
Submuscular Plating:
A viable option for diaphyseal fractures, particularly in osteopenic bone, offering good stability. However, it involves a larger soft tissue dissection and potential for stress shielding.
*
Locked Intramedullary Nailing (IMN):
Considered the most appropriate choice. For an 8-year-old, a trochanteric entry point IMN offers superior stability, particularly with reaming, allowing for a larger diameter nail. It provides axial stability and rotational control crucial for managing spasticity, preserves periosteal blood supply, and facilitates early mobilization with minimal external support. The potential risk of avascular necrosis (AVN) of the femoral head with piriformis entry in a skeletally immature patient was a strong contraindication for that approach; hence, a trochanteric entry nail was favored.
Therefore, the decision was made for reamed antegrade locked intramedullary nailing via a trochanteric entry point.
Surgical Technique / Intervention
Pre-operative Planning:
Detailed pre-operative planning involved templating on radiographs and CT scans to determine appropriate nail length and diameter. The presence of pre-existing femoral bowing and rotational deformities, common in GMFCS Level IV patients, necessitated careful consideration to ensure proper post-operative alignment, preventing functional impingement or exacerbation of existing contractures.
Patient Positioning and Anesthesia:
The patient was placed supine on a radiolucent fracture table. The contralateral limb was positioned in abduction to allow adequate C-arm access. The injured right lower extremity was placed in traction through a distal femoral pin to achieve preliminary length and alignment, facilitating closed reduction. General endotracheal anesthesia was administered.
Surgical Approach:
A 3-4 cm longitudinal incision was made laterally over the greater trochanter, ensuring the incision was slightly posterior to the tip to avoid the abductor musculature during entry. A muscle-splitting approach was used to expose the greater trochanteric apophysis. The entry portal was established at the tip of the greater trochanter, slightly medial and anterior, to optimize nail trajectory down the femoral shaft, aiming to avoid disruption of the piriformis fossa and minimize risk of AVN. A K-wire was used to guide the entry reamer.
Reduction Techniques:
Closed reduction was primarily achieved using longitudinal traction and manipulation via external rotation of the limb. Intraoperative fluoroscopy (AP and lateral views) was used extensively to confirm alignment. In cases of persistent malalignment, various maneuvers, including gentle manual pressure at the fracture site or temporary K-wire joystick techniques, would have been considered. For this comminuted fracture, maintaining length and rotational alignment was challenging, but ultimately achieved with persistent traction and rotational control.
Nail Insertion and Reaming:
A guidewire was carefully advanced across the fracture site and into the distal femoral metaphysis, ensuring it remained centrally placed in both AP and lateral views. Sequential reaming was performed, gradually increasing the reamer size until cortical chatter was felt, indicating reamer contact with the inner cortex. Reaming was performed to a diameter 0.5 mm larger than the selected nail diameter to facilitate insertion and reduce intra-cortical stresses. A 9.0 mm diameter locked intramedullary nail was chosen based on templating and reaming feedback.
Nail Insertion and Locking:
The selected antegrade intramedullary nail was inserted over the guidewire. Careful attention was paid to the nail's tip progression to avoid iatrogenic fracture. Once the nail tip was seated approximately 1-2 cm from the distal femoral physis, proximal and distal locking screws were inserted under fluoroscopic guidance. Two proximal locking screws were used to enhance rotational stability, particularly important given the patient's spasticity. Two distal locking screws were also applied. Intraoperative AP and lateral radiographs confirmed excellent reduction, appropriate nail position, and secure locking screw placement. Final limb length and rotation were checked against the contralateral limb and clinical assessment.
Wound Closure:
The incisions were irrigated thoroughly. The soft tissues and skin were closed in layers. A sterile dressing was applied.
Post-Operative Protocol & Rehabilitation
Immediate Post-operative Period (Days 0-7):
*
Pain Management:
Multimodal analgesia was initiated, including opioid narcotics (initially IV, then oral), NSAIDs (if no contraindications), and acetaminophen. A regional nerve block (femoral nerve block) was considered pre-operatively but not performed due to the patient's baseline neurological status and potential confounding of motor assessment.
*
Neurovascular Monitoring:
Hourly neurovascular checks for the first 24 hours, then every 4 hours, to monitor for any signs of compartment syndrome or vascular compromise.
*
Early Mobilization:
The patient was encouraged to begin assisted transfers from bed to wheelchair on post-operative day 1, with strict touch-down weight-bearing on the injured limb. Caregivers were instructed on appropriate transfer techniques to minimize stress on the fracture site.
*
Physical Therapy (PT) and Occupational Therapy (OT):
Initiated on post-operative day 1.
*
PT Focus:
Gentle passive range of motion of the hip and knee within pain limits, focusing on preventing contractures. Emphasis on maintaining trunk control and upper extremity strength for transfers.
*
OT Focus:
Assessment of adaptive equipment (wheelchair seating, transfer aids) to optimize comfort and function. Caregiver training in safe transfers, hygiene, and positioning to prevent pressure injuries.
*
Spasticity Management:
Baseline anti-spasticity medications were continued. Consideration for botulinum toxin injections to spastic muscles (hamstrings, adductors, gastrocnemius) was made for 4-6 weeks post-op if spasticity remained a significant impediment to rehabilitation.
Intermediate Rehabilitation (Weeks 1-6):
*
Weight-Bearing Progression:
Progressed to protected weight-bearing (e.g., using a platform walker or assisted stander) as tolerated, with emphasis on pain as a guide. For a GMFCS Level IV patient, the goal is often pain-free seated tolerance and safe transfers, rather than independent ambulation.
*
Range of Motion:
Continued passive and gentle active-assisted range of motion exercises for the hip and knee, aiming to restore pre-injury baseline ROM and prevent new contractures. Custom-molded ankle-foot orthoses (AFOs) or knee-ankle-foot orthoses (KAFOs) might be utilized to maintain range, especially at night.
*
Strengthening:
Focus on core stability and upper extremity strengthening for assisted transfers and wheelchair propulsion.
*
Caregiver Education:
Reinforcement of proper positioning, skin care, and transfer techniques. Education on signs of potential complications (infection, implant loosening, pressure sores).
Long-term Rehabilitation (Months 2-6 and beyond):
*
Radiographic Follow-up:
Regular radiographic evaluation (e.g., at 6 weeks, 3 months, 6 months) to monitor fracture healing and alignment.
*
Full Weight-Bearing:
Progression to full weight-bearing on the affected limb was guided by radiographic evidence of union and patient comfort. For a GMFCS IV patient, this primarily meant full weight-bearing in assisted standing or during transfers, and comfortable sitting.
*
Spasticity Re-evaluation:
Ongoing assessment of spasticity and its impact on function. Consideration of further interventions such as botulinum toxin, oral medications, or intrathecal baclofen pump if spasticity significantly impedes care or causes pain.
*
Bone Health:
Continue vitamin D and calcium supplementation. Re-evaluate bone density with DEXA scan at 6-12 months post-fracture, and consider bisphosphonate therapy if severe osteopenia persists.
*
Implant Removal:
Discussion regarding implant removal will occur once fracture union is solid, typically 12-18 months post-surgery, especially if symptomatic or if the hardware causes soft tissue irritation or limits growth potential. For this GMFCS IV patient, given the high risk of refracture and poor bone quality, definitive implant removal might be deferred or never undertaken unless clinically indicated.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
*
GMFCS is paramount:
The patient's GMFCS level is the single most important factor in guiding treatment goals, surgical choice, and rehabilitation strategy for children with CP. For GMFCS Level IV/V, goals prioritize pain relief, ease of care, and maintenance of functional positioning over independent ambulation.
*
Stable fixation is crucial:
Due to high spasticity, osteopenia, and challenges with cast care, surgical stabilization (often IMN or plating) is usually preferred over non-operative management for femur fractures in children with CP. Robust fixation counters spasticity-induced forces.
*
Anticipate poor bone quality:
Osteopenia is common in CP patients due to immobility, malnutrition, and medications. This necessitates careful surgical technique, selection of implants with good bone purchase, and consideration of larger diameter nails or alternative fixation constructs (e.g., locked plating) if IMN is not feasible. Be prepared for less reliable screw purchase.
*
Multidisciplinary Approach:
Successful management requires a team including orthopedic surgeons, neuro pediatricians, physical therapists, occupational therapists, pain specialists, and social workers to address the complex needs of these patients and their families.
*
Proximal Femoral Morphology:
Be aware of the often-abnormal proximal femoral anatomy (coxa valga/vara, anteversion) in CP patients when planning IMN entry points and trajectories. Trochanteric entry is generally preferred in younger children to minimize risk of AVN.
*
Rehabilitation is different:
Rehabilitation focuses on maintaining functional transfers, preventing contractures, managing spasticity, and optimizing caregiver burden rather than restoring independent gait. Early mobilization post-fixation is key for preventing deconditioning and pressure injuries.
Pitfalls:
*
Underestimating Spasticity:
Failing to account for the immense, uncoordinated forces generated by spastic musculature can lead to implant failure, loss of reduction, or delayed union. Adequate fixation is essential.
*
Overestimating Bone Healing/Quality:
Assuming standard healing times or bone strength can lead to premature weight-bearing, refracture, or nonunion. Prolonged protection and careful monitoring are necessary.
*
Inadequate Fixation Choice:
Selecting implants that are not robust enough for the patient's GMFCS level and bone quality (e.g., TENS for a comminuted fracture in a GMFCS IV patient with osteopenia) can result in fixation failure.
*
Neglecting Caregiver Burden:
Post-operative protocols that are too demanding or impractical for caregivers can lead to non-compliance, patient discomfort, and secondary complications. Caregiver education and support are vital.
*
Poor Pain Control:
Inadequate post-operative pain management in a patient who may struggle to verbalize pain can hinder rehabilitation and exacerbate spasticity. Multimodal analgesia is critical.
*
Iatrogenic Injury:
Risk of AVN with piriformis entry in skeletally immature patients. Careful guidewire placement and nail insertion are needed to avoid breaching physes or causing iatrogenic fracture.
*
Ignoring Pre-existing Deformities:
Failure to recognize and account for pre-existing rotational or angular deformities from CP can result in a functionally malaligned limb despite fracture union. Careful pre-operative templating and intraoperative checks are crucial.
*
Not Addressing Osteopenia:
Failing to investigate and treat underlying osteopenia (e.g., Vitamin D deficiency, bisphosphonate consideration) increases the risk of refracture and delayed union.
You Might Also Like