Humerus Fractures: Surgical Anatomy, Epidemiology, & Management

Key Takeaway
Humerus fractures are injuries affecting the proximal, diaphyseal, or distal humerus, with varying epidemiology. Effective management requires understanding the surgical anatomy, including critical neurovascular structures like the axillary and radial nerves, and biomechanics of each region to restore function and minimize long-term disability.
Introduction & Epidemiology
Humerus fractures encompass a broad spectrum of injuries affecting the proximal metaphysis, diaphysis, and distal metaphysis/epiphysis, each presenting unique diagnostic and therapeutic challenges. These fractures are among the most common long bone fractures, exhibiting a bimodal age distribution. Proximal humerus fractures are predominantly observed in older adults, particularly postmenopausal women, often in the setting of osteoporotic bone, typically resulting from low-energy falls. Conversely, diaphyseal and distal humerus fractures show a higher incidence in younger, active individuals due to high-energy trauma, such as motor vehicle accidents or sports injuries. Distal humerus fractures can also affect older osteoporotic patients from low-energy mechanisms.
Epidemiologically, proximal humerus fractures account for approximately 5-6% of all fractures in adults, with an incidence of about 70 per 100,000 person-years, rising dramatically with age. Diaphyseal humerus fractures represent 1-3% of all fractures, with a reported incidence of 10-15 per 100,000 person-years. Distal humerus fractures are less common, comprising about 2% of all adult fractures, but present significant morbidity due to the complex anatomy of the elbow joint.
The primary objective in managing humerus fractures is the restoration of anatomical alignment, stability, and subsequently, functional integrity of the upper extremity, minimizing pain and preventing long-term disability. This necessitates a thorough understanding of the specific fracture morphology, patient physiology, and appropriate application of non-operative or operative treatment modalities.
Surgical Anatomy & Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the humerus is paramount for effective fracture management. The humerus, serving as the bridge between the shoulder and elbow joints, interacts with numerous critical neurovascular structures and musculotendinous units throughout its length.
Proximal Humerus
The proximal humerus consists of the humeral head, anatomical neck, surgical neck, greater tuberosity, and lesser tuberosity.
*
Humeral Head:
Articulates with the glenoid, forming the glenohumeral joint. Its articular cartilage covers approximately one-third of a sphere.
*
Tuberosities:
The greater tuberosity serves as the insertion site for the supraspinatus, infraspinatus, and teres minor tendons. The lesser tuberosity is the insertion for the subscapularis. Together, these form the rotator cuff, crucial for shoulder stability and motion.
*
Surgical Neck:
Located distal to the tuberosities, it is a common site for fractures due to its relatively narrow cross-section. The axillary nerve and posterior circumflex humeral artery are in close proximity, coursing around the surgical neck, approximately 5-7 cm distal to the acromion.
*
Blood Supply:
The vascularity of the humeral head is predominantly supplied by branches of the anterior and posterior circumflex humeral arteries. The arcuate artery, a branch of the anterior circumflex humeral artery, ascends within the bicipital groove and supplies the superior and anterior aspects of the humeral head. The posterior circumflex humeral artery supplies the posterior and inferior aspects. Disruption of this vascular supply, particularly in multi-part fractures involving the anatomical neck and tuberosities, significantly increases the risk of avascular necrosis (AVN) of the humeral head.
*
Biomechanics:
The rotator cuff muscles exert significant forces on the tuberosities, and their integrity is critical for active shoulder motion. Deltoid muscle contraction can also contribute to fracture displacement. The Neer classification system categorizes proximal humerus fractures based on the number of displaced "parts" (humeral head, greater tuberosity, lesser tuberosity, surgical neck fragment) and the degree of displacement (>1 cm or >45 degrees angulation). This classification guides treatment decisions, particularly regarding AVN risk.
Humeral Diaphysis
The humeral diaphysis extends from the surgical neck proximally to the supracondylar ridges distally.
*
Anatomy:
It is a cylindrical bone, with a triangular cross-section proximally and flattening distally. Key landmarks include the deltoid tuberosity (insertion of the deltoid muscle) and the spiral (radial) groove.
*
Muscle Attachments:
The deltoid muscle inserts proximally. The pectoralis major, latissimus dorsi, and teres major insert onto the bicipital groove and medial lip. The triceps brachii originates posteriorly. The brachialis muscle attaches to the anterior surface of the distal half of the diaphysis.
*
Radial Nerve:
The radial nerve is the most critical structure in proximity to the humeral diaphysis, coursing posterolaterally within the spiral groove. It is intimately associated with the bone, particularly in the middle and distal third, rendering it vulnerable to injury during fracture or surgical intervention. Its branches innervate the extensor compartment of the forearm.
*
Biomechanics:
The diaphysis is subjected to bending, torsional, and axial loads. Fracture patterns include transverse, oblique, spiral, and comminuted, reflecting the mechanism of injury. Muscle forces, particularly from the deltoid and pectoralis major, can cause characteristic displacement patterns depending on the fracture level.
Distal Humerus
The distal humerus forms the elbow joint, a complex hinge joint that permits flexion, extension, pronation, and supination.
*
Anatomy:
Comprises the medial and lateral epicondyles, supracondylar ridges, capitellum (articulates with radial head), trochlea (articulates with olecranon), coronoid fossa, and olecranon fossa.
*
Articular Surface:
The trochlea and capitellum form a congruent articular surface vital for elbow function.
*
Nerve Proximity:
The ulnar nerve passes posteriorly in the cubital tunnel, behind the medial epicondyle, making it highly susceptible to injury during distal humerus fractures or surgical exposure. The median nerve and radial nerve are also in proximity, anterior to the joint.
*
Muscle Attachments:
The common flexor-pronator origin is on the medial epicondyle, and the common extensor-supinator origin is on the lateral epicondyle.
*
Biomechanics:
The distal humerus acts as a bony buttress for the elbow joint. Intra-articular fractures are common, particularly in high-energy trauma, often resulting in comminuted and displaced fragments that severely compromise joint mechanics. The AO/OTA classification provides a comprehensive system for describing these fractures, distinguishing between extra-articular, partial articular, and complete articular types.
Bone Quality Considerations
Bone quality significantly influences fracture pattern and surgical strategy. Osteoporosis leads to weaker bone, often resulting in comminuted fractures with poor screw purchase, making fixation challenging. Conversely, high-energy trauma in robust bone can result in complex fracture configurations requiring robust internal fixation.
Indications & Contraindications
The decision-making process for humerus fractures involves a careful assessment of patient-specific factors, fracture characteristics, and potential risks versus benefits of operative versus non-operative management.
General Principles
- Patient Factors: Age, functional demands, medical comorbidities, cognitive status, bone quality, compliance with rehabilitation.
- Fracture Factors: Location (proximal, diaphyseal, distal), pattern (simple, comminuted, segmental, spiral), displacement, angulation, rotation, open vs. closed, associated neurovascular injury.
- Soft Tissue Envelope: Condition of the overlying skin and soft tissues.
Non-Operative Indications
Non-operative management aims to achieve acceptable functional outcomes through immobilization and protected early motion, relying on secondary bone healing.
-
Proximal Humerus Fractures:
- Minimally displaced two-part fractures (surgical neck, tuberosity) in most patients.
- Stable three-part fractures in elderly, low-demand patients with acceptable alignment.
- Impacted valgus fractures where stability is maintained.
- Acceptable alignment typically defined as <45° angulation, <1 cm displacement, and no significant head-shaft dissociation.
-
Humeral Diaphyseal Fractures:
- Closed fractures with acceptable alignment.
- Acceptable alignment criteria are generally <20° anterior angulation, <30° varus/valgus angulation, <3 cm shortening, and less than 15-20° rotational malalignment. These values are often more permissive than for lower extremity long bones.
- Fractures with radial nerve palsy that recovers spontaneously (often observed for 3-6 months).
- Patients with significant comorbidities precluding surgery.
-
Distal Humerus Fractures:
- Minimally displaced extra-articular fractures (supracondylar) in selected, very low-demand elderly patients or those unfit for surgery.
- Rarely, stable pediatric supracondylar fractures (though often pinned).
- Acceptable alignment here is more stringent due to critical elbow function, usually <10-15° angulation.
Operative Indications
Operative intervention aims to achieve anatomical reduction and stable internal fixation, facilitating early motion and optimizing functional recovery, particularly for displaced, unstable, or complex fracture patterns.
-
Proximal Humerus Fractures:
- Displaced three- and four-part fractures in active patients.
- Displaced surgical neck fractures with significant angulation/shortening, particularly if irreducible by closed means.
- Head-splitting fractures.
- Open fractures.
- Fracture-dislocations.
- Nonunion or symptomatic malunion.
- Vascular injury requiring exploration.
- Young, active patients with significant displacement.
-
Humeral Diaphyseal Fractures:
- Open fractures.
- Segmental fractures.
- Polytrauma patients requiring stabilization for early mobilization.
- Vascular injury requiring repair.
- Pathologic fractures (may require adjuvant treatment).
- Radial nerve palsy associated with an open fracture or that fails to recover within 3-6 months.
- Fractures associated with brachial plexus injury.
- Interposition of soft tissue preventing closed reduction.
- Progressive displacement or inability to maintain acceptable alignment with non-operative treatment.
- Nonunion or symptomatic malunion.
-
Distal Humerus Fractures:
- All displaced intra-articular fractures.
- Significantly displaced extra-articular fractures where anatomical alignment is critical for elbow function.
- Open fractures.
- Fracture-dislocations of the elbow.
- Associated neurovascular injury.
- Nonunion or symptomatic malunion.
Contraindications
-
Absolute Contraindications:
- Active infection (unless it's an open fracture with aggressive debridement).
- Poor soft tissue envelope precluding safe surgical incision and closure.
- Patient medically unfit for anesthesia and surgery (ASA class IV/V, unstable vital signs).
-
Relative Contraindications:
- Severe osteoporosis with inadequate bone stock for rigid fixation (may necessitate arthroplasty for proximal humerus or modified fixation).
- Pre-existing neurological deficits or severe comorbidities that limit expected functional improvement.
Summary Table: Operative vs. Non-Operative Indications
| Fracture Type | Non-Operative Indications | Operative Indications |
|---|---|---|
| Proximal Humerus | - Minimally displaced 2-part fractures (<1cm, <45°) | - Displaced 3- or 4-part fractures |
| - Stable impacted valgus fractures | - Head-splitting fractures | |
| - Low-demand elderly patients with acceptable alignment | - Fracture-dislocations | |
| - Open fractures | ||
| - Vascular injury | ||
| - Failure of non-operative treatment | ||
| Humeral Diaphysis | - Closed fractures with acceptable alignment (<20° ant, | - Open fractures |
| <30° varus/valgus, <3cm shortening) | - Segmental fractures | |
| - Radial nerve palsy without vascular injury (observation) | - Polytrauma requiring early mobilization | |
| - Patient medically unfit for surgery | - Vascular injury requiring repair | |
| - Radial nerve palsy with open fracture or persistent | ||
| deficit >3-6 months | ||
| - Inability to achieve/maintain acceptable reduction | ||
| - Nonunion/malunion | ||
| Distal Humerus | - Minimally displaced extra-articular fractures | - All displaced intra-articular fractures |
| (rare, selected low-demand patients) | - Significantly displaced extra-articular fractures | |
| - Open fractures | ||
| - Fracture-dislocations | ||
| - Associated neurovascular injury | ||
| - Nonunion/malunion |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical to anticipating challenges and ensuring a successful outcome. This encompasses comprehensive patient assessment, detailed imaging review, implant selection, and precise surgical positioning.
Pre-Operative Planning
-
Clinical Assessment:
- Detailed history of injury mechanism, timing, and associated symptoms.
- Thorough neurovascular examination, documenting any pre-existing deficits. This is crucial for distinguishing pre-operative vs. iatrogenic injury.
- Assessment of soft tissue status, particularly for open fractures or significant swelling.
- Evaluation of comorbidities, anesthetic risk, and patient's functional demands.
-
Imaging Review:
- Plain Radiographs: Standard orthogonal views (AP, lateral) are essential. For proximal humerus, axillary and Neer trauma series (AP, scapular Y, axillary lateral) are critical. For distal humerus, oblique views may be helpful.
- Computed Tomography (CT) Scan: Indispensable for complex fractures, particularly intra-articular proximal or distal humerus fractures. 3D reconstructions are invaluable for understanding fracture morphology, articular involvement, and comminution, aiding in surgical approach and implant selection. CT angiography may be indicated if vascular injury is suspected.
- Magnetic Resonance Imaging (MRI): Rarely used acutely for fracture assessment, but can be helpful for concomitant ligamentous injuries, rotator cuff tears, or pre-existing avascular necrosis if suspected.
-
Implant Selection & Strategy:
- Proximal Humerus: Locking plates (e.g., PHILOS plate systems) are the most common. Considerations include plate length, number of locking screws (particularly calcar screws), and use of sutures for tuberosity repair. Intramedullary nails (IMN) are less common but an option for selected two-part surgical neck fractures. Hemiarthroplasty or reverse total shoulder arthroplasty (RTSA) are options for unreconstructible fractures, particularly in older patients with poor bone quality and high AVN risk.
- Diaphyseal Humerus: Open reduction and internal fixation (ORIF) with a locking compression plate (LCP) is a standard. IMN (antegrade or retrograde) is an alternative, particularly for comminuted fractures or segmental defects. External fixation for temporary stabilization in severe open injuries.
- Distal Humerus: Bicolumnar plating (medial and lateral plates, typically orthogonal or parallel) is the standard for complex intra-articular fractures. Precontoured plates are often used. Fragment-specific plating may be required.
- Surgical Plan: Detailed step-by-step plan including chosen surgical approach, reduction maneuvers, fixation strategy, nerve and vessel protection, and contingency plans for unexpected findings or complications. Draw the fracture and planned implant on templates.
Patient Positioning
Proper patient positioning is paramount for surgical access, nerve protection, and intra-operative fluoroscopy utilization.
-
Proximal Humerus Fractures:
- Beach Chair Position: Most common. Allows good access to the anterior and lateral shoulder. The patient is semi-recumbent, with the torso elevated 30-70 degrees. The head is secured. The affected arm is prepped free to the hand, allowing manipulation. A bump is placed under the ipsilateral scapula to protract it. Fluoroscopy access for AP and axillary views is essential.
- Supine Position: Less common but may be used with a chest bolster. Allows for easier access for potential conversion to arthroplasty, and sometimes preferred for large patients.
- Key Considerations: Ensure axillary nerve is protected. Avoid excessive traction that could injure the brachial plexus.
-
Humeral Diaphyseal Fractures:
- Supine Position: For anterolateral or deltopectoral approaches (proximal to mid-shaft). The arm is draped free. Fluoroscopy C-arm can obtain AP and lateral views.
- Lateral Decubitus Position: For posterior or posterolateral approaches (mid to distal shaft). The patient is placed on the unaffected side. The affected arm is prepped free and supported on a padded arm board or elevated on a bolster.
- Key Considerations: Meticulous padding of all pressure points. The radial nerve is at critical risk; confirm its expected anatomical location based on the approach.
-
Distal Humerus Fractures:
- Lateral Decubitus Position: Most common for posterior approaches with the arm draped over a chest roll or supported on a padded arm table, allowing for 90-120 degrees of elbow flexion. This facilitates the posterior approach and use of fluoroscopy for true lateral views.
- Prone Position: An alternative for posterior approaches, especially for very distal or comminuted fractures, but can be less ergonomic for the surgeon.
- Supine Position: Less common for complex distal humerus fractures but can be used for medial or lateral epicondylar fractures or simple supracondylar fractures via direct approaches.
- Key Considerations: Protect the ulnar nerve throughout positioning and exposure. Ensure the elbow joint can be fully manipulated and fluoroscopy can obtain true AP and lateral views.
Detailed Surgical Approach / Technique
The choice of surgical approach and technique is dictated by the fracture pattern, location, associated injuries, and surgeon preference. Precision in dissection, reduction, and fixation is paramount to optimize outcomes and minimize complications.
Proximal Humerus Fractures: Open Reduction Internal Fixation (ORIF) with Locking Plate
This technique is commonly employed for displaced 2-, 3-, and 4-part proximal humerus fractures in patients suitable for osteosynthesis.
-
Surgical Approach:
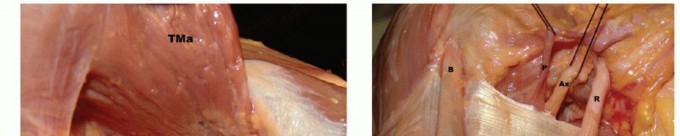
- Deltopectoral Approach: The most common approach. An incision is made from the coracoid process, extending distally along the deltopectoral groove for 10-15 cm. The internervous plane is between the deltoid (axillary nerve) laterally and the pectoralis major (medial and lateral pectoral nerves) medially. The cephalic vein is identified and typically retracted laterally with the deltoid.
- Dissection: The clavipectoral fascia is incised. The conjoined tendon (coracobrachialis and short head of biceps) is identified and protected medially. The anterior circumflex humeral artery and its branches supplying the humeral head are carefully preserved if possible, but often disrupted by the fracture. The axillary nerve, located 5-7 cm distal to the acromion, must be identified or its location estimated and protected during plate application and screw insertion.
-
Fracture Reduction:
- Indirect Reduction: Initial traction on the extremity can help achieve ligamentotaxis. Gentle manipulation of the arm, often with an assistant, can help align the humeral shaft.
- Direct Reduction: Periosteal elevators, joysticks (K-wires inserted into fragments), or sutures passed through the rotator cuff tendons can be used to manipulate and reduce the humeral head and tuberosity fragments. Restore the articular surface alignment and height. A key maneuver is reduction of the tuberosities to the humeral head and then the entire complex to the shaft.
- Temporary Fixation: K-wires are often used to temporarily secure fragments (e.g., tuberosities to the head, or the head-tuberosity block to the shaft).
-
Plate Application and Fixation:
- Plate Selection: A precontoured locking plate (e.g., PHILOS plate) is chosen. The plate should sit slightly lateral to the bicipital groove and proximal enough to capture sufficient humeral head fragments without impinging on the acromion or rotator cuff.
- Plate Position: Position the plate on the lateral aspect of the shaft, approximately 5-8 mm distal to the superior border of the greater tuberosity. Ensure it does not impinge on the subacromial space.
- Shaft Fixation: Secure the plate to the humeral shaft with cortical screws initially, often utilizing a compression screw hole if desired to achieve slight compression at the fracture site (if a transverse component exists). Locking screws are then placed distally to provide angular stability. At least 3-4 bicortical screws are generally recommended for shaft fixation.
- Head Fixation: Insert locking screws into the humeral head. Aim for divergent screw trajectories to maximize purchase and create a "calcar support" effect by directing screws into the inferomedial aspect of the humeral head fragment. The goal is at least 3-5 divergent locking screws into the head. Suture fixation through the rotator cuff tendons (supraspinatus, subscapularis) to plate eyelets is often used to augment tuberosity stability and improve healing.
- Final Assessment: Confirm reduction and fixation stability under fluoroscopy in multiple planes (AP, axillary, Y-view). Check for hardware prominence and smooth range of motion.
Humeral Diaphyseal Fractures: Plating vs. Intramedullary Nailing
A. Open Reduction Internal Fixation (ORIF) with Plate
-
Surgical Approach:
- Anterolateral Approach (Henry Approach): Suitable for proximal and mid-shaft fractures. Incision along the anterior border of the deltoid, extending distally. The internervous plane is between the deltoid (axillary nerve) proximally and biceps/brachialis (musculocutaneous nerve) medially, and the triceps (radial nerve) laterally. The radial nerve is identified in the spiral groove, typically anterior to the lateral head of the triceps, and meticulously protected.
-
Posterior Approach (Thompson or Triceps-Sparing):
Suitable for mid to distal shaft fractures. Incision centered posteriorly.
- Triceps-splitting: Directly through the triceps muscle.
- Triceps-sparing: Between the long and lateral heads of the triceps (proximal) or medial and lateral heads (distal). The radial nerve must be identified proximally as it pierces the lateral intermuscular septum and followed distally within the spiral groove until it exits anteriorly.
- Dissection: Careful hemostasis. Blunt dissection to expose the fracture site.
-
Fracture Reduction:
- Achieve anatomical or near-anatomical reduction using traction, direct manipulation with bone clamps (e.g., Verbrugge, pointed reduction clamps), or joystick K-wires.
- For oblique or spiral fractures, lag screws can be inserted first, perpendicular to the fracture plane, to achieve interfragmentary compression.
-
Plate Application and Fixation:
- Plate Selection: A locking compression plate (LCP) or dynamic compression plate (DCP) of appropriate length is chosen. It should bridge at least 2-3 cortical diameters proximal and distal to the fracture.
- Application: Position the plate on the tension side (e.g., anterolateral for bending stability). Secure the plate to one main fragment, then reduce the other fragment to the plate using a push-pull device or bone clamps.
- Screw Insertion: Insert cortical screws first, often in compression mode (eccentric drilling) if a simple fracture pattern, to achieve primary bone healing. Then insert locking screws for angular stability, particularly in comminuted or osteoporotic fractures. Ensure at least 6 cortices of screw fixation on each side of the fracture.
- Radial Nerve: During plating, the radial nerve is identified and protected with a vessel loop or rubber sling throughout the procedure. Ensure no screws impinge on or are placed near the nerve.
- Final Assessment: Confirm reduction and fixation stability with fluoroscopy.
B. Intramedullary Nailing (IMN)
Indicated for some transverse, oblique, or comminuted diaphyseal fractures, especially in polytrauma settings.
- Patient Position: Often supine or beach chair for antegrade nailing, lateral decubitus for retrograde.
-
Entry Portal:
- Antegrade Nailing: Piriformis fossa (apex of greater tuberosity) or slightly medial to the greater tuberosity. Care is taken to avoid iatrogenic rotator cuff injury. The deltoid is split.
- Retrograde Nailing: Through the olecranon fossa or just proximal to the trochlea, with the elbow flexed.
- Reaming/Nail Insertion: Reaming may be performed to allow for a larger diameter nail, or an unreamed nail can be used. The nail is carefully advanced across the fracture site.
- Interlocking Screws: Proximal and distal interlocking screws are placed under fluoroscopic guidance to prevent rotational instability and axial collapse.
- Radial Nerve: While less common than with plating, iatrogenic radial nerve injury can occur during IMN insertion or interlocking screw placement, particularly for retrograde nails.
Distal Humerus Fractures: Bicolumnar Plating
This is the gold standard for displaced, intra-articular distal humerus fractures.
-
Surgical Approach:
-
Posterior Approach with Olecranon Osteotomy:
Most common and provides excellent exposure of the distal humerus and articular surface.
- Incision: Posterior midline incision centered over the olecranon.
- Ulnar Nerve: The ulnar nerve is identified proximal to the cubital tunnel, carefully mobilized, neurolyzed, and transposed anteriorly to protect it throughout the procedure.
- Olecranon Osteotomy: A chevron or transverse osteotomy is performed in the olecranon, preserving the triceps insertion. A pre-drilled hole for a future lag screw or plate is made prior to osteotomy.
- Dissection: The triceps is elevated subperiosteally to expose the distal humerus. The fracture fragments, including the articular block, are fully exposed.
- Triceps-Sparing Approaches: (e.g., Paratricipital or Triceps-Reflecting Anconeus Pedicle (TRAP) approach): Can be used for less complex fractures, avoiding an osteotomy, but provide more limited exposure.
-
Posterior Approach with Olecranon Osteotomy:
Most common and provides excellent exposure of the distal humerus and articular surface.
-
Fracture Reduction:
- Articular Reconstruction First: The primary goal is anatomical restoration of the articular surface. The trochlea and capitellum fragments are reduced to each other and temporarily fixed with K-wires.
- Metaphyseal-Articular Reduction: Once the articular block is reconstructed, it is then reduced to the humeral shaft. This often involves traction, direct manipulation, and use of bone clamps.
-
Plate Application and Fixation (Bicolumnar):
- Columnar Fixation: The distal humerus is conceptualized as medial and lateral columns. Fixation involves two plates, typically placed orthogonal (90/90) or parallel to each other, engaging both columns.
- Medial Plate: Applied along the medial supracondylar ridge.
- Lateral Plate: Applied along the lateral supracondylar ridge.
- Screw Trajectories: Screws from each plate should engage the opposing column's fragments, creating a stable interlocking construct. Locking screws provide angular stability in the osteoporotic or comminuted bone. Interfragmentary lag screws are used to compress simple articular or metaphyseal fragments.
- Stable Construct: The goal is a rigid construct allowing for early range of motion.
-
Olecranon Osteotomy Fixation:
- Once the distal humerus fixation is complete, the olecranon osteotomy is rigidly fixed, typically with a tension band wire construct or an olecranon plate, ensuring a smooth articular surface.
- Ulnar Nerve: The ulnar nerve is relocated to its native position or placed subcutaneously in an anterior transposition.
- Final Assessment: Evaluate elbow stability and range of motion through the full arc. Confirm reduction and hardware position with fluoroscopy.
Complications & Management
Humerus fractures and their surgical treatment are associated with a range of potential complications, necessitating proactive prevention and timely management.
General Complications
- Infection: Superficial (cellulitis) or deep (osteomyelitis). Incidence varies but generally 1-5%. Managed with antibiotics for superficial, and surgical debridement, antibiotics, and possible hardware removal/exchange for deep.
- Wound Dehiscence: Often due to excessive tension or poor soft tissue handling. Managed with local wound care, skin grafting, or flap coverage as needed.
- Neurovascular Injury: Iatrogenic injury to nerves or vessels during exposure or fixation. Radial nerve is particularly vulnerable in diaphyseal fractures, ulnar nerve in distal. Management involves immediate exploration and repair if detected intraoperatively, or observation with delayed exploration if no recovery.
- Malunion: Healing in a suboptimal position (angulation, rotation, shortening). Can lead to pain, stiffness, or cosmetic deformity. Corrective osteotomy may be indicated for symptomatic malunion, especially in the diaphysis.
- Nonunion: Failure of the fracture to heal after an appropriate period (typically 6-9 months). Incidence is variable, influenced by fracture type, comminution, soft tissue compromise, and patient factors (smoking, NSAIDs). Managed with revision ORIF, bone grafting (autograft or allograft), and often a more rigid fixation construct. Electrical stimulation may be an adjunct.
- Hardware Failure: Breakage or loosening of implants, often secondary to nonunion or excessive stress on an unstable construct. Requires revision surgery.
Proximal Humerus Specific Complications
-
Avascular Necrosis (AVN) of the Humeral Head:
Incidence can be high (up to 30-40% in 4-part fractures), especially if vascular supply is disrupted. Leads to pain, collapse, and arthritis.
- Management: For early/mild AVN, conservative management with activity modification and pain control. For progressive collapse or severe pain, surgical options include hemiarthroplasty or reverse total shoulder arthroplasty (RTSA).
-
Stiffness/Loss of Motion:
Common, especially in older patients. Can result from prolonged immobilization, rotator cuff scarring, or heterotopic ossification.
- Management: Aggressive physical therapy, manipulation under anesthesia, arthroscopic or open arthrolysis for recalcitrant cases.
-
Rotator Cuff Impingement/Tear:
Can occur due to hardware prominence or secondary to tuberosity malunion/nonunion.
- Management: Hardware removal, rotator cuff repair.
-
Hardware Prominence:
Plate or screw heads can impinge on subacromial structures or cause skin irritation.
- Management: Symptomatic hardware removal after fracture healing.
Humeral Diaphyseal Specific Complications
-
Radial Nerve Palsy:
Most common associated nerve injury. Up to 20% incidence with primary fracture, 3-5% iatrogenic during surgery. Most primary palsies resolve spontaneously within 3-6 months.
- Management: Observation for spontaneous recovery in closed fractures. Exploration indicated for open fractures, progressively worsening palsy, or failure to recover after 3-6 months (consider nerve grafting or tendon transfer for persistent deficits). Iatrogenic palsies warrant immediate exploration.
-
Nonunion:
Incidence 5-15%, higher with comminution, open fractures, and poor patient compliance.
- Management: Revision ORIF with plate exchange (often larger, longer plate), bone grafting (autograft from iliac crest or synthetic bone graft), and often a reamed IMN if previously plated.
-
Malunion:
Rotational, angular, or shortening deformities. Significant rotational malunion (>20-30°) can cause functional deficits.
- Management: Corrective osteotomy for symptomatic malunion.
Distal Humerus Specific Complications
-
Ulnar Nerve Neuropathy:
Incidence 10-20% due to injury or iatrogenic manipulation/entrapment.
- Management: Pre-emptive neurolysis and anterior transposition during surgery. Post-op symptoms often managed with observation. Surgical exploration and transposition for persistent or worsening symptoms.
-
Elbow Stiffness/Loss of Motion:
Very common due to the complex nature of the joint and potential for heterotopic ossification. Can significantly limit function.
- Management: Aggressive early motion protocols post-operatively. For persistent stiffness, dynamic splinting, manipulation under anesthesia, or arthroscopic/open arthrolysis with capsulectomy and heterotopic ossification excision.
-
Heterotopic Ossification (HO):
Formation of ectopic bone in soft tissues around the elbow, leading to motion restriction. Incidence up to 30-50% in severe trauma.
- Prevention: Post-operative NSAIDs (e.g., indomethacin) for 3-6 weeks, or single-dose radiation therapy (7-8 Gy) within 72 hours of surgery, especially for high-risk patients (head injury, burns, open fractures).
- Management: Excision of mature HO after fracture healing and resolution of inflammation, often combined with arthrolysis.
-
Post-traumatic Arthritis:
Can occur in intra-articular fractures despite good reduction, due to cartilage damage, malreduction, or altered joint mechanics.
- Management: Activity modification, NSAIDs, intra-articular injections. For severe symptomatic arthritis, total elbow arthroplasty (TEA) or interposition arthroplasty may be considered in selected patients.
-
Nonunion/Malunion:
Can occur if fixation is unstable or reduction inadequate.
- Management: Revision ORIF with more rigid fixation, bone grafting, or in severe cases, TEA.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Salvage/Management Strategy |
|---|---|---|
| General | ||
| Infection (deep) | 1-5 | Debridement, antibiotics, possible hardware removal/exchange |
| Malunion (symptomatic) | Variable (depends on location/type) | Corrective osteotomy |
| Nonunion | 5-15 (diaphyseal); 5-10 (proximal); 10-15 (distal) | Revision ORIF, bone grafting, IMN exchange, more rigid fixation |
| Hardware Failure | 5-10 (often secondary to nonunion) | Revision ORIF, re-fixation, possible removal |
| Proximal Humerus Specific | ||
| Avascular Necrosis (AVN) | 0-10 (2-part); 10-40 (3-4 part) | Hemiarthroplasty, Reverse Total Shoulder Arthroplasty (RTSA) |
| Stiffness/Loss of Motion | 20-50 | Aggressive PT, manipulation under anesthesia, arthrolysis |
| Hardware Prominence | 10-20 | Symptomatic hardware removal |
| Rotator Cuff Impingement | 5-15 | Hardware removal, rotator cuff repair |
| Diaphyseal Humerus Specific | ||
| Radial Nerve Palsy (primary) | 10-20 (associated with fracture) | Observation (3-6 months); surgical exploration if open fracture/no recovery |
| Radial Nerve Palsy (iatrogenic) | 3-5 (during surgery) | Immediate surgical exploration |
| Distal Humerus Specific | ||
| Ulnar Nerve Neuropathy | 10-20 | Neurolysis, anterior transposition; observation for post-op symptoms, delayed exploration |
| Elbow Stiffness/Loss of Motion | 20-60 | Aggressive PT, dynamic splinting, manipulation under anesthesia, arthrolysis |
| Heterotopic Ossification (HO) | 10-50 (esp. severe trauma) | Prevention (NSAIDs, radiation); surgical excision for symptomatic mature HO |
| Post-traumatic Arthritis | 10-30 | Conservative management; Total Elbow Arthroplasty (TEA) for severe cases |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical intervention itself in achieving optimal functional outcomes. Protocols are tailored to fracture stability, fixation strength, patient compliance, and the specific anatomical region involved. The overarching goals are pain control, restoration of range of motion (ROM), progressive strengthening, and return to functional activities.
General Principles
- Early Protected Motion: Initiated as soon as the stability of fixation allows, to prevent stiffness, promote cartilage health, and facilitate soft tissue healing.
- Pain and Edema Control: Essential for patient comfort and participation in therapy. Includes analgesics, ice, and elevation.
- Progressive Loading: Strength and functional demands are gradually increased over time to allow for bone healing and tissue adaptation.
- Patient Education: Crucial for adherence to the protocol and understanding limitations.
- Supervised Therapy: Regular sessions with a qualified physical therapist are usually necessary.
Phases of Rehabilitation
Phase I: Immobilization and Early Protected Motion (Typically 0-6 weeks)
- Focus: Protect the fracture site, manage pain and swelling, initiate gentle, protected range of motion to prevent stiffness.
-
Proximal Humerus:
- Immobilization: Arm in a sling (e.g., shoulder immobilizer) for 4-6 weeks, removing for hygiene and exercises.
-
Exercises:
- Pendulum (Codman's) Exercises: Gentle, gravity-assisted circular motions of the shoulder, keeping the body bent forward.
- Passive Range of Motion (PROM): Initiated by a therapist within a pain-free arc. Flexion to 90-120°, external rotation to 0-30° (avoiding internal rotation past neutral, which can stress tuberosity repairs).
- Active-Assisted Range of Motion (AAROM): Self-assisted or therapist-assisted movements for flexion, abduction, and rotation within pain-free limits.
- Elbow, Wrist, Hand ROM: Active exercises to maintain mobility of adjacent joints.
- Isometric Exercises: Gentle submaximal isometric exercises for shoulder musculature (deltoid, rotator cuff) may be introduced late in this phase, without resisted motion.
-
Humeral Diaphysis:
- Immobilization: Sling for comfort, particularly if plate fixation allows. For IMN, a sling is often used briefly. Functional bracing may be employed for some non-operative cases.
-
Exercises:
- Active Elbow, Wrist, Hand ROM: Emphasize full extension and flexion of the elbow.
- Gentle Shoulder AAROM/AROM: As pain allows, avoiding excessive stress on the healing shaft.
- Avoid: Lifting, pushing, pulling with the affected arm.
-
Distal Humerus:
- Immobilization: Splint or cast for 1-2 weeks post-operatively, then transition to hinged elbow brace.
-
Exercises:
- CPM (Continuous Passive Motion) Machine: May be initiated immediately if fixation is stable and tolerated, to maintain articular cartilage health and prevent stiffness.
- PROM/AAROM: Elbow flexion/extension within the limits of the brace or as tolerated. Pronation/supination.
- Avoid: Any active lifting or forceful movements.
Phase II: Progressive Active Motion and Light Strengthening (Typically 6-12 weeks)
- Focus: Increase active range of motion, introduce light strengthening exercises, reduce reliance on assistive devices. Bone healing is typically sufficient to allow more aggressive motion.
-
Proximal Humerus:
- Weaning from Sling: Gradually discontinue sling use.
- AROM: Progress full active shoulder flexion, abduction, and rotation.
- Light Strengthening: Initiate isometric and isotonic exercises with light resistance bands or weights for rotator cuff, deltoid, and scapular stabilizers.
- Proprioceptive Exercises: Wall slides, table slides.
-
Humeral Diaphysis:
- AROM: Continue to maximize shoulder and elbow ROM.
- Strengthening: Progressive strengthening of the entire upper extremity, including bicep curls, triceps extensions, shoulder presses with light weights or resistance bands.
- Weight Bearing: Gradually introduce light weight-bearing activities.
-
Distal Humerus:
- AROM: Continue to achieve full elbow flexion, extension, pronation, and supination. Address any persistent ROM deficits.
- Strengthening: Begin gentle, progressive strengthening for elbow flexors and extensors, and forearm muscles.
- Hinged Brace: May continue to use the hinged elbow brace for protection during activities.
Phase III: Advanced Strengthening and Functional Return (Typically 12+ weeks)
- Focus: Maximize strength, endurance, and power. Return to sport or work-specific activities.
-
All Fracture Types:
- Aggressive Strengthening: Progress to heavier weights and higher resistance exercises, incorporating functional movements.
- Endurance Training: Repetitive tasks to build muscle stamina.
- Sport-Specific/Work-Specific Training: Gradually reintroduce activities required for their specific occupation or sport. This may involve plyometrics or impact loading.
- Return to Full Activity: Typically permitted after 4-6 months, depending on fracture consolidation (radiographic evidence of healing) and restoration of strength.
- Addressing Deficits: Continue to address any residual ROM or strength deficits. For recalcitrant stiffness, manipulation under anesthesia or arthrolysis may be considered.
Rehabilitation protocols must be individualized, adapting to the patient's progress, pain levels, and radiographic evidence of fracture healing. Close communication between the surgeon, physical therapist, and patient is essential for a successful recovery.
Summary of Key Literature / Guidelines
The management of humerus fractures is guided by an extensive body of literature, including landmark studies and consensus guidelines.
Proximal Humerus Fractures
- Neer Classification (1970): Remains the most widely used classification system, providing a common language and guiding treatment decisions based on fracture displacement and involvement of the four main segments (anatomical neck, surgical neck, greater tuberosity, lesser tuberosity).
- Non-operative Management: Studies by Constant et al. (1987) and others have demonstrated good outcomes for minimally displaced fractures treated non-operatively with early protected mobilization, particularly in the elderly.
- ORIF with Locking Plates: The introduction of locking plates (e.g., PHILOS, LPHP) has improved fixation stability, particularly in osteoporotic bone, reducing rates of screw cut-out and loss of reduction compared to conventional plating. Studies by Olerud et al. (2010) and Südkamp et al. (2009) have shown favorable outcomes with locking plates, though complications like AVN and stiffness remain.
-
Arthroplasty:
For complex 3- and 4-part fractures, especially in older patients with poor bone quality or high AVN risk, hemiarthroplasty (HA) or reverse total shoulder arthroplasty (RTSA) are often considered.
- CODMAN Trial (2015): A landmark randomized controlled trial comparing ORIF with HA for displaced 3- and 4-part proximal humerus fractures in older adults found no significant difference in functional outcomes, suggesting HA does not offer a clear advantage over ORIF in this specific population.
- RTSA for Fracture: Numerous studies (e.g., Gallinet et al. 2007, Cazeneuve et al. 2013) have highlighted RTSA as a reliable option for unreconstructible fractures in the elderly, offering predictable pain relief and improved active elevation, often superior to HA in this context, especially in older patients with rotator cuff deficiency. Current trends favor RTSA for older, low-demand patients with complex fractures or those with rotator cuff dysfunction.
- Controversies: The optimal treatment for displaced 3- and 4-part fractures, particularly in the elderly, remains a subject of ongoing debate, with patient-specific factors heavily influencing the choice between ORIF, HA, and RTSA.
Humeral Diaphyseal Fractures
- Non-operative Treatment: Historically, functional bracing (Sarmiento brace) has been highly successful, with union rates of 80-90% for closed diaphyseal fractures, as demonstrated by Sarmiento et al. (1990).
- Operative Treatment Indications: Generally reserved for specific indications as outlined in the "Indications & Contraindications" section.
-
Plating vs. Nailing:
- Plating (ORIF): Provides excellent anatomical reduction and stability. Studies by Ring et al. (1999) and McCormack et al. (2000) have shown high union rates (90-95%) with plating. The main concern is radial nerve injury, either iatrogenic or associated with the fracture itself.
- Intramedullary Nailing (IMN): Less soft tissue dissection, potential for faster union in some contexts. Antegrade nailing has been associated with shoulder pain and rotator cuff impingement, while retrograde nailing may have a slightly higher risk of elbow pain. Randomized trials comparing plating and nailing have yielded mixed results, with some favoring plating for lower nonunion rates and fewer complications (e.g., Tingstad et al., 2011), while others show comparable outcomes. IMN is often preferred for segmental fractures or polytrauma.
- Radial Nerve Palsy: Most commonly, associated with primary fracture. Observational management for primary palsy typically results in 70-90% spontaneous recovery (Shafi et al., 2014). Early exploration is indicated for open fractures, neurological deterioration, or lack of recovery after 3-6 months.
Distal Humerus Fractures
- AO/OTA Classification: Standard for describing distal humerus fractures (type A: extra-articular; type B: partial articular; type C: complete articular), which strongly dictates treatment strategy.
- Anatomical Reduction and Stable Fixation: Key principles for displaced intra-articular fractures. Studies by Gruen et al. (1995) and Sanchez-Sotelo et al. (2000) have emphasized the importance of anatomical reduction of the articular surface and a stable bicolumnar plate fixation construct.
- Bicolumnar Plating: The standard technique, often using precontoured locking plates. Orthogonal (90/90) plating constructs are widely used, providing strong biomechanical stability by placing plates on the medial and posterolateral columns (Colton, 1987; O'Driscoll, 2000). Parallel plating constructs have also shown good results.
- Olecranon Osteotomy vs. Triceps-Sparing: While olecranon osteotomy provides excellent exposure for complex intra-articular fractures, studies have explored triceps-sparing approaches to minimize osteotomy-related complications. However, for highly comminuted articular fractures, the superior visualization offered by an osteotomy often outweighs its inherent risks.
- Ulnar Nerve Management: Prophylactic ulnar nerve transposition, particularly anterior transposition, is a common practice during distal humerus ORIF to prevent post-operative neuropathy, as supported by various series (e.g., Ring et al., 2004).
- Early Motion: Critical for preventing stiffness. The stability of modern bicolumnar plating allows for early initiation of passive and active-assisted range of motion.
The evolving understanding of biomechanics, implant technology, and surgical techniques continues to refine best practices for humerus fracture management. Staying abreast of current literature and guidelines is essential for all orthopedic surgeons.
You Might Also Like