Humerus Fractures: A Comprehensive Surgical Review for Orthopedic Professionals
Key Takeaway
Surgical management of humerus fractures involves understanding distinct epidemiological patterns, biomechanics, and specific anatomical considerations for proximal, diaphyseal, and distal types. A comprehensive review emphasizes critical surgical anatomy, particularly nerve and vascular structures, along with operative indications, techniques, and potential complications, guiding orthopedic surgeons in evidence-based care.
Fractures of the Humerus: A Comprehensive Surgical Review
Introduction & Epidemiology
Humerus fractures constitute a significant burden within orthopedic trauma, representing approximately 3% to 5% of all adult fractures. These injuries are broadly categorized by anatomical location: proximal, diaphyseal, and distal, each with distinct epidemiological patterns, biomechanical considerations, and management strategies.
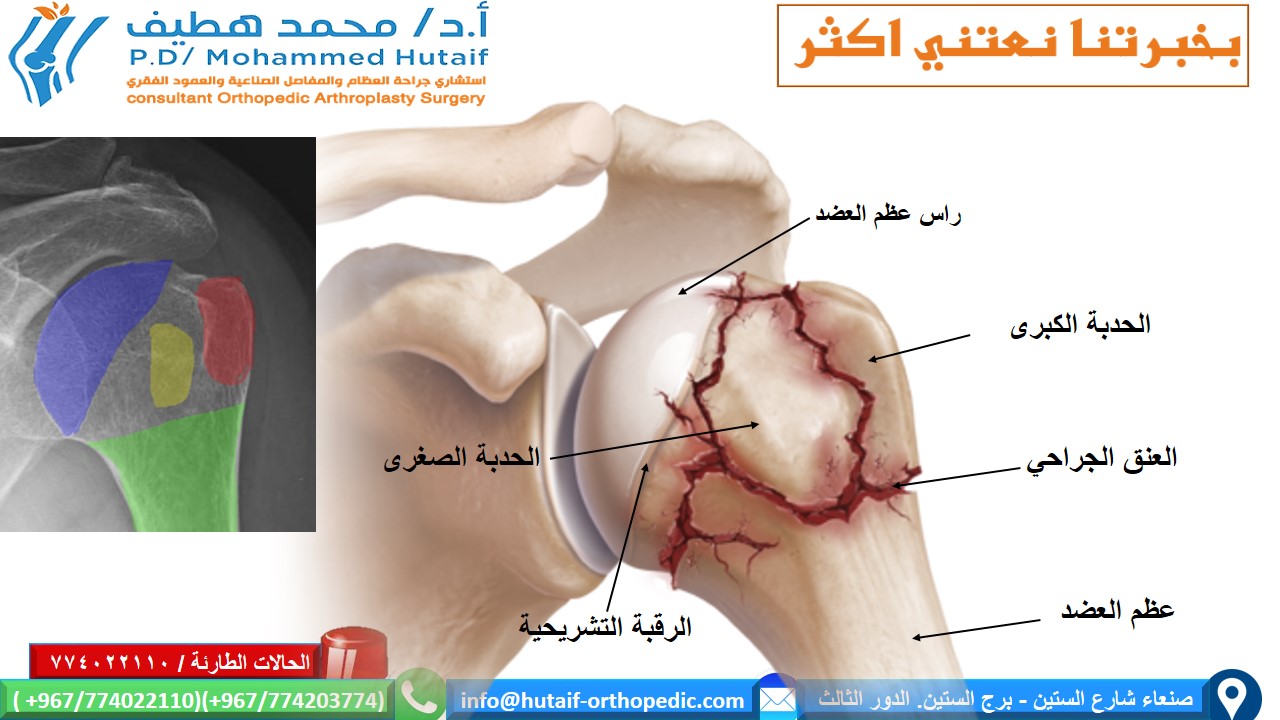
Proximal Humerus Fractures: These are common, accounting for 4-5% of all fractures and 45% of all humerus fractures, with a bimodal distribution. In younger patients, they typically result from high-energy trauma, while in the elderly, they are often low-energy falls in osteoporotic bone. Women are affected more frequently than men, with an increasing incidence correlating with age and osteoporosis. The Neer classification system, based on the displacement of four major segments (humeral head, greater tuberosity, lesser tuberosity, and humeral shaft), remains a widely adopted tool for guiding treatment decisions.
Humeral Diaphyseal Fractures: These fractures represent 1-3% of all fractures, with a similar bimodal distribution. High-energy mechanisms (e.g., motor vehicle accidents) are common in younger individuals, while falls often cause these in the elderly. The middle third of the diaphysis is most frequently affected, and radial nerve involvement is a critical associated concern. AO/OTA classification is commonly used, describing fracture morphology, location, and severity.
Distal Humerus Fractures: These are less common, accounting for approximately 2% of all adult fractures. They are often complex, intra-articular injuries resulting from high-energy trauma in younger patients (e.g., direct impact on the elbow) or low-energy falls in osteoporotic elderly individuals. The challenge lies in restoring articular congruity and elbow stability while preserving neurovascular structures. The AO/OTA classification provides a comprehensive framework for characterizing these complex injuries.
This guide is designed for orthopedic surgeons, residents, and medical students, offering a high-yield, evidence-based review of humerus fracture management, emphasizing surgical anatomy, operative indications, techniques, and potential complications.

Surgical Anatomy & Biomechanics
A thorough understanding of the humerus's regional anatomy and biomechanics is paramount for effective surgical management.
Proximal Humerus
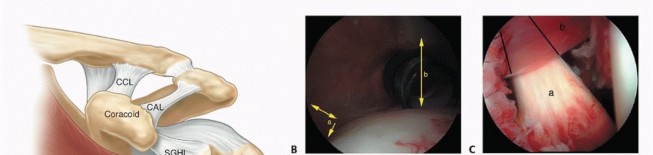
- Bony Anatomy: The proximal humerus comprises the humeral head, anatomical and surgical necks, greater and lesser tuberosities, and the bicipital groove. The head is approximately hemispherical, articulating with the glenoid fossa.
- Rotator Cuff: The supraspinatus, infraspinatus, and teres minor insert onto the greater tuberosity, while the subscapularis inserts onto the lesser tuberosity. These muscles exert significant deforming forces on fracture fragments and are critical for shoulder function.
- Vascularity: The blood supply to the humeral head is primarily derived from the anterior and posterior humeral circumflex arteries. The arcuate artery, a branch of the anterior humeral circumflex artery, penetrates the head near the bicipital groove and is crucial for subchondral bone vascularity. Fractures disrupting these vessels, particularly Neer 3- and 4-part fractures, significantly increase the risk of avascular necrosis (AVN). The calcar region, a dense bony strut posteromedial to the humeral head, provides critical support for locking plate constructs.
- Nerve Structures: The axillary nerve courses circumferentially around the surgical neck, approximately 5-7 cm distal to the acromion, making it vulnerable during surgical approaches and plate application.
Humeral Diaphysis
- Bony Anatomy: The humeral shaft extends from the surgical neck to the supracondylar ridges. Its cross-sectional anatomy changes from cylindrical proximally to triangular distally.
- Muscle Attachments: The pectoralis major, latissimus dorsi, and teres major insert proximally, creating adduction and internal rotation forces. The deltoid inserts at the midshaft, creating abduction forces. Biceps and triceps act distally. Deforming forces vary significantly with fracture location.
- Nerve Structures: The radial nerve is the most critical structure, traversing the posterior aspect of the humerus in the spiral groove, running intimately against the bone. It pierces the lateral intermuscular septum approximately 10-14 cm proximal to the lateral epicondyle, then divides into deep (posterior interosseous nerve) and superficial branches. The nerve's vulnerability in diaphyseal fractures, particularly those of the middle and distal thirds, necessitates careful assessment and protection. The brachial artery and median nerve are located anteromedially but are less commonly injured in closed diaphyseal fractures.
Distal Humerus
- Bony Anatomy: The distal humerus features the trochlea (medial, articulates with ulna) and capitellum (lateral, articulates with radius), flanked by the medial and lateral epicondyles. The olecranon and coronoid fossae accommodate the olecranon and coronoid processes of the ulna during flexion and extension.
- Ligaments: The medial (ulnar) collateral ligament complex and lateral (radial) collateral ligament complex provide critical elbow stability.
- Nerve Structures: The ulnar nerve passes posteriorly in the cubital tunnel, behind the medial epicondyle, making it highly susceptible to injury during trauma and surgical exposure. The median nerve and brachial artery are located anteriorly, within the cubital fossa.
Indications & Contraindications
Management of humerus fractures spans a spectrum from non-operative care to complex surgical reconstruction. The decision-making process is guided by patient factors (age, comorbidities, functional demands), fracture characteristics (location, displacement, comminution, open vs. closed), and surgeon expertise.
Proximal Humerus Fractures
-
Non-Operative Indications:
- Minimally displaced fractures (Neer 1-part).
- Stable 2-part surgical neck fractures with acceptable angulation (<45 degrees) and translation (<1 cm).
- Valgus-impacted fractures.
- Patients with significant medical comorbidities precluding surgery, or low functional demands.
-
Operative Indications:
-
ORIF (Locking Plate Osteosynthesis/IMN):
- Displaced 2-part surgical neck fractures with unacceptable angulation or translation.
- Displaced 2-part greater tuberosity fractures (>5mm displacement in active patients).
- Displaced 2-part lesser tuberosity fractures (rarely operative, may indicate posterior dislocation).
- Most 3-part and 4-part fractures in younger, active patients.
- Fracture-dislocations.
- Open fractures.
-
Arthroplasty (Hemiarthroplasty/Reverse Shoulder Arthroplasty):
- Displaced 4-part fractures, particularly in elderly patients with osteoporotic bone where tuberosity fixation is unreliable.
- Humeral head split fractures with severe comminution.
- Head-splitting fractures with articular surface damage.
- Fractures with high risk of AVN.
- Failed ORIF with nonunion or AVN.
- Reverse shoulder arthroplasty (RTSA) is increasingly favored in elderly patients, especially those with pre-existing rotator cuff dysfunction or irreparable tuberosity comminution.
-
ORIF (Locking Plate Osteosynthesis/IMN):
Humeral Diaphyseal Fractures
-
Non-Operative Indications:
- Most closed, stable diaphyseal fractures with acceptable alignment (angulation <20 degrees in AP, <30 degrees in lateral; shortening <3 cm; no rotational malalignment). These are typically managed with a functional brace (e.g., Sarmiento brace).
- Patients with significant comorbidities or unwilling to undergo surgery.
-
Operative Indications:
-
ORIF (Plate Osteosynthesis/IMN):
- Open fractures.
- Polytrauma patients requiring early mobilization or weight-bearing.
- Vascular injury requiring repair.
- Associated brachial plexus or radial nerve injury (controversial for nerve; typically treated in conjunction if nerve deficit is acute/complete/open).
- Floating elbow injury.
- Pathological fractures.
- Segmental fractures.
- Fractures with unacceptable alignment or inability to maintain reduction with non-operative management.
- Delayed union or nonunion.
- Concomitant ipsilateral forearm fractures requiring stabilization (floating elbow).
- Obesity, making bracing difficult.
-
ORIF (Plate Osteosynthesis/IMN):
Distal Humerus Fractures
-
Non-Operative Indications:
- Rarely indicated for displaced fractures, generally only for truly non-displaced, stable, extra-articular fractures in low-demand patients or those medically unfit for surgery.
-
Operative Indications:
-
ORIF (Dual Plating):
- Most displaced distal humerus fractures, both extra-articular and intra-articular (AO/OTA Type C).
- Fracture-dislocations.
- Open fractures.
- Failure of non-operative management.
-
Total Elbow Arthroplasty (TEA):
- Severely comminuted intra-articular fractures, particularly in elderly, low-demand patients with osteoporotic bone where stable ORIF is unlikely.
- Patients with pre-existing inflammatory arthritis.
- Failed ORIF or nonunion with severe articular destruction.
-
ORIF (Dual Plating):
Contraindications for Operative Management
- Absolute: Active infection (unless urgent debridement/fixation for open fracture), severe uncorrectable medical comorbidities precluding anesthesia.
- Relative: Severe soft tissue compromise (consider external fixation then delayed ORIF), poor bone quality precluding stable fixation, non-compliance with post-operative regimen.
Table: Operative vs. Non-Operative Indications for Humerus Fractures
| Fracture Location | Fracture Type / Characteristics | Non-Operative Management | Operative Management |
|---|---|---|---|
| Proximal Humerus | Minimally displaced (Neer 1-part) | Sling, early ROM | - |
| Stable 2-part surgical neck (<45° angulation, <1cm translation) | Sling, early ROM | - | |
| Displaced 2-part (surgical neck, tuberosity) | - | ORIF (locking plate/IMN) | |
| 3-part, 4-part (Neer) | - (except in very low-demand, high-risk patients) | ORIF (locking plate/IMN), Hemiarthroplasty, RTSA | |
| Fracture-dislocation, open fracture | - | ORIF, Arthroplasty | |
| Humeral Diaphysis | Closed, stable, acceptable alignment (<20° angulation, <3cm shortening) | Functional brace (Sarmiento) | - |
| Open fracture | - | ORIF (plate/IMN) with debridement | |
| Unacceptable alignment, inability to reduce | - | ORIF (plate/IMN) | |
| Polytrauma, vascular injury, floating elbow, pathological | - | ORIF (plate/IMN) | |
| Radial nerve palsy (controversial, typically conservative unless open fracture/vascular injury) | Observation, EMG/NCS follow-up | Nerve exploration if complete deficit, open fracture | |
| Distal Humerus | Non-displaced, stable extra-articular (rare) | Sling/splint, early ROM if stable | - |
| Displaced extra-articular, intra-articular (Type C) | - | ORIF (dual plating) | |
| Severely comminuted intra-articular (elderly, osteoporotic) | - | Total Elbow Arthroplasty (TEA) | |
| Fracture-dislocation, open fracture | - | ORIF, TEA |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for successful outcomes and to anticipate potential challenges.
Pre-Operative Planning
-
Imaging:
- Standard Radiographs: AP, lateral, and scapular Y views for proximal humerus; AP and lateral views for diaphyseal and distal humerus (ensure full length of humerus including shoulder/elbow joints for shaft). Transthoracic lateral or trauma lateral views may be necessary for uncooperative patients.
- CT Scan: Indispensable for complex fractures, especially 3- and 4-part proximal humerus fractures, intra-articular distal humerus fractures, and highly comminuted diaphyseal fractures. 3D reconstructions are invaluable for understanding fracture morphology, articular involvement, and fragment rotation. Angio-CT may be required for suspected vascular injury.
- MRI: Rarely indicated acutely but can be useful for assessing rotator cuff integrity in proximal humerus fractures, or chronic soft tissue lesions.
-
Patient Evaluation:
- Thorough medical history and physical examination to assess comorbidities, neurovascular status, and soft tissue envelope.
- Evaluate for associated injuries (polytrauma protocol if indicated).
- Anesthesia consultation and medical optimization.
-
Surgical Strategy:
- Fracture Classification: Utilize standard systems (Neer, AO/OTA) to guide implant selection and approach.
- Implant Selection: Determine type of plate (locking vs. non-locking), intramedullary nail (antegrade vs. retrograde, reamed vs. unreamed), or arthroplasty components.
- Templating: Utilize templating films to estimate plate length, screw size, and appropriate implant dimensions. This aids in anticipating the number of screws needed proximal and distal to the fracture.
- Surgical Approach: Plan the incision and approach based on fracture location and morphology, considering internervous planes and critical neurovascular structures.
- Reduction Strategy: Plan for provisional reduction techniques (e.g., K-wires, joy sticks, external manipulation).
Patient Positioning
Appropriate patient positioning is crucial for adequate exposure, fluoroscopic access, and nerve protection.
Proximal Humerus
- Beach Chair Position: Common for deltopectoral approach. Head supported, torso slightly elevated (30-60 degrees), arm draped free. Allows for manipulation of the arm. Care must be taken to prevent brachial plexus stretch or spinal injury.
- Supine Position on Radiolucent Table: Arm on an arm board or over a radiolucent hand table, allowing full fluoroscopic visualization. Pillow under ipsilateral scapula. Less strain on the spine.
- Fluoroscopy: Essential for all operative proximal humerus fractures. C-arm positioned to obtain true AP, lateral (outlet/Y view), and axillary views.
Humeral Diaphysis
-
Positioning depends on the chosen surgical approach:
- Anterolateral Approach: Supine on a radiolucent table, arm on an arm board. Allows for radial nerve protection.
- Posterior Approach (for middle/distal shaft): Lateral decubitus or prone. For lateral decubitus, the arm can be draped free or supported on an arm rest. Prone position offers excellent visualization but requires careful airway management.
- Fluoroscopy: Required for confirming reduction and implant placement.
Distal Humerus
- Lateral Decubitus or Prone Position: Arm draped over a support or on an articulated arm holder. This allows for unrestricted movement of the elbow joint during surgery.
- Tourniquet: Often used for distal humerus ORIF to minimize bleeding and improve visualization.
- Ulnar Nerve Protection: Meticulous padding and positioning to prevent iatrogenic ulnar nerve injury.
- Fluoroscopy: Crucial for confirming articular reduction and implant placement, especially with dual plating.
Detailed Surgical Approach / Technique
Proximal Humerus ORIF (Locking Plate Osteosynthesis)
Approach: Deltopectoral Approach
1.
Incision:
Start at the coracoid process, extend distally 8-10 cm along the deltopectoral groove.
2.
Dissection:
Identify and preserve the cephalic vein (retract laterally with the deltoid or medially with the pectoralis major). Develop the interval between the deltoid (lateral) and pectoralis major (medial).
3.
Deep Dissection:
Incise the clavipectoral fascia. Retract the conjoined tendon and musculocutaneous nerve medially.
4.
Axillary Nerve Identification:
Proximally, identify the anterior branch of the axillary nerve running inferomedially from the quadrangular space, 5-7 cm distal to the acromion. Protect it meticulously.
5.
Subdeltoid Exposure:
Incise the subdeltoid bursa. Expose the fracture site.
Reduction & Fixation
1.
Reduction:
* Gently debride hematoma and soft tissue impeding reduction.
* Use K-wires as "joy sticks" into the humeral head and shaft for manipulation.
* Suture passage (heavy non-absorbable) through the rotator cuff tendons (supraspinatus, infraspinatus, subscapularis) and tuberosity fragments can aid in reduction and stability.
* Restore anatomical neck-shaft angle (approximately 130-140 degrees of valgus).
* Provisional fixation with K-wires across the fracture lines and into the glenoid or transosseously.
2.
Plate Application (e.g., PHILOS plate):
* Position the plate laterally on the proximal humerus, approximately 5-8 mm distal to the superior aspect of the greater tuberosity (to avoid acromial impingement).
* Ensure the plate sits flush to the bone.
* Place proximal locking screws into the humeral head. Aim for inferomedial support (calcar screws) to resist varus collapse.
* Place distal cortical or locking screws into the humeral shaft, ensuring at least 3-4 bicortical screws for adequate fixation.
*
Image Integration:
The provided second image

is generic "Image". If it were to depict a surgical scene, a locking plate in situ or during application for proximal humerus fracture would be a relevant context.
3.
Tuberosity Repair:
If tuberosity fragments are avulsed, pass sutures through the fragments and secure them to the plate or adjacent tendons for enhanced stability.
4.
Final Checks:
Confirm reduction and hardware position with fluoroscopy. Assess range of motion for impingement. Close in layers.
Humeral Diaphyseal ORIF (Plate Osteosynthesis)
Approach: Anterolateral Approach (for proximal/midshaft fractures)
1.
Incision:
Longitudinal incision on the anterolateral aspect of the arm.
2.
Dissection:
Develop the interval between the deltoid (laterally) and the biceps/brachialis (medially). Proximally, the deltopectoral groove is identified.
3.
Radial Nerve:
Crucial to identify and protect the radial nerve. It typically exits the spiral groove in the distal third of the humerus, but its course is variable. Proximally, it lies posterior to the humerus. Distally, it pierces the lateral intermuscular septum to lie anteriorly. Elevate the brachialis muscle from the anterior humeral shaft.
4.
Exposure:
Expose the fracture site.
Reduction & Fixation (Plate Osteosynthesis)
1.
Reduction:
* Indirect reduction techniques (traction, external manipulation) are preferred for comminuted fractures to preserve fracture biology.
* Direct reduction with reduction clamps or K-wires may be used for simple patterns.
* Ensure anatomical length and rotation are restored.
2.
Plate Application (e.g., LCP):
* Bridge plating is preferred for comminuted fractures to maintain indirect reduction and preserve periosteal blood supply.
* Plate length should allow for at least 6 cortices of fixation (3 bicortical screws) proximal and distal to the fracture zone.
* For simple fracture patterns, compression plating can be applied.
* Ensure the plate avoids impingement on the deltoid or triceps.
* Place screws carefully, considering the radial nerve. Post-operative X-rays to confirm no radial nerve impingement.
Approach: Posterior Approach (for mid/distal shaft fractures)
1.
Incision:
Longitudinal incision posteriorly from the acromion to the olecranon.
2.
Dissection:
Split the triceps muscle or use a paratricipital approach (between long and lateral heads of triceps).
3.
Radial Nerve Identification:
Isolate the radial nerve as it exits the spiral groove. It is typically found between the lateral and medial heads of the triceps. Mobilize and protect it with a vessel loop.
4.
Exposure:
Expose the humeral shaft posteriorly.
Fixation (Intramedullary Nailing - IMN)
1.
Antegrade Nailing (for proximal/midshaft):
*
Entry Point:
Typically through the greater tuberosity, either directly through its apex or through a more lateral approach (between the supraspinatus and infraspinatus tendons) to avoid rotator cuff damage.
*
Reaming:
Ream the canal incrementally to match nail diameter.
*
Nail Insertion:
Advance the nail across the fracture, ensuring it is sufficiently distal.
*
Locking Screws:
Place proximal and distal interlocking screws for rotational and angular stability.
2.
Retrograde Nailing (for mid/distal shaft):
*
Entry Point:
Through the olecranon fossa, usually just proximal to the olecranon. Requires elbow flexion.
*
Nail Insertion:
Advance nail proximally.
*
Locking Screws:
Place proximal and distal interlocking screws.
Distal Humerus ORIF (Dual Plating)
Approach: Posterior Approach with Olecranon Osteotomy (Standard for complex intra-articular fractures)
1.
Incision:
Posterior midline incision over the elbow.
2.
Ulnar Nerve:
Identify and release the ulnar nerve proximally, throughout the cubital tunnel, and distally into the flexor carpi ulnaris. Transpose it anteriorly to protect it.
3.
Olecranon Osteotomy:
Perform a Chevron or transverse osteotomy of the olecranon. Preserve the triceps tendon insertion. Reflect the olecranon proximally with the triceps. This provides excellent exposure of the distal humeral articular surface.
4.
Exposure:
Elevate medial and lateral soft tissues to expose the fracture.
Reduction & Fixation
1.
Articular Reduction:
* The primary goal is anatomical restoration of the articular surface. Use small K-wires or reduction clamps.
* Reconstruct the trochlea and capitellum. Provisional fixation with small K-wires.
* Confirm articular congruity with fluoroscopy and direct visualization.
2.
Column Reconstruction:
* Reduce the medial and lateral columns to the reconstructed articular segment and the humeral shaft.
* Ensure correct rotation, length, and valgus/varus alignment.
3.
Dual Plating:
* Apply two plates (orthogonal or parallel constructs). The orthogonal (90/90) technique is common, with one plate on the medial column and another on the posterior or posterolateral aspect of the lateral column. Parallel plating (both medial and lateral plates on the posterior surface) is also effective and can provide good stability.
* Utilize long plates to ensure adequate fixation in the humeral shaft.
* Place bicortical screws through both plates where possible, ensuring they do not interfere with each other or the articular surface. Locking plates enhance stability in osteoporotic bone.
4.
Olecranon Osteotomy Fixation:
* Fix the olecranon osteotomy with a tension band wire construct or an olecranon plate, ensuring stable fixation to allow early elbow motion.
Post-Operative Considerations:
*
Wound Closure:
Meticulous layered closure.
*
Neurovascular Assessment:
Critical post-operatively.
*
Early Motion:
As soon as stable fixation is achieved, early range of motion is paramount, especially for distal humerus fractures, to prevent stiffness.
Complications & Management
Humerus fractures and their treatment are associated with a range of potential complications, some common, others devastating. Proactive recognition and appropriate management are crucial.
Proximal Humerus Specific Complications
-
Avascular Necrosis (AVN) of the Humeral Head:
- Incidence: Varies from 0% in 2-part to 10-30% in 3-part, and up to 30-80% in 4-part fractures, especially those with significant head displacement or disruption of the medial calcar and articular blood supply.
- Management: Non-operative (activity modification, analgesia) for early asymptomatic stages. For symptomatic AVN or collapse, hemiarthroplasty or reverse shoulder arthroplasty are common salvage options.
-
Nonunion/Malunion:
- Incidence: Varies, but higher in complex patterns, osteoporotic bone, or inadequate fixation.
- Management: Malunion may be managed conservatively if asymptomatic or with osteotomy if symptomatic. Nonunion typically requires revision ORIF with bone grafting, or arthroplasty.
-
Rotator Cuff Dysfunction/Impingement:
- Incidence: Common, due to tuberosity malunion, hardware prominence, or primary cuff tear.
- Management: Physical therapy, hardware removal if prominent, or rotator cuff repair.
-
Stiffness/Adhesive Capsulitis:
- Incidence: Significant problem post-ORIF.
- Management: Early aggressive rehabilitation. Manipulation under anesthesia or arthroscopic capsular release for refractory cases.
-
Axillary Nerve Injury:
- Incidence: Can occur with initial trauma or iatrogenically during surgery (1-10%).
- Management: Observation for spontaneous recovery (up to 6-12 months), EMG/NCS. Surgical exploration for complete deficits with no recovery or open injury.
Humeral Diaphyseal Specific Complications
-
Radial Nerve Palsy:
- Incidence: Most common complication, 8-15% of closed diaphyseal fractures. Up to 20% in open fractures. Most are neurapraxias and resolve spontaneously (90% within 3-6 months).
- Management: Observation for closed fractures. Splinting for wrist/finger drop. EMG/NCS after 3-4 months if no recovery. Surgical exploration indicated for acute complete deficit with an open fracture, lack of recovery by 3-6 months, or secondary injury during surgery.
-
Nonunion:
- Incidence: 5-10% with operative fixation, higher with non-operative management of certain patterns (e.g., transverse, comminuted, open). Smoking and NSAID use increase risk.
- Management: Revision surgery with plate exchange, IMN, or bone grafting (autograft or allograft), potentially with biological adjuncts.
-
Malunion:
- Incidence: More common with non-operative management.
- Management: Acceptable if minimal. Symptomatic malunion (cosmetic, impingement, pain) may require corrective osteotomy.
-
Infection:
- Incidence: ~1-5% in closed fractures, much higher in open fractures.
- Management: Surgical debridement, appropriate antibiotic therapy, hardware retention if stable, or staged removal and external fixation.
Distal Humerus Specific Complications
-
Ulnar Nerve Neuropathy:
- Incidence: Up to 10-25% due to initial trauma, prolonged traction, surgical manipulation, or post-operative scarring/swelling.
- Management: Observation for neurapraxia. Anterior transposition during surgery reduces risk. Surgical neurolysis for persistent symptomatic cases.
-
Stiffness/Loss of Motion:
- Incidence: Extremely common, especially loss of extension. Up to 50% may have some degree of stiffness.
- Management: Early and aggressive rehabilitation. Heterotopic ossification prophylaxis (radiation/NSAIDs). Manipulation under anesthesia, arthrolysis, or total elbow arthroplasty for severe, debilitating stiffness.
-
Heterotopic Ossification (HO):
- Incidence: Up to 20-30% in severe trauma or head injury patients.
- Management: Prophylaxis with NSAIDs or low-dose radiation in high-risk patients. Excision for symptomatic HO after maturation.
-
Post-Traumatic Arthritis:
- Incidence: Long-term complication of intra-articular fractures despite anatomical reduction.
- Management: Non-operative for mild cases. Total elbow arthroplasty for debilitating arthritis.
-
Nonunion/Malunion:
- Incidence: Less common with modern dual plating techniques but can occur with inadequate fixation or poor bone quality.
- Management: Revision ORIF with plate exchange, bone grafting, or TEA.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Fracture Location | Incidence (%) | Salvage Strategy / Management |
|---|---|---|---|
| Avascular Necrosis (AVN) | Proximal Humerus | 10-80% (esp. 3-4 part fractures) | Hemiarthroplasty, Reverse Shoulder Arthroplasty |
| Radial Nerve Palsy | Humeral Diaphysis | 8-15% (closed); up to 20% (open) | Observation (90% resolve), EMG/NCS, Nerve exploration/repair, Tendon transfer |
| Nonunion | All | Proximal: 5-10%; Diaphyseal: 5-10%; Distal: <5% | Revision ORIF (plate/nail exchange, bone graft), Arthroplasty (for proximal/distal) |
| Malunion | All | Varies with fracture type/treatment | Observation, Corrective osteotomy (for symptomatic cases) |
| Stiffness / Loss of Motion | All (esp. Distal) | Proximal: 10-20%; Diaphyseal: 5-10%; Distal: 30-50% | Early rehabilitation, Manipulation under anesthesia, Arthrolysis, Arthroplasty |
| Ulnar Nerve Neuropathy | Distal Humerus | 10-25% (surgical/post-op) | Observation, Neurolysis, Anterior transposition |
| Axillary Nerve Injury | Proximal Humerus | 1-10% (surgical) | Observation, Nerve exploration/repair, Tendon transfer |
| Infection | All | 1-5% (closed); >10% (open) | Debridement, Antibiotics, Hardware retention/removal, Staged reconstruction |
| Hardware Impingement/Failure | All | 5-15% | Hardware removal, Revision fixation |
| Heterotopic Ossification (HO) | Distal Humerus | 20-30% (severe trauma/TBI) | Prophylaxis (NSAIDs/XRT), Excision (after maturation) |
| Post-Traumatic Arthritis | Proximal, Distal | Long-term complication | Non-operative, Arthroplasty |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical procedure itself for achieving optimal functional outcomes. Protocols are tailored based on fracture stability, fixation achieved, and individual patient factors.
General Principles
- Pain Management: Multimodal approach including NSAIDs (if no contraindication to healing), opioids, nerve blocks.
- Wound Care: Standard wound care, suture/staple removal at 2-3 weeks.
- Early Mobilization: The goal is to initiate motion as soon as stability allows, preventing stiffness while protecting healing bone.
Proximal Humerus Fracture Rehabilitation
-
Phase 1: Immobilization & Protection (0-4/6 weeks)
- Goal: Protect fracture healing, control pain/edema.
- Intervention: Arm in sling (shoulder immobilizer) for 4-6 weeks, potentially removed for hygiene and specific exercises. Elbow, wrist, hand ROM exercises. Pendulum exercises (Codman's) for gravity-assisted passive motion, initiated usually within 1-2 weeks. Scapular stabilization exercises. No active shoulder range of motion or lifting.
-
Phase 2: Early Motion (4-12 weeks)
- Goal: Restore passive and active-assisted ROM.
- Intervention: Progress from passive to active-assisted exercises (e.g., pulley exercises, cane exercises). Begin gentle isometric exercises for rotator cuff and deltoid, without resistance. No lifting objects heavier than 1-2 lbs. Wean from sling as comfort and stability allow.
-
Phase 3: Strengthening & Advanced Motion (12+ weeks)
- Goal: Restore active ROM, improve strength, endurance.
- Intervention: Gradual progression to active resistance exercises for all shoulder musculature, initially with light weights/bands. Progress to functional activities. Return to sport/heavy lifting typically cleared by 4-6 months, depending on fracture consolidation confirmed by radiographs.
Humeral Diaphyseal Fracture Rehabilitation
-
Non-Operative (Functional Bracing):
- Intervention: Immediate application of a functional fracture brace (Sarmiento). Early active and passive ROM for shoulder and elbow. Brace is worn full-time until radiographic union, then gradually weaned.
-
Operative (ORIF/IMN):
-
Phase 1: Early Protection & Motion (0-6 weeks)
- Goal: Protect fixation, maintain joint mobility above/below fracture.
- Intervention: Sling for comfort. Early active and passive ROM for shoulder and elbow as pain allows (e.g., pendulum exercises, elbow flexion/extension, forearm rotation). No weight-bearing through the arm or resisted lifting.
-
Phase 2: Gradual Strengthening (6-12 weeks)
- Goal: Increase strength, restore full ROM.
- Intervention: Begin light isometric exercises, gradually progress to resistance exercises (bands, light weights). Full active ROM encouraged. Careful with exercises that apply torsional stress across the healing fracture.
-
Phase 3: Advanced Strengthening & Return to Activity (12+ weeks)
- Goal: Maximize strength, power, and endurance.
- Intervention: Progress with resistance training. Gradual return to work and sport activities. Full union must be confirmed radiographically before unrestricted activity or heavy lifting.
-
Phase 1: Early Protection & Motion (0-6 weeks)
Distal Humerus Fracture Rehabilitation
-
Phase 1: Early Motion (0-3 weeks)
- Goal: Prevent stiffness, protect anatomical reduction.
- Intervention: If fixation is stable, immediate continuous passive motion (CPM) or active-assisted ROM exercises for the elbow (flexion/extension, pronation/supination). Often initiated within 2-5 days post-op. A dynamic splint or hinged elbow brace may be used for protection and controlled motion. Ulnar nerve gliding exercises.
-
Phase 2: Progressive Motion & Light Strengthening (3-8 weeks)
- Goal: Increase ROM, begin light strengthening.
- Intervention: Progress with active and passive ROM. Begin gentle isometric exercises for forearm and triceps. Light resistance exercises for biceps and triceps. Avoid activities that could apply varus or valgus stress to the elbow.
-
Phase 3: Strengthening & Functional Recovery (8+ weeks)
- Goal: Restore full strength, power, and function.
- Intervention: Gradual increase in resistance exercises. Incorporate functional activities and sport-specific training. Full return to activity typically at 4-6 months, contingent on radiographic union and strength recovery. Close monitoring for heterotopic ossification or nerve irritation.
Summary of Key Literature / Guidelines
Evidence-based practice is paramount in orthopedic trauma. Several key studies and guidelines inform the management of humerus fractures.
Proximal Humerus Fractures
- Neer Classification (1970): Remains the cornerstone, guiding treatment based on displacement of the four segments. While inter-observer reliability can be an issue, it provides a common language.
- Current Trends: While ORIF with locking plates (e.g., PHILOS) is standard for many displaced fractures in younger patients, evidence for its superiority over non-operative management in minimally displaced fractures or those with high AVN risk is mixed.
- Arthroplasty in Elderly: Recent literature, particularly the DELPHI study, supports reverse total shoulder arthroplasty (RTSA) over hemiarthroplasty for complex proximal humerus fractures in elderly patients, citing better functional outcomes and lower revision rates due to tuberosity complications with hemiarthroplasty. The PROFHER trial (2015) , a landmark randomized controlled trial, demonstrated no significant difference in functional outcomes between surgical fixation and non-operative treatment for displaced proximal humerus fractures in adults. This study significantly shifted the paradigm, emphasizing judicious patient selection for operative intervention. However, its generalizability to all fracture types and patient populations is debated.
Humeral Diaphyseal Fractures
- Non-operative Management: Functional bracing (Sarmiento brace) has a high success rate (80-90% union) for closed, stable fractures with acceptable alignment, as described by Sarmiento et al.
- Operative Indications: Clear indications for surgery include open fractures, vascular injury, floating elbow, pathological fractures, segmental fractures, and failure of non-operative treatment.
- IMN vs. Plating: Literature comparing intramedullary nailing (IMN) and plate osteosynthesis for diaphyseal fractures shows similar union rates, but IMN is associated with a higher risk of shoulder pain, while plating carries a higher risk of iatrogenic radial nerve injury (though rare). IMN is generally preferred for comminuted or segmental fractures, while plating is often chosen for fractures near the metaphysis or those with an associated radial nerve deficit (allowing nerve exploration). A meta-analysis by Rathore et al. (2014) indicated no significant difference in nonunion, malunion, or infection rates between plating and nailing for diaphyseal humerus fractures, but plating had a higher incidence of radial nerve palsy and nailing had more shoulder pain.
Distal Humerus Fractures
- Dual Plating: Orthogonal or parallel dual plating constructs are the gold standard for displaced intra-articular distal humerus fractures, providing stable fixation necessary for early range of motion. Studies by O'Driscoll et al. and others have elucidated the biomechanical principles of these constructs.
- Total Elbow Arthroplasty (TEA): Increasingly recognized as a viable option for severely comminuted intra-articular fractures in low-demand elderly patients, offering reliable pain relief and early function when ORIF is technically challenging or likely to fail. Long-term outcomes for TEA in trauma patients are generally good, though implant longevity and activity restrictions remain considerations.
General Guidelines
- AO/OTA Classification: The comprehensive classification system is essential for consistent description, treatment planning, and research across all regions of the humerus.
- Radial Nerve Management: Current guidelines for radial nerve palsy in closed humeral shaft fractures recommend an initial period of observation (3-6 months) unless the injury is open, involves a vascular deficit, or there is no sign of recovery on serial EMG/NCS.
- Open Fractures: Require urgent surgical debridement and stabilization, with prophylactic antibiotics, tetanus immunization, and early soft tissue coverage as per Gustilo-Anderson classification principles.
The continuous evolution of surgical techniques, implant designs, and rehabilitation protocols necessitates ongoing engagement with the orthopedic literature to provide the most effective and evidence-based care for patients with humerus fractures.
You Might Also Like