Anterior Glenohumeral Dislocation: Comprehensive Guide to Epidemiology, Anatomy, Biomechanics & Management
Key Takeaway
Anterior glenohumeral dislocation is when the humeral head displaces anteriorly from the glenoid, representing 95-97% of all shoulder dislocations. Often caused by an abducted, externally rotated arm trauma, it involves injury to static stabilizers like the Inferior Glenohumeral Ligament complex (e.g., Bankart lesion) and potential axillary nerve damage.
Introduction & Epidemiology
Anterior glenohumeral dislocation represents the most prevalent form of shoulder instability, accounting for approximately 95-97% of all shoulder dislocations. This traumatic event occurs when the humeral head is forcefully displaced anteriorly and inferiorly relative to the glenoid fossa. The typical mechanism involves an indirect force applied to an arm in an abducted, externally rotated, and extended position, commonly seen in contact sports, falls onto an outstretched hand, or motor vehicle accidents. In the elderly population, lower energy trauma may precipitate dislocation due to underlying degenerative changes, often associated with concomitant rotator cuff tears or proximal humeral fractures.
The incidence of primary anterior shoulder dislocation is estimated at 17 to 20 per 100,000 person-years. Demographically, young, active males (18-30 years old) involved in contact or overhead sports exhibit the highest rates of initial and recurrent dislocations. A second peak in incidence is observed in individuals over 60, where the mechanism of injury tends to be less violent, and the prevalence of associated soft tissue injuries, particularly rotator cuff tears, is significantly higher.
The immediate priorities in the emergency department (ER) for an anterior shoulder dislocation are prompt diagnosis, thorough neurovascular assessment, safe reduction of the joint, confirmation of reduction, and identification of any associated injuries. Early and appropriate management is crucial to mitigate acute complications and inform subsequent definitive treatment strategies aimed at preventing recurrence and restoring optimal shoulder function.
Surgical Anatomy & Biomechanics
A comprehensive understanding of glenohumeral anatomy and biomechanics is fundamental for the effective management of anterior shoulder dislocations.
Bony Anatomy
- Glenoid Fossa: A shallow, pear-shaped articular surface on the lateral aspect of the scapula. Its depth and orientation (glenoid version and inclination) contribute minimally to static stability. Significant glenoid bone loss from recurrent dislocations can critically compromise stability.
- Humeral Head: Approximately one-third to one-half of a sphere, much larger than the glenoid, emphasizing the shoulder's inherent mobility over stability. Its retroversion (typically 30-40 degrees relative to the epicondylar axis) is crucial for glenohumeral articulation.
- Coracoid Process & Acromion: Part of the scapular spine, these bony landmarks provide attachment sites for numerous ligaments and muscles, indirectly influencing glenohumeral stability.
Capsuloligamentous Structures
The joint capsule is a thin, fibrous envelope, reinforced anteriorly by three distinct thickenings known as the glenohumeral ligaments (GHLs), along with the coracohumeral ligament.
*
Superior Glenohumeral Ligament (SGHL):
Limits inferior translation of the humeral head when the arm is adducted.
*
Middle Glenohumeral Ligament (MGHL):
Contributes to anterior stability in mid-ranges of abduction and external rotation.
*
Inferior Glenohumeral Ligament (IGHL) Complex:
This is the primary static stabilizer against anterior dislocation when the arm is abducted and externally rotated. It consists of an anterior band (AIGHL), a posterior band (PIGHL), and an intervening axillary pouch. Pathological lesions to the AIGHL, particularly an avulsion from the anterior-inferior glenoid (Bankart lesion), are pathognomonic for anterior instability.
*
Coracohumeral Ligament:
Connects the coracoid to the greater and lesser tuberosities, contributing to superior stability and preventing inferior subluxation.
Labrum
The glenoid labrum is a fibrocartilaginous ring that circumferentially deepens the glenoid fossa by approximately 50%, enhancing the congruity between the humeral head and glenoid. It serves as an attachment point for the joint capsule and the glenohumeral ligaments. A traumatic avulsion of the anterior-inferior labrum, often accompanied by a periosteal stripping (Bankart lesion), is the most common pathology in anterior dislocations.
Musculature
- Rotator Cuff (SITS muscles): Supraspinatus, Infraspinatus, Teres Minor, Subscapularis. These muscles dynamically stabilize the glenohumeral joint by compressing the humeral head into the glenoid, particularly during movement. The subscapularis plays a critical role in anterior stability by resisting external rotation.
- Deltoid: A large, powerful muscle responsible for shoulder abduction and flexion/extension, it contributes to dynamic stability but can also exacerbate dislocation forces if spastic.
Neurovascular Structures
- Axillary Nerve: The most commonly injured nerve in anterior shoulder dislocations. It originates from the posterior cord of the brachial plexus (C5-C6), exits the axilla through the quadrangular space, and innervates the deltoid and teres minor muscles, providing sensation over the lateral deltoid (regimental badge area). Pre- and post-reduction assessment of axillary nerve function is paramount.
- Brachial Plexus: Damage to other components of the brachial plexus is less common but can occur with severe trauma.
- Axillary Artery and Vein: Located anterior and medial to the humeral head. Injury is rare but devastating, typically occurring in elderly patients with atherosclerotic vessels or high-energy trauma. Assessment of distal pulses is essential.
Biomechanics of Stability
Glenohumeral stability is a complex interplay of static and dynamic factors:
*
Static Stabilizers:
*
Bony Congruity:
The relatively flat glenoid and large humeral head contribute minimally, making the joint inherently mobile but unstable.
*
Glenoid Labrum:
Deepens the fossa.
*
Joint Capsule and Ligaments (GHLs):
Act as primary restraints, especially the IGHL in abduction and external rotation.
*
Negative Intra-articular Pressure:
Contributes to suction effect, maintaining coaptation.
*
Dynamic Stabilizers:
*
Rotator Cuff Muscles:
Compress the humeral head into the glenoid, providing a dynamic "concavity compression" effect.
*
Long Head of Biceps Tendon:
Contributes to superior and anterior stability.
*
Scapular Stabilizers:
Proper scapular rhythm and muscle balance are crucial for optimal glenohumeral mechanics.
Pathomechanically, anterior dislocation occurs when forces overcome the anterior static and dynamic restraints, typically leading to avulsion of the capsulolabral complex (Bankart lesion) or plastic deformation of the anterior capsule. The posterolateral humeral head often impacts the anterior glenoid rim, creating a compression fracture known as a Hill-Sachs lesion.
Indications & Contraindications
The management of anterior shoulder dislocation involves immediate reduction in the ER setting, followed by comprehensive evaluation to determine the need for further intervention, including potential surgical stabilization.
ER Management (Acute Reduction)
Indications for Attempted Closed Reduction:
* All acute anterior glenohumeral dislocations without absolute contraindications. Prompt reduction minimizes pain, swelling, and potential neurovascular compromise.
Contraindications / Red Flags for Blind Closed Reduction:
*
Absolute Contraindications:
*
Significant neurovascular compromise (e.g., absent pulses, acute limb ischemia):
This necessitates immediate vascular surgery consultation and may require open reduction and vascular repair.
*
Relative Contraindications / Indications for Urgent Orthopedic Consultation/OR:
*
Suspected Irreducible Dislocation:
Clinical suspicion of soft tissue interposition (e.g., biceps tendon, labrum, capsule, subscapularis) or bony impingement. Attempts at closed reduction in these cases are futile and may cause further damage.
*
Associated Unstable Fractures:
* Displaced surgical neck fracture of the humerus.
* Large, significantly displaced greater tuberosity fracture.
* Large bony Bankart lesion involving >20-25% of the glenoid articular surface, especially if irreducible or significantly unstable after reduction.
*
Open Dislocation:
Requires urgent surgical debridement and reduction.
Operative Intervention (Acute or Elective)
Indications for Acute Operative Intervention (Rare, Emergent):
*
Irreducible Dislocation:
Failed closed reduction attempts requiring open reduction.
*
Significant Neurovascular Injury:
Requiring emergent exploration and repair (e.g., axillary artery laceration).
*
Complex Fracture-Dislocation:
Displaced humeral surgical neck or greater tuberosity fractures that preclude stable closed reduction or warrant ORIF.
*
Extensive Bony Bankart Lesion:
If unstable after reduction and significantly compromising joint stability acutely.
Indications for Elective Operative Intervention (for Recurrent Instability or High Risk):
*
Recurrent Anterior Instability:
The primary indication for surgical stabilization, particularly if symptomatic and affecting quality of life or athletic performance.
*
First-Time Dislocation with High Risk of Recurrence:
* Young age (<25-30 years old).
* Participation in contact or overhead sports.
* Presence of significant lesions on MRI/CT (e.g., Bankart lesion, significant Hill-Sachs lesion, glenoid bone loss).
*
Significant Glenoid Bone Loss (>20-25%):
Pre-disposition to recurrent instability, often managed with bony augmentation (e.g., Latarjet procedure).
*
Engaging Hill-Sachs Lesion:
A large Hill-Sachs lesion that engages the anterior glenoid rim during abduction and external rotation, leading to recurrent dislocation.
*
Failed Non-Operative Management:
Persistent instability despite appropriate rehabilitation and activity modification.
*
Associated Rotator Cuff Tear:
If symptomatic and warranting repair.
Contraindications for Elective Operative Intervention:
*
Patient Unfit for Surgery:
Significant medical comorbidities or general anesthesia risks.
*
Non-Compliance:
Unwillingness or inability to adhere to post-operative rehabilitation protocols.
*
Minimal Symptoms / Low Demand:
Older, less active individuals with minimal symptoms may be managed non-operatively.
*
Chronic Dislocation (>3-6 weeks):
Without significant symptoms or functional impairment, surgical intervention may be more complex with higher risk, and non-operative management may be preferred in certain cases.
Operative vs. Non-Operative Indications
| Feature | Non-Operative Management (ER/Initial) | Operative Management (Acute/Elective) |
|---|---|---|
| Primary Goal | Pain relief, restoration of anatomy, early mobility | Definitive stabilization, prevention of recurrence, anatomical restoration, addressing associated pathology. |
| Acute Dislocation | All reducible dislocations without significant associated injuries. | Acute: Irreducible dislocation; significant neurovascular injury requiring exploration; large, displaced concomitant fracture (e.g., >5mm displaced greater tuberosity, unstable proximal humerus fx); large bony Bankart fragment involving >20-25% glenoid. |
| Recurrent Instability | Seldom indicated after initial event for high-risk patients; brace treatment; activity modification for low-demand patients or those unfit for surgery. | Elective: Symptomatic recurrent anterior instability; significant glenoid bone loss (>20-25%); engaging Hill-Sachs lesion; failed non-operative management; young, active individuals (especially overhead/contact athletes) with high recurrence risk after first dislocation. |
| Patient Factors | Elderly, low-demand patients; individuals with contraindications to surgery. | Young, active individuals (especially overhead/contact athletes); patients with connective tissue disorders predisposing to instability (consider specific techniques); patients for whom recurrence is unacceptable. |
| Associated Pathology | Small, non-displaced rotator cuff tears (initial conservative trial); small, non-engaging Hill-Sachs; small, stable non-displaced bony Bankart. | Significant rotator cuff tear requiring repair; large engaging Hill-Sachs; Bankart lesion with significant capsulolabral avulsion; large bony Bankart (>20-25% glenoid loss). |
Pre-Operative Planning & Patient Positioning
ER Pre-Reduction Planning
-
History and Physical Examination:
- Mechanism of Injury: Helps anticipate potential associated injuries.
- Prior Dislocations: Inquire about frequency, ease of dislocation, previous treatments.
-
Neurovascular Assessment:
This is critical.
- Neurological: Assess axillary nerve function (sensation over lateral deltoid, deltoid contraction), musculocutaneous nerve (biceps), and the entire brachial plexus (median, ulnar, radial nerve motor/sensory function). Document meticulously before reduction.
- Vascular: Palpate radial and ulnar pulses; assess capillary refill and skin color/temperature.
-
Imaging:
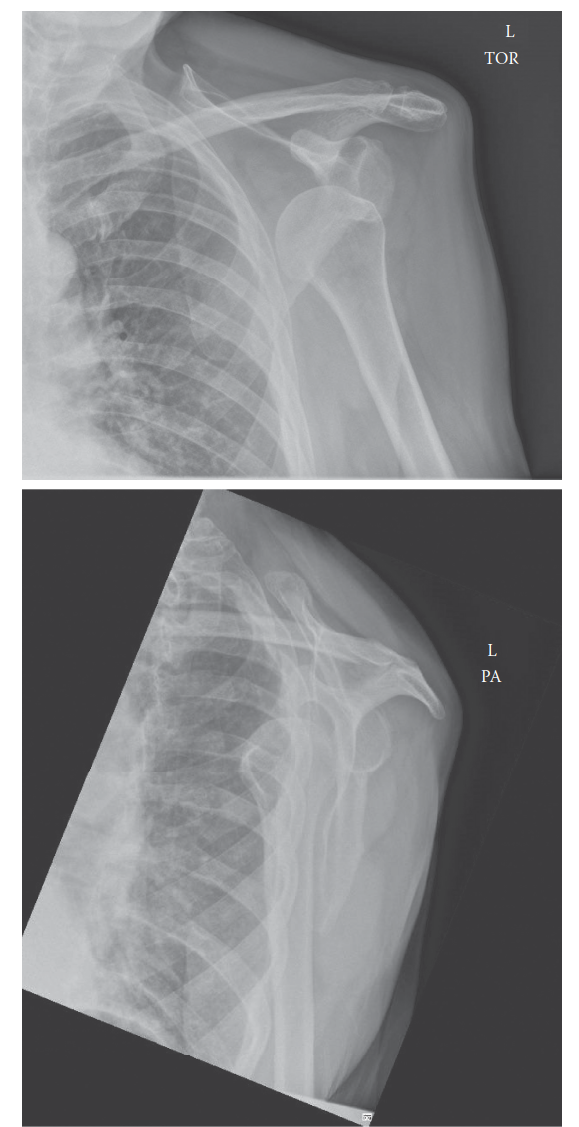
- X-rays (Pre-reduction): An essential diagnostic step. Obtain minimum of two views, typically an AP (Anteroposterior) view and a Y-scapular (or Lateral Transscapular) view. An Axillary Lateral view is ideal but often difficult to obtain pre-reduction due to pain. These views confirm dislocation, identify the direction (anterior, posterior, inferior), and screen for associated fractures (e.g., greater tuberosity, surgical neck, Hill-Sachs, bony Bankart).
-
Pain Management and Sedation:
- Analgesia: Intravenous opioids (e.g., fentanyl, morphine) are typically administered.
- Conscious Sedation: Often necessary to achieve adequate muscle relaxation for successful reduction and minimize patient discomfort. Common agents include midazolam (anxiolysis) combined with fentanyl, or dissociative agents like ketamine or etomidate. Careful monitoring of vital signs and airway is mandatory.
- Regional Anesthesia: An interscalene or supraclavicular brachial plexus block can provide excellent analgesia and muscle relaxation, reducing the need for systemic sedation and its associated risks.
- Informed Consent: Obtain consent for the reduction procedure, explaining the risks (e.g., nerve/vascular injury, iatrogenic fracture, failure of reduction, recurrence).
- Positioning: Position the patient appropriately for the chosen reduction maneuver (e.g., supine, prone, seated).
Surgical Planning (for Elective Stabilization)
-
Advanced Imaging:
- CT Scan: Crucial for quantifying glenoid bone loss and evaluating the size and engagement of a Hill-Sachs lesion. 3D reconstructions are highly valuable.
- MRI: Essential for assessing labral pathology (Bankart lesion, ALPSA lesion, Perthes lesion), rotator cuff integrity, capsular laxity, and cartilaginous damage.
- Pre-operative Medical Workup: Standard assessment of patient health, comorbidities, and fitness for general or regional anesthesia.
- Equipment and Instrumentation: Ensure availability of arthroscopy tower, video system, shaver, radiofrequency ablation, suture passers, suture anchors (bioabsorbable or non-absorbable), suture material. For open procedures, appropriate retractors, drills, and fixation implants. For bony procedures (Latarjet), guide wires, screws, and potential allograft/autograft.
-
Patient Positioning:
- Beach Chair Position: Most common for arthroscopic shoulder surgery. Allows for easy access to the anterior, posterior, and superior aspects of the shoulder. The torso is semi-reclined (30-70 degrees), arm is free-draped or in an arm holder.
- Lateral Decubitus Position: Patient lies on the contralateral side, affected arm placed in a traction device. Offers good visualization, particularly for posterior and inferior glenoid work, but requires careful positioning and traction management.
- Antibiotic Prophylaxis: Administer pre-operatively (e.g., Cefazolin) according to institutional protocols.
Detailed Surgical Approach / Technique
I. Acute Reduction Techniques (ER Management)
The goal of acute reduction is to restore anatomical alignment of the humeral head within the glenoid fossa with minimal force, preventing iatrogenic injury. Adequate analgesia and muscle relaxation are paramount.
An illustrative image potentially depicting a shoulder dislocation on X-ray, or a reduction maneuver.
General Principles of Reduction:
*
Muscle Relaxation:
Achieved via conscious sedation or regional block.
*
Gentle and Controlled Forces:
Avoid aggressive or forceful maneuvers that can cause iatrogenic fractures or neurovascular damage.
*
Traction and Counter-traction:
Often utilized to overcome muscle spasm.
*
Leverage:
Applying forces to the humeral head to guide it back into the glenoid.
Commonly Employed Reduction Techniques:
-
Kocher's Method:
- Mechanism: Externally rotates, adducts, and internally rotates the humeral head.
-
Steps:
- Patient supine or seated. Examiner stands on the affected side.
- Traction: Grasp the patient's elbow, apply gentle, sustained longitudinal traction in slight abduction.
- External Rotation: Slowly and gently externally rotate the arm to approximately 90 degrees (until resistance is met or reduction occurs). Caution: Do not force external rotation if pain or resistance is excessive.
- Adduction: Adduct the elbow across the patient's chest.
- Internal Rotation: Internally rotate the arm by bringing the hand towards the opposite shoulder.
- Success Rate: High, but historically associated with higher complication rates if performed forcefully.
-
Stimson's Technique (Gravity Method):
- Mechanism: Utilizes gravity and muscle fatigue for reduction.
-
Steps:
- Patient prone on an examination table, the affected arm hanging over the side.
- Attach a 5-10 lb weight to the patient's wrist.
- Allow the weight to apply sustained traction for 10-20 minutes, which gradually fatigues the muscles.
- Gentle internal and external rotation of the arm may aid reduction.
- Success Rate: High, patient-friendly, often requires minimal sedation.
-
Scapular Manipulation:
- Mechanism: Repositions the glenoid relative to the humeral head.
-
Steps:
- Patient prone (similar to Stimson's) or seated.
- One assistant applies longitudinal traction to the arm (with or without weights).
- The examiner uses one hand to stabilize the superior scapula (acromion) and the other to grasp the inferior angle of the scapula.
- Rotate the inferior angle medially and the superior aspect laterally.
- Success Rate: High, especially when combined with gentle traction.
-
External Rotation Method (Hennepin or Cunningham Method variants):
- Mechanism: Relies on slow, sustained external rotation to fatigue muscle spasm.
-
Steps:
- Patient supine or seated, arm adducted to the chest, elbow flexed to 90 degrees.
- Gently and slowly externally rotate the forearm/hand while maintaining adduction.
- Maintain gentle pressure, allowing muscles to relax. Reduction typically occurs within 5-10 minutes.
- Success Rate: High, often requires minimal or no sedation, making it suitable for field use.
-
Traction-Countertraction Method:
- Mechanism: Direct longitudinal force to overcome muscle spasm and lever the humeral head into place.
-
Steps:
- Patient supine. An assistant applies counter-traction by pulling a sheet wrapped around the patient's axilla.
- The examiner grasps the affected arm and applies sustained longitudinal traction.
- Gentle adduction or external rotation may be applied during traction to aid reduction.
- Success Rate: Reliable, but requires two operators and good muscle relaxation.
Post-Reduction Assessment:
1.
Confirm Reduction:
Clinically, a palpable "clunk," restoration of normal shoulder contour, and ability to move the arm passively and actively (within pain limits).
2.
Neurovascular Reassessment:
Repeat the full neurovascular examination immediately after reduction to detect any iatrogenic injury.
3.
Post-Reduction X-rays:
Obtain AP and Axillary Lateral (or Y-scapular) views to confirm concentric reduction and identify any new or previously unappreciated fractures (e.g., iatrogenic greater tuberosity fracture).
4.
Immobilization:
Immobilize the arm in a sling and swathe for comfort and to allow initial soft tissue healing. Duration is debatable, typically 1-3 weeks in internal rotation. For young, active patients, controversy exists regarding immobilization in external rotation, though practical challenges and compliance issues are significant.
II. Surgical Stabilization (Example: Arthroscopic Anterior Labral Repair / Bankart Repair)
For patients with recurrent anterior instability, significant labral pathology, or high-risk features, surgical stabilization is often indicated. Arthroscopic Bankart repair is the most common technique for primary labral pathology.
Indications: Recurrent anterior instability due to a Bankart lesion with minimal glenoid bone loss (<20-25%).
Patient Positioning:
*
Beach Chair Position:
The patient is placed in a semi-recumbent position (30-70 degrees elevation) with the affected shoulder draped freely. The head is stabilized and protected. The arm can be held by an assistant or in an articulating arm holder.
Anesthesia: General anesthesia, often supplemented with an interscalene block for post-operative analgesia.
Portals:
1.
Posterior Portal (Standard):
2-3 cm inferior and 1 cm medial to the posterior angle of the acromion. Used for initial diagnostic arthroscopy and visualizing the anterior glenoid.
2.
Anterosuperior Portal:
Created under direct visualization, just lateral to the anterior aspect of the acromion. Used for suture anchor placement and superior labral repair.
3.
Anteroinferior Portal (Working Portal):
Created under direct visualization, typically 1 cm superior to the subscapularis tendon, in the rotator interval. This is the primary working portal for anterior labral repair, suture passing, and knot tying. Additional anteroinferior portals may be used as needed.
Detailed Surgical Steps:
-
Diagnostic Arthroscopy:
- Systematic evaluation of all intra-articular structures: rotator cuff, biceps tendon, labrum (especially anterior-inferior), glenoid articular cartilage, humeral head articular cartilage (assess for Hill-Sachs lesion), and capsular integrity.
- Confirm the presence and extent of the Bankart lesion (avulsion of the anterior-inferior labrum and IGHL complex).
- Assess for glenoid bone loss and Hill-Sachs engagement.
- Perform a dynamic stability assessment under arthroscopic visualization.
-
Preparation of the Glenoid Neck:
- Using a shaver or radiofrequency device through the working portal, debride the anterior-inferior glenoid neck to expose bleeding bone. This promotes healing of the reattached labrum. Ensure the glenoid articular cartilage is not damaged.
-
Mobilization of the Capsulolabral Complex:
- Using a periosteal elevator or blunt dissector, free the anterior-inferior capsulolabral complex from the glenoid neck. Ensure sufficient mobilization to allow anatomical reduction of the labrum to the glenoid rim without excessive tension. Release any medialized scar tissue.
-
Suture Anchor Placement:
- Typically 2-4 suture anchors (bioabsorbable or non-absorbable) are placed along the anterior-inferior glenoid rim, starting from the 5 o'clock position (right shoulder) and moving superiorly towards the 3 o'clock position.
- A guidewire is advanced through the anteroinferior portal and drilled into the glenoid rim, ensuring appropriate trajectory to capture bone securely.
- The suture anchor is then inserted.
-
Capsulolabral Repair and Fixation:
- Using specialized suture passers through the working portals, the sutures from the anchors are passed through the avulsed capsulolabral complex.
- The goal is to capture sufficient tissue to anatomically reduce the labrum to the glenoid rim and imbricate the anterior capsule, recreating the anterior bumper and tensioning the inferior glenohumeral ligament complex.
- Sutures are then tied using arthroscopic knot-tying techniques, securing the labrum and capsule to the glenoid.
-
Assessment of Stability:
- Perform a thorough arthroscopic assessment of glenohumeral stability by manually translating and rotating the humeral head throughout the range of motion. Confirm appropriate capsular tension and reduction of anterior translation.
-
Closure: Remove instruments, irrigate the joint, and close portal sites with sutures or steri-strips. Apply sterile dressings.
Internervous Planes (relevant for Open Bankart / Latarjet):
* If an open approach is chosen (e.g., for Latarjet procedure or complex cases), the
deltopectoral interval
is utilized.
* This interval lies between the deltoid (innervated by the axillary nerve) and the pectoralis major (innervated by medial and lateral pectoral nerves).
* The cephalic vein typically runs in this interval and should be preserved if possible.
* Careful dissection is required to protect the axillary nerve as it courses inferiorly and posteriorly, approximately 5-7 cm distal to the acromion.
Complications & Management
Complications following anterior shoulder dislocation can range from minor neurosensory deficits to recurrent instability and debilitating fractures. Prompt recognition and appropriate management are essential.
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Recurrence | 20-90% (highest in young, active males post-first dislocation) |
Prevention:
Appropriate post-reduction immobilization and rehabilitation; surgical stabilization (Arthroscopic Bankart repair, Latarjet procedure, Remplissage) for high-risk patients or after first recurrence.
Salvage: Re-evaluation of underlying pathology (bone loss, engagement), revision stabilization (e.g., Latarjet for glenoid bone loss, Remplissage for engaging Hill-Sachs, capsular shift for generalized laxity). |
| Axillary Nerve Injury | 5-50% (predominantly neuropraxia) |
Diagnosis:
Clinical assessment (deltoid motor function, lateral arm sensation).
Management: Observation is primary. Most neuropraxias resolve spontaneously within 3-6 months. Electromyography (EMG) and Nerve Conduction Studies (NCS) at 3 months if no recovery. Surgical exploration rarely indicated, only for complete loss with no signs of recovery after 6 months or in cases of nerve transection suspected acutely. |
| Rotator Cuff Tear | 30-80% (>40 years old) |
Diagnosis:
Clinical suspicion in older patients, confirmed by MRI.
Management: Acute surgical repair for significant tears, especially if symptomatic and in active patients. Small, non-displaced tears may be managed non-operatively initially with physical therapy. |
| Hill-Sachs Lesion | 60-80% |
Diagnosis:
AP X-ray (internal rotation view), CT scan for quantification.
Management: Non-operative if small and non-engaging. For engaging lesions, surgical options include: - Remplissage: Arthroscopic capsulodesis of the infraspinatus tendon into the defect. - McLaughlin Procedure: Transfer of subscapularis tendon into the defect (for posterior instability, less common in anterior). - Bone grafting: For very large lesions. |
| Bony Bankart Lesion | Up to 20% |
Diagnosis:
X-rays (especially West Point axillary view), CT scan for quantification.
Management: Non-operative if small (<20% glenoid surface), stable, and non-displaced. Arthroscopic repair with suture anchors for larger, but stable, fragments. Latarjet procedure or allograft/autograft reconstruction for fragments involving >20-25% of the glenoid articular surface or unstable fragments. |
| Vascular Injury (Axillary Artery) | <1% (rare, but severe) |
Diagnosis:
Absent distal pulses, expanding hematoma, signs of ischemia.
Management: IMMEDIATE vascular surgery consultation. Angiography. Emergent open repair or bypass. Life-limb threatening emergency. |
| Irreducible Dislocation | Rare |
Diagnosis:
Failed multiple gentle closed reduction attempts.
Management: Emergent open reduction, typically via an anterior deltopectoral approach, to remove interposed soft tissue (labrum, biceps, subscapularis, capsule) or bony fragments. |
| Post-Reduction Stiffness / Adhesive Capsulitis | Variable |
Prevention:
Early, controlled range of motion exercises (especially in older patients).
Management: Physical therapy, anti-inflammatory medications. Manipulation under anesthesia (MUA) or arthroscopic capsular release for refractory cases. |
| Iatrogenic Fracture | Rare (e.g., greater tuberosity, humeral neck) |
Prevention:
Gentle reduction techniques, adequate sedation.
Management: Depends on fracture type and displacement. ORIF for displaced fractures (e.g., >5mm greater tuberosity or significant humeral neck displacement). |
| Infection (Surgical) | <1% |
Prevention:
Strict aseptic technique, prophylactic antibiotics.
Management: Debridement, irrigation, appropriate antibiotics (empiric initially, then culture-directed). May require hardware removal in persistent cases. |
Post-Operative Rehabilitation Protocols
Rehabilitation after shoulder dislocation, whether treated non-operatively or surgically, is critical for restoring range of motion (ROM), strength, stability, and functional return. Protocols are typically phased, progressive, and individualized.
Post-Reduction (Non-Operative Management)
-
Phase I: Protection & Early Motion (Weeks 0-3)
- Immobilization: Sling and swathe for comfort, typically 1-3 weeks. The optimal duration and position (internal vs. external rotation) of immobilization are debated; prolonged immobilization in internal rotation can lead to stiffness, especially in older patients. For younger, active patients, some protocols suggest external rotation bracing, though compliance is a challenge.
- Goals: Pain control, protect healing soft tissues, prevent stiffness in unaffected joints.
- Activities: Pendulum exercises, elbow/wrist/hand ROM exercises. Avoid active abduction, external rotation, and extension beyond neutral. Scapular setting exercises within pain tolerance.
-
Phase II: Intermediate Motion & Light Strengthening (Weeks 3-6)
- Goals: Restore pain-free passive and active-assisted ROM, begin gentle strengthening.
- Activities: Progressive passive and active-assisted ROM (flexion, abduction, internal/external rotation within safe limits). Initiate gentle isometric strengthening of rotator cuff and deltoid. Begin light resistance band exercises for internal rotation and adduction.
- Precautions: Avoid combined abduction and external rotation, especially at 90 degrees.
-
Phase III: Progressive Strengthening & Proprioception (Weeks 6-12)
- Goals: Restore full ROM, improve strength, endurance, and proprioception.
- Activities: Continue progressive strengthening (rotator cuff, deltoid, periscapular muscles) with increasing resistance. Introduce proprioceptive exercises (e.g., balance board, rhythmic stabilization). Begin plyometric exercises for athletes.
-
Phase IV: Return to Activity (Weeks 12+ / Months 3-6)
- Goals: Gradual return to full activities, including sport-specific training.
- Activities: Advanced strengthening, power training, and sport-specific drills. Return to contact sports or overhead activities is typically 3-6 months, depending on individual progress and recurrence risk.
Post-Surgical Stabilization (e.g., Arthroscopic Bankart Repair)
Rehabilitation protocols following surgical stabilization are more structured and emphasize protecting the repair while gradually restoring function.
-
Phase I: Maximum Protection & Early Passive Motion (Weeks 0-6)
- Immobilization: Sling for 4-6 weeks, typically in internal rotation, removing only for hygiene and exercises.
- Goals: Protect the capsulolabral repair, control pain and swelling, prevent stiffness, initiate early protected passive ROM.
-
Activities:
- Passive ROM: Pendulum exercises. Passive flexion to 90-120 degrees. Passive external rotation to 0-30 degrees (surgeon-dependent, conservative initially). Passive abduction to 45-60 degrees.
- Elbow, Wrist, Hand ROM: Actively perform exercises to prevent stiffness.
- Scapular Mobility: Gentle scapular retraction and protraction exercises.
- Precautions: No active shoulder motion. No lifting. Avoid external rotation and extension beyond prescribed limits.
-
Phase II: Moderate Protection & Progressive Motion (Weeks 6-12)
- Goals: Gradually increase passive and active-assisted ROM to full, initiate gentle active strengthening.
-
Activities:
- ROM: Progress passive and active-assisted ROM. Initiate active ROM (flexion, scaption, internal rotation). Continue working towards full external rotation (up to 45-60 degrees initially, then full).
- Strengthening: Gentle isometric exercises (internal/external rotation, abduction, flexion). Progress to light resistance band exercises for internal rotation and adduction. Begin scapular stabilization with light resistance.
- Precautions: Continue to avoid combined abduction and maximal external rotation. No lifting heavy objects.
-
Phase III: Minimum Protection & Advanced Strengthening (Weeks 12-24)
- Goals: Restore full, pain-free ROM. Progress strengthening, power, and endurance. Improve proprioception.
-
Activities:
- Strengthening: Progress with resistance exercises for all major shoulder muscle groups (rotator cuff, deltoid, pectoralis, latissimus dorsi, periscapular). Incorporate free weights, machines, and resistance bands.
- Proprioception: Advanced proprioceptive drills (e.g., plyoball, dynamic stability).
- Functional Training: Begin sport-specific drills if appropriate. Gradually reintroduce overhead activities.
- Precautions: Monitor for pain and compensations. Avoid ballistic movements and maximal external rotation at 90 degrees abduction until late in this phase.
-
Phase IV: Return to Sport / High-Demand Activity (Months 6-9+)
- Goals: Full return to desired activities, including competitive sports.
- Activities: Comprehensive sport-specific training, agility drills, plyometrics. Focus on power, endurance, and dynamic stability required for specific activities.
- Criteria for Return: Full pain-free ROM, strength >90% of the contralateral limb, negative apprehension tests, successful completion of functional and sport-specific testing.
- Timeline: Return to contact sports or overhead activities typically takes 6-9 months or longer after surgical stabilization.
Summary of Key Literature / Guidelines
The management of anterior shoulder dislocation is continuously refined by evolving research, yet several foundational principles and landmark studies guide current practice.
-
Reduction Techniques: While numerous closed reduction techniques exist, current literature suggests that success rates are generally high across most methods when performed with adequate analgesia and muscle relaxation. The choice often depends on provider experience and patient comfort. Techniques emphasizing gentle, slow movements (e.g., external rotation, Stimson) may require less sedation and carry a lower risk of iatrogenic injury compared to forceful maneuvers.
- Sayegh, F. E., et al. (2015). "Reduction maneuvers for anterior shoulder dislocation: a systematic review and meta-analysis." CJEM 17(5): 521-527. This review highlights the high success rates of various techniques and the importance of sedation.
-
Immobilization Post-Reduction: The optimal duration and position of immobilization after a first-time anterior dislocation remain controversial. Early studies advocated for prolonged immobilization in internal rotation to allow capsulolabral healing, but more recent evidence, particularly from meta-analyses, has challenged this.
- Hovelius, L., et al. (1982). "Primary anterior dislocation of the shoulder in young patients: a ten-year study." J Bone Joint Surg Am 64(7): 955-961. A classic study establishing recurrence rates in young patients.
- Handoll, H. H. G., et al. (2004). "Interventions for treating acute traumatic anterior dislocation of the shoulder." Cochrane Database Syst Rev 3: CD004290. This foundational Cochrane review found insufficient evidence to recommend any specific immobilization strategy over another.
- Recent studies on external rotation bracing: While theoretically appealing, external rotation bracing has largely shown no significant clinical benefit in reducing recurrence rates compared to internal rotation immobilization and suffers from poor patient compliance.
-
Surgical vs. Non-Surgical Management: For young, active individuals, particularly those involved in contact or overhead sports, surgical stabilization after a first-time traumatic anterior dislocation significantly reduces the risk of recurrence compared to non-operative management.
- Kirkley, A., et al. (2003). "A randomized clinical trial comparing arthroscopic stabilization to nonoperative treatment for a first episode traumatic anterior shoulder dislocation." Am J Sports Med 31(4): 556-563. This landmark trial demonstrated a significantly lower recurrence rate with arthroscopic stabilization.
- Bottoni, C. R., et al. (2006). "A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations." Am J Sports Med 34(11): 1742-1748. Another randomized trial supporting surgical intervention in young, active patients.
- For older patients (>40-50 years), the risk of rotator cuff tears is higher, and the recurrence rate is lower, often favoring non-operative management unless a specific surgical indication (e.g., significant rotator cuff tear) exists.
-
Management of Bone Loss: The presence of significant glenoid bone loss (typically >20-25%) or an engaging Hill-Sachs lesion significantly increases the risk of recurrence after isolated soft tissue repair (e.g., Bankart repair). Quantification of bone loss via CT imaging is critical for surgical planning.
- Burkhart, S. S., and M. D. De Beer. (2004). "Capsulolabral reconstruction for recurrent anterior shoulder instability. Surgical technique." J Bone Joint Surg Am 86.Suppl 1: 50-64. Describes the concept of the "inverted pear" glenoid and the importance of addressing bone loss.
- Lafosse, L., et al. (2006). "Arthroscopic Latarjet procedure for anterior shoulder instability. Surgical technique." J Bone Joint Surg Am 88.Suppl 1: 190-202. Details the arthroscopic approach to the Latarjet procedure, which is the gold standard for glenoid bone loss.
- Remplissage (arthroscopic infracoracoid capsulotenodesis): An effective technique to address engaging Hill-Sachs lesions, improving stability by filling the defect with capsule and infraspinatus tendon.
-
Complications: Axillary nerve neuropraxia is the most common neurological complication, usually resolving spontaneously. Rotator cuff tears are a significant concern, especially in older patients, warranting careful screening and potential surgical repair. Vascular injuries are rare but devastating.
Overall Guidelines: Major orthopedic societies (e.g., AAOS, ESSKA) emphasize a thorough pre-reduction assessment, gentle and well-sedated reduction, post-reduction imaging to confirm reduction and rule out iatrogenic injury, and an individualized management plan based on patient age, activity level, associated pathology (especially bone loss), and patient preference. The goal is to restore stability and function while minimizing the risk of recurrence and complications.
You Might Also Like


