Complex Pediatric Distal Tibia Physeal Fracture: A Detailed Case Study

Key Takeaway
Complex pediatric distal tibia physeal fractures, often from high-energy rotational trauma, present with severe pain and gross deformity. Diagnosis mandates meticulous clinical examination, assessing neurovascular status and skin integrity. Comprehensive X-rays (AP, lateral, mortise views) are crucial to identify displaced intra-articular fractures and syndesmotic disruption, informing treatment focused on physeal preservation.
Patient Presentation & History
A 10-year-old male was referred to our Level I Pediatric Trauma Center following a high-energy, rotational injury to his right ankle sustained during a competitive soccer match. The patient reports being tackled from behind while his foot was planted, resulting in an immediate "pop" sensation, excruciating pain, and gross deformity. This mechanism, involving axial load combined with rotation, is highly suggestive of complex physeal injuries in skeletally immature patients, often leading to displaced intra-articular fractures of the distal tibia. The energy involved, as evidenced by the "tackled from behind" description in a competitive setting, indicates significant force transmission through the lower extremity. The immediate onset of "pop" and excruciating pain, coupled with gross deformity and inability to bear weight, are cardinal signs of a severe osseous and potentially ligamentous injury rather than a simple sprain. He was unable to bear any weight on the affected limb and was promptly immobilized at the scene by emergency medical services in a vacuum splint before transport, which is appropriate pre-hospital management to minimize further neurovascular compromise or soft tissue damage.
His medical history is unremarkable, with no known allergies, bleeding diatheses, or underlying bone metabolic disorders, which simplifies pre-operative planning and reduces anesthetic risks. He is prepubescent, with Tanner stage II development, indicating open physes and ongoing growth potential. This is a critical factor in pediatric ankle fractures, as treatment must prioritize physeal preservation to prevent growth arrest and subsequent angular deformity or limb length discrepancy. No previous orthopedic injuries or surgeries are noted, suggesting a healthy musculoskeletal system prior to this event. His vaccination status is up-to-date, minimizing infection risks from routine exposures.
Clinical Examination
Upon arrival, the patient was alert, oriented, and hemodynamically stable, with an initial pain score of 9/10, managed effectively with intravenous analgesia.
- Inspection: The right ankle exhibited significant swelling, diffuse ecchymosis extending from the midfoot to the distal tibia, and a palpable, gross deformity. The foot was externally rotated approximately 30-45 degrees and displaced laterally relative to the tibia. There was notable skin tenting over the medial malleolus, raising concern for impending soft tissue compromise and potential conversion to an open fracture if not promptly reduced. This skin tenting indicates severe displacement and tension, which can lead to skin necrosis, blistering, or even frank breach, increasing the risk of infection. Despite the tension, no open wounds or blistering were present on initial inspection. The overall skin integrity was intact, with no signs of blanching or severe skin wrinkling, indicating the skin had not yet progressed to critical ischemia.
- Palpation: Marked tenderness was elicited over the distal metaphyseal region of the tibia, the distal fibula shaft, and the anterolateral aspect of the ankle. Significant pain was also elicited with palpation along the medial and lateral malleoli, as well as the syndesmotic region. There was no tenderness noted proximally over the fibular head or shaft, ruling out a Maisonneuve-type injury. A distinct gap was palpable medially, consistent with severe medial displacement of the talus relative to the tibia.
- Range of Motion (ROM): Active and passive range of motion of the ankle was severely limited and exquisitely painful due to the gross deformity and instability. Attempts at dorsiflexion, plantarflexion, inversion, and eversion were met with significant patient guarding and exacerbation of pain. No crepitus was elicited on gentle palpation during attempted motion, which is often difficult to assess accurately in the presence of significant soft tissue swelling and pain.
- Neurological/Vascular Assessment: Distal neurovascular status was assessed meticulously. The dorsalis pedis and posterior tibial pulses were palpable bilaterally, 2+ and symmetrical, with brisk capillary refill (less than 2 seconds) in all toes. Sensation was intact to light touch in the dermatomes supplied by the superficial and deep peroneal nerves (dorsum of foot, first web space), saphenous nerve (medial ankle), and sural nerve (lateral foot). Motor function of the extensor hallucis longus (deep peroneal), tibialis anterior (deep peroneal), and gastrocnemius-soleus complex (tibial nerve) was difficult to assess accurately due to pain and gross deformity but no obvious paralysis or weakness was noted beyond what would be expected given the injury. There were no signs of impending compartment syndrome, such as disproportionate pain, paresthesias, or pain with passive stretch of the toes.
Imaging & Diagnostics
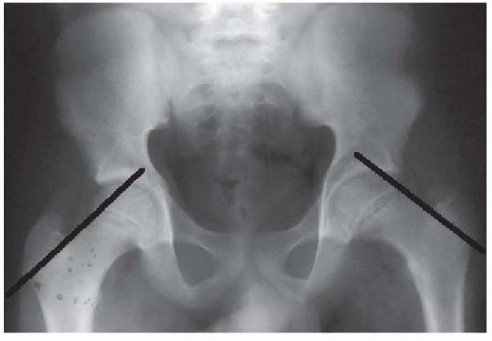
Following clinical assessment, the patient underwent a standard radiographic series of the right ankle, including anteroposterior (AP), lateral, and mortise views. Initial imaging was crucial to characterize the fracture pattern and guide management.
-
X-ray Findings:
-
AP and Mortise Views:
These demonstrated a significantly displaced intra-articular fracture of the distal tibia, extending through the physis and epiphysis. Specifically, there was an obliquely oriented fracture line originating from the metaphysis, extending distally through the physis, and then exiting through the articular surface of the medial malleolus. There was also a separate, laterally displaced epiphyseal fragment involving the lateral aspect of the distal tibia. The talus was laterally and externally rotated relative to the tibial plafond. The fibula appeared intact on the AP view, but the mortise view revealed widening of the tibiofibular clear space and an increased medial clear space, indicating significant syndesmotic disruption and medial instability.

- Lateral View: The lateral view further elucidated the distal tibial fracture morphology. It confirmed the intra-articular extension and demonstrated significant posterior displacement of the distal epiphyseal fragment along with the talus. The fracture configuration, with involvement of both the metaphysis, physis, and epiphysis, and sagittal and coronal plane fracture lines, was highly suggestive of a Triplane fracture of the distal tibia . This type of fracture is characteristic of adolescents due to partial physeal closure, typically occurring in the distal tibia where the physis closes from central to peripheral, and then medial to lateral, and anterior to posterior. The specific pattern identified appeared to be a four-part Triplane fracture (based on initial radiographic assessment implying posterior metaphyseal, lateral epiphyseal, and medial malleolar fragments, with the fibula often intact or minimally involved).
-
AP and Mortise Views:
These demonstrated a significantly displaced intra-articular fracture of the distal tibia, extending through the physis and epiphysis. Specifically, there was an obliquely oriented fracture line originating from the metaphysis, extending distally through the physis, and then exiting through the articular surface of the medial malleolus. There was also a separate, laterally displaced epiphyseal fragment involving the lateral aspect of the distal tibia. The talus was laterally and externally rotated relative to the tibial plafond. The fibula appeared intact on the AP view, but the mortise view revealed widening of the tibiofibular clear space and an increased medial clear space, indicating significant syndesmotic disruption and medial instability.
-
CT Scan Indication: Given the complex, multi-planar nature of the suspected Triplane fracture, with significant articular involvement and displacement, a computed tomography (CT) scan of the ankle was indicated. CT is invaluable in pediatric ankle fractures for several reasons:
- Detailed Fracture Morphology: It provides a precise 3D understanding of the fracture lines, articular step-off, and fragment orientation, which is often poorly visualized on plain radiographs due to superimposition, especially in Triplane fractures with their characteristic components in sagittal, coronal, and axial planes.
- Articular Congruity Assessment: Crucial for surgical planning, CT helps quantify articular displacement and step-off, which are direct predictors of post-traumatic arthritis.
- Physeal Involvement: Better delineates the extent of physeal injury, aiding in the assessment of potential growth arrest risk.
- Fragment Identification: Identifies entrapped periosteum or osteochondral fragments within the joint that may impede reduction.
-
Syndesmotic Integrity:
While syndesmotic widening was evident on X-rays, CT can provide a more definitive assessment of diastasis and rotation, particularly through axial cuts.
A CT scan was performed and confirmed a complex, comminuted Triplane fracture of the distal tibia, involving the metaphysis, physis, and epiphysis, with significant intra-articular displacement of the posterolateral epiphyseal fragment. There was also evidence of syndesmotic disruption. The CT scan provided the necessary detail to plan the surgical approach and fixation strategy to achieve anatomical reduction of the articular surface.
-
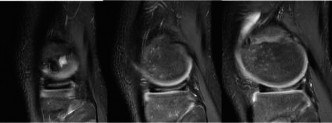
MRI Indications: Magnetic resonance imaging (MRI) was not deemed immediately necessary for acute surgical planning in this case, as the CT provided sufficient detail regarding the osseous and articular injury. However, MRI may be considered in cases of:
- Suspected ligamentous injury not apparent on other imaging (e.g., deltoid ligament or interosseous membrane injury).
- Concern for chondral injury or osteochondral lesions not well visualized on CT.
- Evaluation of physeal bar formation or growth arrest in the post-operative period, if complications arise.
-
Templating: Pre-operative templating based on the CT scan was performed to anticipate the size and type of fixation hardware. This involved determining the optimal entry points and trajectories for cannulated screws to achieve stable fixation while minimizing physeal violation. Small-diameter, fully threaded cannulated screws (e.g., 3.5 mm) or K-wires are typically preferred in pediatric physeal fractures. The goal was to select hardware that would provide sufficient stability for healing without crossing the open physis perpendicular to its growth axis unnecessarily or causing compression across it.
Differential Diagnosis
The presentation of a high-energy rotational ankle injury in a 10-year-old warrants a detailed differential diagnosis to ensure accurate classification and appropriate management.
| Feature | Triplane Fracture (Most Likely) | Tillaux Fracture | Salter-Harris Type III Distal Tibia | Severe Ankle Sprain / Syndesmotic Injury (Less Likely with Gross Deformity) |
|---|---|---|---|---|
| Mechanism | Rotational (external rotation of foot on fixed tibia), typically higher energy. | External rotation and abduction, often lower energy than triplane. | Rotational (external rotation), abduction, or adduction. | Inversion/eversion (lateral/medial sprain), external rotation (syndesmotic). |
| Age Group | Late adolescent (12-16 years), partial physeal closure. Can occur younger (as in this case, 10-year-old) if physeal closure patterns allow. | Late adolescent (12-16 years), partial physeal closure, anterolateral physis last to close. | Any age with open physis, but Type III usually later childhood/adolescence. | Any age. |
| Clinical Features | Gross deformity, severe pain, swelling, skin tenting. Significant articular displacement. Often associated with syndesmotic injury. | Localized pain/tenderness over distal anterolateral tibia. Less gross deformity unless severely displaced. | Localized pain, swelling, tenderness over epiphysis/physis. Articular step-off if displaced. Variable deformity. | Localized pain, swelling, ecchymosis. Ligamentous tenderness. Stability assessed with stress tests. Less gross deformity. |
| X-ray Findings | Complex intra-articular fracture: AP, lateral, mortise views show fracture lines in different planes (metaphyseal, physeal, epiphyseal). Typically 2, 3, or 4 fragments. | AP view shows fracture through distal tibial epiphysis, parallel to physis, involving anterolateral corner. Variable displacement. | Fracture line through physis, exiting into epiphysis (articular surface). Requires AP, lateral, and mortise views for classification. | Soft tissue swelling. Widened mortise, increased tibiofibular clear space (syndesmotic). No obvious fracture. |
| CT/MRI Role | Essential for understanding 3D morphology, articular step-off, and surgical planning. | Beneficial for precise articular assessment and displacement. | Beneficial for detailed articular congruity, especially in cases of suspected displacement or comminution. | MRI for definitive ligamentous integrity, particularly syndesmotic. CT if occult fracture suspected. |
| Treatment | Anatomical ORIF (cannulated screws or K-wires) if displaced (>2mm articular step-off or >2mm physeal displacement). | ORIF if displaced (>2mm articular step-off), often with cannulated screw. Closed reduction if minimally displaced. | ORIF if displaced (>2mm articular step-off or >2mm physeal displacement). Closed reduction if stable. | RICE, immobilization. ORIF for unstable syndesmotic injury or avulsion fracture. |
| Prognosis | Good with anatomical reduction. Risk of growth arrest, physeal bar, post-traumatic arthritis if malreduced. | Good with anatomical reduction. Risk of growth arrest, post-traumatic arthritis. | Good with anatomical reduction. Risk of growth arrest (physeal bar), post-traumatic arthritis. | Good, but chronic instability and pain if syndesmotic injury untreated. |
The patient's gross deformity, severe multi-planar displacement evident on initial radiographs, and the characteristic age group for transitional fractures, strongly pointed towards a Triplane fracture of the distal tibia. This was definitively confirmed by the CT scan, illustrating the critical role of advanced imaging in such complex cases.
Surgical Decision Making & Classification
The primary surgical decision in this case was dictated by the significant displacement of the intra-articular distal tibial fracture, specifically a Triplane fracture, and the associated gross deformity with impending skin compromise.
Why Operative vs. Non-Operative?
*
Displacement:
The CT scan demonstrated significant articular step-off (>2mm) and physeal displacement (>2mm), which are absolute indications for surgical intervention in pediatric ankle fractures, especially those involving the articular surface. Anatomical reduction of the articular surface is paramount to prevent post-traumatic arthritis.
*
Instability:
The gross deformity and widening of the syndesmosis indicated an unstable fracture pattern that would not achieve acceptable reduction or stability with closed methods alone.
*
Impending Soft Tissue Compromise:
The severe skin tenting over the medial malleolus, while not yet an open fracture, mandated urgent reduction to prevent further skin necrosis, blistering, or even frank breach, which would complicate treatment and increase infection risk.
*
Fracture Type:
Triplane fractures, due to their complex multi-planar nature and intra-articular involvement, frequently require open reduction and internal fixation (ORIF) to achieve anatomical alignment. Closed reduction can be attempted, but typically only achieves acceptable results in minimally displaced or less complex patterns.
Classification:
The fracture was classified as a
Triplane fracture of the distal tibia
. This is a specific type of physeal fracture occurring during the period of physeal closure, typically between 12-16 years, but can occur younger as in this case (10 years old) due to individual variations in growth plate maturation. It involves fracture lines in three anatomical planes:
1.
Sagittal plane:
Through the epiphysis (often posterolateral).
2.
Transverse plane:
Through the physis (Salter-Harris I component).
3.
Coronal plane:
Through the metaphysis (often posterior).
Further characterization is typically done by the number of fragments observed on axial CT cuts (e.g., two-part, three-part, four-part). In this case, the CT scan elucidated a
four-part Triplane fracture
based on the following:
* An anteromedial epiphyseal fragment (tibia, part of the distal articular surface).
* A posterolateral epiphyseal fragment (tibia, part of the distal articular surface).
* A metaphyseal fragment (posterior aspect of distal tibia).
* The remainder of the distal tibia and fibula.
The concurrent widening of the tibiofibular clear space and medial clear space indicated significant disruption of the syndesmosis and deltoid ligament complex, further supporting the need for operative stabilization. While technically not a Salter-Harris classification directly, it contains Salter-Harris Type I (physeal) and Type III/IV (epiphyseal/metaphyseal) components. The unique pattern necessitates specific surgical techniques.
Surgical Technique / Intervention
The patient was taken to the operating room urgently for open reduction and internal fixation (ORIF) of the right distal tibial Triplane fracture.
-
Patient Positioning: The patient was positioned supine on the operating table. A high thigh tourniquet was applied to the right leg but not inflated initially. A radiolucent bolster was placed under the ipsilateral hip to internally rotate the leg and present the ankle neutrally. The foot of the bed was removed, and the leg was draped free to allow for full range of motion of the ankle and easy access for fluoroscopy. A C-arm was positioned to allow for clear AP, lateral, and mortise views of the ankle throughout the procedure.
-
Initial Reduction Attempt & Preparation:
Prior to incision, a gentle attempt at closed reduction was performed under general anesthesia. This involved traction to length, followed by internal rotation and correction of the lateral displacement. While this maneuver partially improved the gross deformity and relieved some skin tension, complete anatomical reduction of the articular surface was not achieved, as confirmed by fluoroscopy. The skin tenting was also significantly improved, lessening the urgency for immediate open reduction. The leg was prepped and draped in a sterile fashion. -
Surgical Approach:
Given the complex nature of the fracture and the significant displacement of the anteromedial and posterolateral epiphyseal fragments, a dual approach was deemed necessary to achieve anatomical reduction and stable fixation.- Anteromedial Approach: A 5-cm longitudinal incision was made over the anteromedial aspect of the distal tibia, directly overlying the medial malleolus. The incision was deepened through the subcutaneous tissue. The saphenous vein and nerve were identified and protected. The periosteum was incised longitudinally and reflected sparingly to expose the fracture site, specifically the medial malleolar fragment and the articular surface.
- Anterolateral Approach: A second, 4-cm longitudinal incision was made over the anterolateral aspect of the distal tibia, extending distally towards the talar dome. This approach provided access to the lateral epiphyseal fragment and the syndesmotic region. Care was taken to protect the superficial peroneal nerve.
-
Reduction Techniques:
The goal was to restore the articular congruity of the distal tibia precisely.- Syndesmotic Reduction: With the anterolateral incision providing direct visualization, attention was first directed to the syndesmosis. The widened tibiofibular clear space was reduced. The interosseous membrane and anterior inferior tibiofibular ligament were carefully inspected.
-
Epiphyseal Fragment Reduction:
Using blunt elevators and reduction clamps, the large anteromedial and posterolateral epiphyseal fragments were carefully manipulated under direct visualization and fluoroscopic guidance. The key was to reduce the primary epiphyseal fragments anatomically to the tibial shaft, restoring the articular congruity. Traction was maintained on the foot to distract the joint slightly and allow for better visualization and manipulation. Small K-wires were used as joysticks to control and rotate fragments. Once the articular surface was anatomically reduced, temporary K-wires (1.6mm) were used to stabilize the epiphyseal fragments to each other and to the distal tibia, avoiding the physis as much as possible. Fluoroscopy confirmed anatomical reduction in AP, lateral, and mortise views.
-
Fixation Construct:
After achieving anatomical reduction and temporary K-wire stabilization, definitive fixation was performed.- Medial Malleolus/Epiphyseal Fixation: Through the anteromedial approach, two 3.5 mm fully threaded cannulated screws were inserted. These screws were directed from the medial malleolus, across the reduced epiphyseal fragment, and into the metaphysis of the distal tibia. Care was taken to aim parallel to the physis, or through non-weight-bearing parts of the physis if unavoidable, to minimize the risk of physeal arrest. The cannulated technique allowed for precise placement over guidewires.
- Lateral Epiphyseal/Syndesmotic Fixation: Through the anterolateral approach, a third 3.5 mm fully threaded cannulated screw was inserted. This screw was directed from the lateral aspect of the distal tibia, engaging the reduced lateral epiphyseal fragment and providing additional stability to the articular block. This screw also helped maintain the syndesmotic reduction.
-
Syndesmotic Screw (Optional):
Given the resolution of syndesmotic widening after fracture reduction and stable screw fixation, a dedicated syndesmotic screw was not deemed necessary in this particular case. However, if syndesmotic instability persisted after definitive fracture fixation, a single 3.5 mm tricortical syndesmotic screw could have been placed 2-3 cm proximal to the physis, parallel to the joint, to stabilize the distal tibiofibular articulation. This would typically be removed at 6-8 weeks post-op to prevent growth arrest or hardware breakage.
Final fluoroscopic images confirmed excellent anatomical reduction of the articular surface, stable fixation, and appropriate hardware placement relative to the physis. The mortise was symmetrical, and the syndesmotic clear space was restored.
-
Wound Closure:
The tourniquet was deflated. Hemostasis was achieved. The wounds were irrigated thoroughly. The periosteum was reapproximated where possible. Subcutaneous tissues were closed with absorbable sutures, and the skin was closed with non-absorbable sutures. A sterile dressing was applied, followed by a well-padded short leg plaster splint in a neutral ankle position.
Post-Operative Protocol & Rehabilitation
The post-operative protocol for a complex distal tibial Triplane fracture aims to protect the repair, allow for bone healing, and prevent complications while facilitating functional recovery.
-
Initial Immobilization (Weeks 0-6):
-
Phase 1 (Weeks 0-2):
Immediately post-operatively, the patient was immobilized in a well-padded short leg plaster splint in a neutral position.
- Elevation of the limb and ice application were emphasized to minimize swelling.
- Non-weight-bearing (NWB) status on the operative limb was strictly enforced.
- Pain management and regular neurovascular checks were performed.
-
Phase 2 (Weeks 2-6):
At the first post-operative visit (typically 10-14 days), the splint was removed, surgical wounds were inspected, and sutures were removed. A new, non-removable short leg fiberglass cast was applied.
- NWB status continued.
- Gentle, non-weight-bearing range of motion exercises for the knee and hip were encouraged to prevent stiffness.
-
Phase 1 (Weeks 0-2):
Immediately post-operatively, the patient was immobilized in a well-padded short leg plaster splint in a neutral position.
-
Progressive Weight-Bearing (Weeks 6-12):
- Radiographic Assessment (Week 6): At 6 weeks post-op, follow-up radiographs (AP, lateral, mortise views) were obtained to assess fracture healing and alignment. Signs of early callus formation and bridging were expected.
-
Transition to Controlled Weight-Bearing:
If radiographic healing was satisfactory and the patient reported minimal pain, the cast was converted to a removable CAM walker boot.
- Partial Weight-Bearing (PWB): The patient was allowed to begin partial weight-bearing (25-50% body weight) with crutches.
-
Physical Therapy (PT) Initiation:
Formal physical therapy commenced. Initial goals focused on:
- Restoring ankle range of motion (dorsiflexion, plantarflexion, inversion, eversion).
- Initiating gentle isometric strengthening exercises for ankle musculature.
- Gait training with PWB.
-
Progression to Full Weight-Bearing (Weeks 8-12):
As pain tolerance improved and radiographic healing progressed, weight-bearing was gradually advanced to full weight-bearing (FWB) in the CAM walker, typically by 8-10 weeks.
- PT progressed to incorporate progressive resistive exercises for ankle strength, proprioceptive training (balance board), and endurance activities.
-
Return to Activity & Sport (Weeks 12+):
- Hardware Considerations: Given that the hardware (cannulated screws) was placed to avoid or minimize physeal disruption, routine removal is not always necessary unless symptomatic (e.g., pain, prominence, irritation). In this case, the decision for hardware removal would be made on a case-by-case basis, typically after 6-12 months if growth disturbance is a concern or if symptomatic.
-
Advanced Rehabilitation:
Once FWB was achieved without pain and muscle strength was symmetrical, the patient transitioned out of the CAM walker.
- Return to sport-specific drills, agility training, and plyometrics under the guidance of a physical therapist.
- Emphasis on single-leg balance, jumping, and cutting maneuvers.
- Psychological readiness for return to sport was also addressed.
-
Return to Sport Criteria:
Full return to competitive soccer was anticipated at approximately 4-6 months post-operatively, provided:
- Full, pain-free range of motion.
- Symmetrical strength (e.g., >90% contralateral limb on isokinetic testing).
- Excellent dynamic stability and proprioception.
-
Radiographic evidence of complete fracture consolidation.
- Long-Term Follow-up: The patient will require long-term follow-up to monitor for potential complications such as growth arrest (physeal bar formation), angular deformity, limb length discrepancy, or post-traumatic arthritis, which can manifest years after the initial injury. Radiographic surveillance for physeal bridging is crucial during the growth phase.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- High Index of Suspicion for Complex Injuries: In adolescents and pre-adolescents presenting with high-energy ankle trauma and gross deformity, always suspect complex intra-articular fractures like Triplane or Tillaux fractures, even if initial plain radiographs appear equivocal.
- Mandatory CT Scan for Transitional Fractures: For any suspected Triplane or Tillaux fracture, a CT scan is essential for definitive diagnosis, characterization of fragment orientation and displacement, and meticulous pre-operative planning. Plain films alone are often insufficient to fully delineate these 3D fractures.
- Prioritize Articular Congruity: Anatomical reduction of the articular surface is the single most critical factor in preventing long-term post-traumatic arthritis. Even small step-offs (>1-2mm) can lead to accelerated degenerative changes.
- Physeal Sparing Fixation: In skeletally immature patients, hardware placement must respect the open physis. Use small-diameter, fully threaded screws or K-wires aimed parallel to the physis or through the epiphysis/metaphysis where possible. If screws must cross the physis, they should be fully threaded and perpendicular to minimize compression and growth arrest.
- Address Associated Injuries: Always assess for and address associated injuries, especially syndesmotic instability, which is common with Triplane fractures. If residual instability exists after fracture fixation, consider a temporary syndesmotic screw.
- Urgency for Soft Tissue Compromise: Gross displacement leading to skin tenting or impending open fracture warrants urgent reduction (closed or open) to prevent skin necrosis, infection, and further complications.
Pitfalls
- Inadequate Imaging: Relying solely on plain radiographs for complex intra-articular pediatric ankle fractures will lead to missed components, inaccurate classification, and potentially suboptimal treatment.
- Incomplete Reduction: Failure to achieve true anatomical reduction of the articular surface, particularly of the epiphyseal fragments, is a common pitfall. This often necessitates open reduction and direct visualization of the joint. Fluoroscopy alone can sometimes be misleading, highlighting the value of direct visualization through appropriate surgical approaches.
- Physeal Injury from Hardware: Incorrect hardware placement (e.g., partially threaded screws compressing the physis, screws crossing the physis at too steep an angle) can lead to premature physeal closure, angular deformity, and limb length discrepancy.
- Missed Syndesmotic Instability: Failure to diagnose or adequately stabilize a syndesmotic injury can result in chronic ankle pain, instability, and accelerated wear of the ankle joint.
- Over-reliance on Closed Reduction: While desirable, closed reduction of significantly displaced Triplane fractures often fails to achieve acceptable articular congruity. Persistence with closed methods when an open reduction is clearly indicated delays definitive treatment and can worsen soft tissue compromise.
- Premature Weight-Bearing: Allowing weight-bearing too early before adequate fracture healing can lead to loss of reduction, hardware failure, or delayed union. Adherence to a structured, radiographic-guided rehabilitation protocol is vital.
- Failure to Monitor for Complications: Long-term follow-up is critical to monitor for growth arrest, physeal bar formation, angular deformity, or early signs of post-traumatic arthritis. These complications can arise years after the initial injury and may require further intervention.
Clinical & Radiographic Imaging
You Might Also Like