Comprehensive Guide to Slipped Capital Femoral Epiphysis (SCFE): Epidemiology, Biomechanics, and Management
Key Takeaway
Slipped Capital Femoral Epiphysis (SCFE) is an adolescent hip condition involving femoral head displacement due to physeal weakness and shear forces. Surgical *in situ* fixation is the gold standard for both stable and unstable SCFE. This aims to prevent progression, reduce avascular necrosis risk, and optimize long-term hip function. Prophylactic contralateral pinning is often considered.
Mastering Pediatric SCFE: How to Properly Engage the Epiphysis
Introduction & Epidemiology
Slipped Capital Femoral Epiphysis (SCFE) represents a biomechanical failure of the proximal femoral physis, leading to displacement of the femoral head (epiphysis) relative to the femoral neck (metaphysis). This posteromedial displacement is a critical orthopedic condition in adolescents, often precipitated by a combination of biomechanical stress and underlying physeal weakness. Its classification is paramount for guiding treatment strategies. Stable SCFE allows for weight-bearing, albeit painfully, while unstable SCFE prevents any weight-bearing, carrying a significantly higher risk of avascular necrosis (AVN) and other severe complications. Further categorization includes acute (symptoms < 3 weeks), chronic (symptoms > 3 weeks), and acute-on-chronic slips.
The incidence of SCFE ranges from 0.7 to 10.8 per 100,000 children annually, with a notable increase observed in recent decades, correlating with the rising prevalence of childhood obesity. Males are affected more frequently than females, typically presenting between 10-16 years in boys and 8-14 years in girls. Risk factors extend beyond obesity to include endocrine disorders such as hypothyroidism, growth hormone deficiency, renal osteodystrophy, and panhypopituitarism, which contribute to physeal weakening. Early diagnosis and appropriate surgical intervention are critical to prevent slip progression, mitigate complications, and optimize long-term hip function.
Surgical Anatomy & Biomechanics
A thorough understanding of the proximal femoral physeal anatomy and biomechanics is fundamental to successful SCFE management. The proximal femoral physis is unique, exhibiting an oblique orientation relative to the horizontal plane, sloping inferoposteriorly. This configuration positions the epiphysis to bear substantial shear forces, particularly during weight-bearing and hip motion.
The epiphyseal side of the physis is cartilaginous, with a complex undulating interface that interdigitates with the metaphyseal side. This creates a zone of transition that is highly susceptible to shear stress. In SCFE, the failure occurs through the hypertrophic zone of the physis. The perichondrial ring (of LaCroix and Hansson) provides critical circumferential stability to the physis; however, in SCFE, this ring, along with the adjacent periosteum, may become attenuated or disrupted, contributing to progressive displacement.
The vascular supply to the femoral head is predominantly via the medial femoral circumflex artery (MFCA) and its retinacular branches, which ascend along the femoral neck within the joint capsule to supply the epiphysis. Critically, these vessels are located posteromedially, the very region most prone to displacement and mechanical impingement in SCFE. Aggressive manipulation during reduction, screw placement that violates the capsular reflection, or excessive physeal compression can compromise these retinacular vessels, leading to devastating avascular necrosis.
Biomechanical factors contributing to SCFE include increased body weight, leading to higher shear forces across the physis. The retroversion of the capital femoral epiphysis and the valgus angle of the physis itself also contribute to the unique susceptibility. The epiphysis typically displaces inferoposteriorly, resulting in external rotation and extension of the femoral head relative to the neck. This understanding dictates the optimal trajectory for surgical stabilization, aiming to counteract the predominant displacement vector.
Indications & Contraindications
Surgical intervention is the cornerstone of SCFE management for the vast majority of cases, aiming to prevent further slip, stabilize the physis, and minimize long-term sequelae. Non-operative management is rarely indicated and typically reserved for specific, highly scrutinized circumstances.
Indications for Operative Management:
- All Unstable SCFE: Considered a surgical emergency due to the high risk (up to 50%) of avascular necrosis (AVN) with conservative management or delayed fixation. Urgent in situ fixation is standard.
- All Stable SCFE (symptomatic): The primary goal is to prevent progression of the slip and stabilize the physis. In situ fixation is the gold standard.
- Contralateral Asymptomatic SCFE (Prophylactic Pinning): While controversial, prophylactic pinning of the contralateral, asymptomatic hip is widely practiced, particularly in patients with risk factors such for bilateral involvement (e.g., younger age, severe obesity, endocrine disorders). The rationale is to prevent future slip, avoid a second, potentially unstable, contralateral event, and minimize the morbidity of two separate surgical episodes. The reported incidence of contralateral slip ranges from 20-60%.
- Failed Non-operative Management: In rare instances where conservative management was initially attempted (e.g., highly stable, minimal slip in a patient with significant medical comorbidities precluding surgery), evidence of slip progression necessitates operative intervention.
Contraindications for Operative Management:
- Absolute Contraindications: None, if the patient is symptomatic and SCFE is diagnosed. The risks of non-treatment far outweigh the surgical risks in most scenarios.
-
Relative Contraindications:
- Asymptomatic, non-displaced contralateral SCFE (Controversial): In cases of very minimal, truly asymptomatic contralateral slips, and in patients without significant risk factors for progression, observation with close clinical and radiographic follow-up may be considered. However, this is a nuanced decision and not a universally accepted approach. Many surgeons advocate for prophylactic pinning in these instances.
- Significant Medical Comorbidities: In rare cases, a patient's medical status may preclude surgery. This requires careful multidisciplinary discussion, but alternative fixation methods (e.g., spica cast) are generally ineffective and associated with high complication rates.
The following table summarizes the indications:
| Indication Type | Specific Condition | Rationale for Intervention | Management Strategy |
|---|---|---|---|
| Operative | Unstable SCFE | High risk of Avascular Necrosis (AVN) and rapid slip progression; surgical emergency. | Urgent in situ fixation (with or without gentle reduction). |
| Operative | Stable SCFE (symptomatic) | Prevent further slip progression, stabilize physis, mitigate long-term sequelae (e.g., FAI, osteoarthritis). | In situ fixation. |
| Operative | Contralateral Asymptomatic SCFE | High risk of subsequent slip (20-60%), particularly in younger patients, severe obesity, or endocrine disorders; preemptive stabilization. | Prophylactic in situ fixation of the contralateral hip. |
| Non-Operative | Asymptomatic, non-displaced contralateral SCFE (controversial) | Very rare; considered only in specific low-risk cases with high patient/family compliance for observation. | Close clinical and radiographic monitoring (AP/frog-leg lateral views every 3-6 months until physeal closure). |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to ensure a safe and effective surgical procedure.
Pre-Operative Planning:
-
Radiographic Assessment:
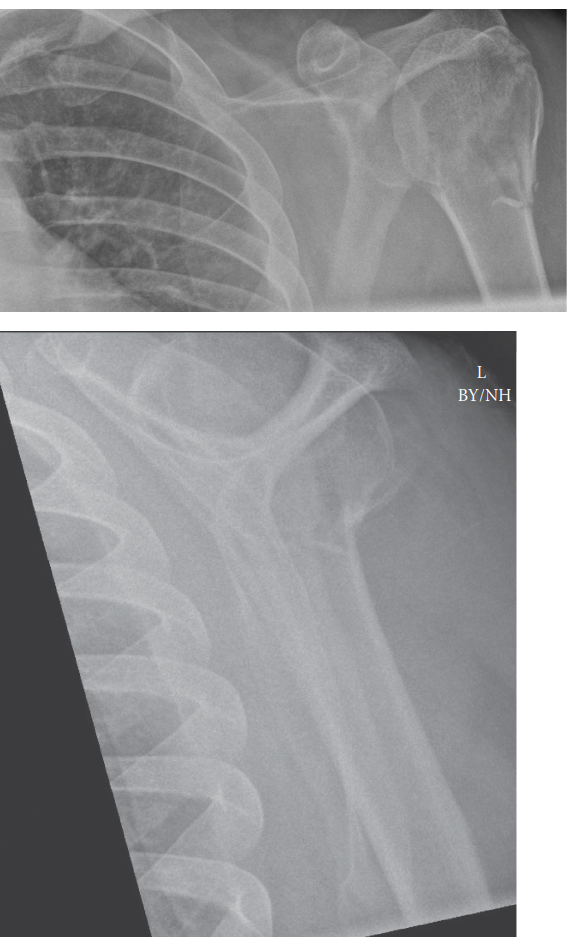
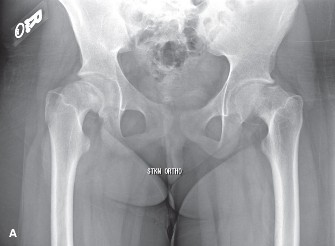
- Plain Radiographs: Anteroposterior (AP) and true lateral views of both hips are indispensable. A frog-leg lateral view is helpful for initial diagnosis but can underestimate slip severity and potentially mask an unstable slip. A true lateral (Lauenstein or cross-table lateral) provides the most accurate assessment of posterior displacement and is critical for surgical planning.
- Classification: The slip angle (Southwick angle) on the lateral view (normal 0-10 degrees) quantifies severity: mild (<30 degrees), moderate (30-50 degrees), and severe (>50 degrees). On the AP view, the Klein's line method can also assess stability and displacement.
- Stability Assessment: Clinical assessment (ability to weight-bear) is paramount for classifying as stable or unstable. Radiographic findings are supportive.
- MRI: Magnetic Resonance Imaging may be utilized in cases of suspected "pre-slip" (bone marrow edema without frank displacement), subtle slips, or to assess physeal edema and integrity. It is not routinely required for clear cases of SCFE.
-
Implant Selection:
- Screws: Cannulated screws, typically 6.5mm or 7.3mm, are standard. The number of screws is debated: a single screw is generally sufficient for stable slips and may reduce AVN risk compared to multiple screws, particularly if screw placement is suboptimal. Two screws may be considered for larger, unstable slips in select cases, but careful trajectory is critical.
- Screw Length: Pre-operative templating based on radiographs can estimate screw length, but intra-operative fluoroscopy will determine the exact required length. Aim for firm epiphyseal engagement without joint penetration.
-
Special Considerations:
- Unstable Slips: Require immediate intervention. Pre-operative reduction attempts are generally discouraged or must be extremely gentle and controlled, as aggressive manipulation significantly increases the risk of AVN.
- Endocrine Workup: For atypical presentations (e.g., very young age, unusual body habitus, bilateral slips without obesity), screening for endocrine disorders (thyroid function tests, growth hormone, renal panel) is indicated.
Patient Positioning:
- Operating Table: The patient is positioned supine on a radiolucent operating table (e.g., a fracture table or a regular operating table with a beanbag). A fracture table offers excellent control for gentle traction and allows for precise positioning for fluoroscopy. If using a regular table, ensure the gluteal region is clear to allow for true lateral imaging.
- C-arm Access: Crucially, the setup must allow for unrestricted movement of the C-arm to obtain high-quality AP, lateral (true lateral and frog-leg), and oblique views of the affected hip. The unaffected leg should be flexed and abducted or placed in a leg holder to facilitate true lateral views of the surgical hip.
- Draping: The entire affected leg is draped freely, allowing for full range of motion of the hip during the procedure to facilitate imaging and, if necessary, gentle manipulation. The iliac crest should also be prepared and draped, as it is a common landmark for the incision.
- Traction: For unstable slips, very gentle traction (5-10 lbs) may be applied through the affected leg prior to incision. The goal is to unload the hip joint and potentially achieve a subtle, spontaneous reduction without forceful manipulation. Over-traction or aggressive forced reduction is contraindicated due to the high risk of retinacular vessel compromise and AVN.
Detailed Surgical Approach / Technique
The primary goal of SCFE fixation is to stabilize the physis and prevent further slip, ensuring proper engagement of the epiphysis without causing iatrogenic injury. In situ fixation with a single cannulated screw is the gold standard for stable slips and the preferred method for unstable slips after gentle or no reduction.
1. Reduction (for Unstable Slips Only):
- Principle: For unstable SCFE, immediate stabilization is critical. While some surgeons advocate for gentle closed reduction, others proceed directly to in situ fixation without formal reduction due to the high AVN risk. If reduction is attempted, it must be extremely gentle and controlled .
- Technique (if attempted): Under fluoroscopic guidance, apply gentle traction to the affected limb. With the hip in slight flexion, perform a slow, sustained internal rotation and abduction maneuver. The goal is to reverse the posteromedial displacement. Absolutely avoid forceful manipulation or repetitive attempts , which are associated with higher rates of AVN. Often, only a partial reduction is achieved or intended. The primary goal remains stabilization.
2. Incision and Approach:
- Incision: A small (2-3 cm) longitudinal or transverse skin incision is made over the lateral aspect of the proximal femur, just inferior to the vastus ridge. The incision should be centered approximately at the level of the tip of the greater trochanter or slightly distal to it.
- Dissection: Blunt dissection is performed through the subcutaneous tissue. The iliotibial band is either split longitudinally or incised transversely. The vastus lateralis muscle is then split or retracted anteriorly to expose the lateral femoral cortex. Care should be taken to avoid stripping the periosteum extensively, which can compromise the metaphyseal blood supply.
- Entry Point: The ideal entry point on the lateral femoral cortex is typically just distal to the vastus ridge, in the metaphyseal region. This location allows for optimal screw trajectory, avoiding fracture of the greater trochanter and minimizing the risk of growth disturbance to the greater trochanteric apophysis.
3. Guide Wire Placement: The Crucial Step for Epiphyseal Engagement
This is the most critical phase, directly addressing "how to properly engage the epiphysis." The guide wire dictates the final screw position and determines the success of fixation and avoidance of complications.
-
Initial Placement:
Insert a 2.0 mm (or similar) cannulated guide wire through the previously identified entry point on the lateral femoral cortex.
- Trajectory - AP View: Advance the guide wire under continuous fluoroscopic guidance. On the AP view, aim for the center of the femoral head (epiphysis). Avoid placing the wire too anteriorly or posteriorly. The optimal trajectory is slightly superior to the center to achieve adequate bone purchase in the weight-bearing dome.
-
Trajectory - Lateral View:
On the true lateral view, this is where the precision of engagement becomes paramount.
- The epiphysis is displaced posteriorly and inferiorly . To counteract this and provide robust fixation, the guide wire should aim for the anterior-superior quadrant of the epiphysis .
- Start the wire trajectory slightly anterior and superior within the femoral neck metaphysis. As the wire crosses the physis, it should penetrate the anterior-superior portion of the epiphysis. This anterior entry into the epiphysis helps prevent further posterior displacement.
- Maintain a trajectory that avoids the posterior-inferior segment of the femoral neck, where the retinacular vessels are most vulnerable.
- Crossing the Physis: The guide wire must traverse the entire width of the physis. You should feel a distinct change in resistance as the wire passes from the softer metaphyseal bone, through the physeal cartilage, and into the denser epiphyseal bone.
-
Epiphyseal Engagement:
- The guide wire must be advanced firmly into the epiphysis. Aim for the tip of the wire to be approximately 2/3 to 3/4 of the way across the epiphysis .
-
Crucially, the wire tip
must not breach the articular cartilage
of the femoral head or enter the hip joint. This is verified by obtaining multiple fluoroscopic views:
- True Lateral View: Confirm the wire tip is well within the epiphysis, not projecting beyond its margin.
- AP View: Confirm central placement and no breach.
- Frog-leg Lateral (if used): Provides an additional perspective.
- Oblique Views: Can be helpful to confirm no joint penetration.
-
"Feel" the Engagement:
A properly positioned guide wire will provide firm tactile feedback as it purchases into the dense epiphyseal bone. If the wire feels "soft" or "wobbly," it may be too superficial or in compromised bone, necessitating repositioning.

- Re-evaluation: If the guide wire position is suboptimal (e.g., too posterior, too anterior, too shallow, or approaching the joint), it must be removed and reinserted. Never attempt to "wiggle" or redirect a partially inserted guide wire, as this can damage the physis or epiphysis.
4. Screw Placement:
- Length Measurement: Once the guide wire is optimally positioned, determine the appropriate screw length using a calibrated depth gauge over the guide wire. The measurement should ensure the screw threads will adequately engage the epiphysis without over-penetrating.
- Drilling: A cannulated drill bit, sized to the chosen screw, is advanced over the guide wire, drilling through the lateral cortex and into the metaphysis. For self-tapping screws, drilling might be limited to the cortex.
-
Screw Insertion:
The cannulated screw is then inserted over the guide wire.
- Avoid Compression (for stable slips): For in situ fixation of stable slips, the screw should be inserted without creating significant compression across the physis. The goal is to pin and stabilize, not to reduce the slip. Over-compression can lead to premature physeal closure, potentially causing further deformity or growth arrest. Use a partially threaded screw where the threads cross the physis and engage the epiphysis, while the smooth shaft spans the physis.
- Gentle Compression (for unstable slips after reduction): If a gentle reduction was performed for an unstable slip, very gentle compression may be applied by fully seating the screw, but this must be done cautiously to minimize AVN risk.
-
Epiphyseal Purchase:
The threads of the screw must securely purchase into the epiphyseal bone. Ensure at least
3-4 full threads
are well within the epiphysis to provide stable fixation. The screw head should be flush with the lateral femoral cortex.

-
Final Fluoroscopic Confirmation:
Obtain final AP and true lateral fluoroscopic images to confirm:
- Central placement of the screw within the epiphysis.
- Adequate epiphyseal engagement (threads entirely within the epiphysis).
- No penetration of the articular cartilage or joint space.
- Appropriate screw length, with the tip well within the epiphysis and not projecting beyond its contours.
5. Wound Closure:
- Remove the guide wire.
- Irrigate the wound.
- Layered closure of the vastus lateralis, iliotibial band, subcutaneous tissue, and skin.
Complications & Management
Despite meticulous technique, SCFE fixation carries a risk of significant complications. Awareness and prompt management are crucial for optimal outcomes.
| Complication | Incidence (%) | Etiology / Risk Factors | Salvage Strategies & Management Principles |
|---|---|---|---|
| Avascular Necrosis (AVN) | 0-10% (stable); 10-50%+ (unstable) | Aggressive reduction, unstable slip, multiple screws, capsular injury, joint penetration, vascular compromise. | Prevention: Gentle/no reduction for unstable slips, single screw, careful capsular management. Management: Core decompression, osteotomies (e.g., Ganz periacetabular or subtrochanteric derotational), vascularized fibular graft, hip fusion, total hip arthroplasty (THA) in adulthood. |
| Chondrolysis | 5-15% | Articular screw penetration, inflammation, reactive synovitis, retained cartilage fragments, infection. | Prevention: Precise screw placement. Management: Analgesics, NSAIDs, physical therapy, intra-articular steroid injections (controversial), arthroscopic debridement, ultimately hip arthrodesis or THA if severe. |
| Further Slip / Nonunion | <5% | Inadequate fixation (short screw, poor epiphyseal purchase), premature weight-bearing, persistent physeal instability. | Revision surgery with repeat in situ fixation (longer screw, better trajectory), or osteotomy (e.g., flexion osteotomy of the femoral neck) for refractory cases. |
| Screw Penetration (Articular) | 1-5% | Improper guide wire/screw placement, dynamic penetration (screw backs out or head shifts). | Immediate screw removal/repositioning. Post-operative observation for chondrolysis/pain. Arthroscopy may be needed for retained fragments or chondral injury. |
| Femoroacetabular Impingement (FAI) | High (especially with moderate-severe slips) | Residual metaphyseal "bump" or deformity at the head-neck junction after the slip, altered femoral head-neck offset. | Prevention: Minimize slip, ideally by early fixation. Management: Hip arthroscopy or open surgical dislocation with osteochondroplasty (cam resection) to restore head-neck offset. |
| Contralateral SCFE | 20-60% | Bilateral hormonal/mechanical predisposition; higher risk in younger, obese, or endocrinopathic patients. | Prophylactic pinning of the contralateral hip (controversial but widely practiced). Close monitoring if not pinned. |
| Infection | <1% | Standard surgical risks. | Incision and drainage (I&D), parenteral antibiotics, hardware removal once physis is closed or infection is controlled. |
| Hardware-Related Issues | Variable (screw prominence, migration) | Improper length, inadequate bone purchase. | Symptomatic hardware removal (typically after physeal closure), repositioning if causing pain or impingement. |
Management Principles for Complications:
- Avascular Necrosis: The most devastating complication. Prevention is key. Once established, AVN can lead to femoral head collapse and severe osteoarthritis. Early recognition is crucial. Management often involves complex reconstructive procedures tailored to the patient's age and degree of collapse, ranging from osteotomies (e.g., valgus osteotomy, Ganz osteotomy to re-orient the acetabulum) to hip fusion or, in adulthood, total hip arthroplasty.
- Chondrolysis: Joint space narrowing due to cartilage degeneration. It can be painful and lead to significant functional limitations. Non-surgical management includes NSAIDs and physical therapy. In severe cases, surgical options like arthroscopic debridement or, ultimately, hip fusion or THA may be required.
- FAI: A common long-term sequela due to the residual metaphyseal prominence (cam deformity) that develops on the anterior-superior aspect of the femoral neck following the posteromedial slip. This can lead to labral tears, chondral damage, and early osteoarthritis. Surgical treatment typically involves arthroscopic or open osteochondroplasty to re-establish a normal head-neck junction and improve range of motion.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation aims to protect the operative site, facilitate healing, and restore hip function while preventing secondary complications. Protocols vary depending on the stability of the slip and the extent of intervention.
1. Stable SCFE, in situ Fixation:
-
Weight-Bearing:
- Partial Weight-Bearing (PWB): Typically initiated immediately or within the first week, using crutches or a walker. PWB continues for 4-6 weeks, allowing for initial soft tissue healing and physeal stabilization.
- Progressive Weight-Bearing to Full Weight-Bearing (FWB): Progress from PWB to FWB over the next 2-4 weeks, guided by pain tolerance and radiographic evidence of healing.
-
Range of Motion (ROM):
- Early, Gentle ROM: Active and passive ROM exercises within pain-free limits are encouraged from the outset, focusing on flexion, abduction, and internal/external rotation. Avoid extreme end-range loading or vigorous stretches initially.
- Hip Precautions: Avoid deep flexion, forced internal rotation, and squatting initially to prevent undue stress on the healing physis and minimize impingement.
-
Strengthening:
- Isometric Exercises: Gentle isometric quadriceps and gluteal strengthening can begin early.
- Progressive Strengthening: As pain subsides, progress to isotonic exercises for hip abductors, adductors, flexors, and extensors. Core strengthening is also important.
-
Return to Activity:
- Low-impact activities (e.g., swimming, cycling) can typically resume after 3-4 months, or once radiographic evidence of physeal closure/stable healing is present.
- High-impact sports and strenuous activities are generally restricted until complete physeal closure, usually confirmed by radiographs at 6-12 months post-surgery.
2. Unstable SCFE, Reduction & Fixation:
-
Weight-Bearing:
- Non-Weight-Bearing (NWB): Strict NWB on the affected limb for 6-8 weeks is often recommended to protect the compromised physis and reduce the risk of AVN. This is a critical period for vascular recovery and early healing.
- Partial Weight-Bearing (PWB): Gradual progression to PWB with crutches typically begins after 6-8 weeks, assuming no signs of AVN or further instability.
- Full Weight-Bearing (FWB): FWB is delayed until 3-4 months post-op or longer, contingent on clinical status and radiographic confirmation of stable healing.
- Range of Motion & Strengthening: Similar to stable SCFE, but often with a more cautious and delayed progression, especially in the initial NWB phase. Close monitoring for signs of AVN (e.g., persistent pain, limited ROM, radiographic changes) is paramount.
- Follow-up: More frequent clinical and radiographic follow-up is necessary for unstable slips due to the higher complication rates, particularly AVN.
3. General Considerations for Both Groups:
- Pain Management: Adequate post-operative analgesia is crucial for comfort and compliance with rehabilitation.
- Physical Therapy: Referral to a physical therapist is highly recommended to guide a structured rehabilitation program, focusing on gait training, ROM, and strengthening exercises.
- Radiographic Monitoring: Serial radiographs (AP and lateral) are obtained at regular intervals (e.g., 6 weeks, 3 months, 6 months, 12 months) until physeal closure is complete. This monitors for hardware issues, further slippage, AVN, and confirms physeal closure.
- Hardware Removal: Elective screw removal is generally performed after complete physeal closure, typically 12-18 months post-surgery, or earlier if hardware prominence causes symptoms.
Summary of Key Literature / Guidelines
The body of literature on SCFE has provided robust evidence for current treatment paradigms, while ongoing research continues to refine specific aspects.
-
In Situ
Fixation as Gold Standard:
Numerous studies and long-term follow-up series have consistently demonstrated that
in situ
fixation with a single cannulated screw is the safest and most effective treatment for stable SCFE. It effectively prevents further slip and minimizes iatrogenic complications.
- The Scoliosis Research Society (SRS) and Pediatric Orthopaedic Society of North America (POSNA) guidelines strongly recommend in situ fixation for stable SCFE.
-
Unstable SCFE and AVN Risk:
Unstable SCFE remains the most challenging presentation due to the significantly elevated risk of AVN.
- Early fixation (within 24-48 hours) is critical. The debate continues regarding the role of gentle closed reduction. While some studies suggest cautious, single-attempt reduction may improve long-term hip morphology, others emphasize the paramount importance of avoiding any forceful manipulation to preserve the already compromised retinacular vessels, even if it means accepting a greater residual deformity. The consensus leans towards in situ fixation without aggressive reduction.
-
Prophylactic Contralateral Pinning:
The incidence of contralateral SCFE is high (20-60%), prompting widespread discussion about prophylactic pinning.
- Arguments for: Prevents a potentially unstable slip, reduces the need for multiple operations, and avoids the burden of a second diagnosis. Cost-effectiveness has also been a consideration.
- Arguments against: Risks of AVN, chondrolysis, or other complications in an asymptomatic hip. It also exposes the patient to unnecessary surgery if a slip would not have occurred.
- Current Recommendations: Most surgeons consider prophylactic pinning in patients with high-risk features, such as younger age, severe obesity, or endocrine abnormalities. The decision is often individualized, balancing the risks and benefits in shared decision-making with families.
-
Long-Term Outcomes and FAI:
SCFE, even when successfully treated, often leads to long-term sequelae, primarily Femoroacetabular Impingement (FAI) and premature osteoarthritis.
- The residual metaphyseal bump (cam deformity) and altered head-neck junction contribute to FAI symptoms. Studies indicate that a significant proportion of SCFE patients will develop hip osteoarthritis in adulthood, highlighting the importance of long-term follow-up and consideration for FAI-correcting procedures.
- Mild slips tend to fare better long-term than severe slips. The severity of the initial slip angle is a strong predictor of future hip function and the development of osteoarthritis.
- Screw Placement and Epiphyseal Engagement: Literature consistently highlights that proper screw placement – central in the epiphysis in both AP and lateral views, with adequate epiphyseal purchase (at least 3-4 threads) and avoidance of articular penetration – is paramount for stable fixation and complication prevention. Studies comparing single vs. multiple screws for stable slips generally support a single screw approach due to its equivalent stability and potentially lower complication rate.
In conclusion, the successful management of pediatric SCFE demands a comprehensive understanding of its pathophysiology, meticulous pre-operative planning, precise surgical execution with an emphasis on proper epiphyseal engagement, and diligent post-operative care. While in situ fixation remains the cornerstone, ongoing research into prevention, early detection, and optimal management of long-term sequelae like FAI continues to evolve the field.
You Might Also Like