Three-Stage Reconstruction for Pelvic Malunions: A Comprehensive Surgical Guide
Key Takeaway
Three-stage reconstruction for pelvic malunions is a complex, highly demanding procedure designed to restore pelvic ring symmetry, correct leg-length discrepancy, and alleviate chronic pain. This sequential approach—typically alternating between supine and prone positions—allows for comprehensive mobilization of both anterior and posterior pelvic segments. By systematically releasing contracted ligaments and osteotomizing healed deformities, surgeons can achieve anatomical reduction and rigid internal fixation, ultimately restoring optimal pelvic biomechanics and patient function.
INTRODUCTION TO PELVIC MALUNION RECONSTRUCTION
Pelvic ring malunions represent one of the most formidable challenges in orthopedic trauma and reconstructive surgery. These complex deformities typically arise from missed injuries, failed conservative management of unstable fractures, or loss of fixation in the postoperative period. The resulting biomechanical derangements are profound, often manifesting as severe leg-length discrepancies, sitting imbalance, compensatory lumbar scoliosis, and debilitating chronic pelvic pain.
Because the pelvis heals rapidly, deformities become rigidly fixed within a matter of weeks. The surrounding soft tissues—including the pelvic floor musculature, the lumbosacral plexus, and the robust ligamentous complexes—contract and adapt to the distorted anatomy. Consequently, acute fracture reduction techniques are entirely ineffective for delayed presentations.
To overcome these rigid, multiplanar deformities, a sequential, multi-stage surgical approach is required. The Three-Stage Reconstruction is the gold standard for severe pelvic malunions, allowing the surgeon to systematically osteotomize healed bone, release contracted soft tissues, and sequentially mobilize the hemipelvis before achieving final reduction and rigid internal fixation.
PREOPERATIVE EVALUATION AND BIOMECHANICAL CONSIDERATIONS
Clinical Assessment
Patients with pelvic malunions typically present with a constellation of mechanical and neurological symptoms. A thorough clinical evaluation must quantify:
* Leg-Length Discrepancy (LLD): Cranial migration of the hemipelvis results in a true shortening of the affected lower extremity.
* Sitting Imbalance: Rotational deformities (especially internal or external rotation of the hemipelvis) alter the spatial relationship of the ischial tuberosities, making sitting painful or impossible without leaning.
* Neurological Deficits: The lumbosacral plexus (L4-S4) is highly susceptible to traction or compression injuries during the initial trauma or subsequent malunion. Baseline electromyography (EMG) and nerve conduction studies (NCS) are mandatory.
* Urogenital Function: Assessment of bladder, bowel, and sexual function is critical, as these may be compromised by the initial injury or tethered by the malunion.
Advanced Imaging and Templating
Standard anteroposterior (AP), inlet, and outlet pelvic radiographs provide a baseline understanding of the deformity. However, surgical planning relies entirely on advanced imaging:
* High-Resolution CT with 3D Reconstruction: Essential for defining the exact planes of the malunion, identifying areas of heterotopic ossification, and planning osteotomy trajectories.
* CT Angiography (CTA): Highly recommended to map the pelvic vasculature. The iliac vessels and their branches (e.g., the obturator artery and the corona mortis) often become encased in scar tissue or callus, significantly increasing the risk of catastrophic intraoperative hemorrhage.
* 3D Printed Models: In contemporary practice, 3D printing a life-sized model of the patient's malunited pelvis allows for tactile preoperative planning, pre-contouring of reconstruction plates, and precise calculation of osteotomy angles.
Clinical Pearl: Always template the osteotomies at the sites of the original injury. Attempting to create compensatory osteotomies in native, uninjured bone often leads to secondary deformities and incongruent joint surfaces.
OPERATING ROOM SETUP AND POSITIONING
The three-stage procedure requires multiple patient repositionings, demanding meticulous coordination with the anesthesia and nursing teams.
Equipment Requirements
- Radiolucent Operating Table: Essential for unobstructed fluoroscopic imaging in multiple planes (AP, inlet, outlet, and Judet views).
- Judet Traction Table: In cases with severe cranial displacement, a Judet table or a skeletal traction setup (via a distal femoral pin) is highly advantageous. It provides sustained, controlled longitudinal traction to overcome soft tissue contractures.
- High-Quality Fluoroscopy: Two C-arms can be utilized simultaneously to save time during complex multiplanar reductions.
- Intraoperative External Fixators: Used as temporary reduction tools ("joysticks") to manipulate the hemipelvis.
THE THREE-STAGE SURGICAL TECHNIQUE: SUPINE-PRONE-SUPINE
The classic three-stage approach alternates the patient between supine and prone positions. This sequence ensures that tethering structures are released sequentially, preventing the surgeon from fighting opposing fixed points.
Stage 1: Anterior Mobilization (Supine Position)
The primary goal of the first stage is to release the anterior tether. No definitive fixation is applied during this stage.
- Surgical Approach: An ilioinguinal approach or a modified Stoppa approach is utilized, depending on the location of the anterior malunion (symphysis pubis vs. superior/inferior pubic rami).
- Vascular Control: The external iliac vessels and the corona mortis are carefully identified and protected. Scar tissue often obscures these structures; meticulous dissection is paramount.
- Osteotomy: The deformed anterior pelvic structures are osteotomized using an oscillating saw or osteotomes. If an anterior nonunion is present, the fibrous tissue is excised, and the bone ends are mobilized.
- Soft Tissue Release: The rectus abdominis insertions or adductor origins may require partial release if they are severely contracted.
- Closure: Hemostasis is achieved, a drain is placed, and the anterior wound is temporarily closed.
Surgical Warning: Do not attempt to reduce the anterior ring during Stage 1. The posterior ring remains rigidly fixed, and forceful anterior manipulation will only result in iatrogenic fractures or vascular injury.
Stage 2: Posterior Mobilization, Reduction, and Fixation (Prone Position)
The patient is carefully log-rolled into the prone position. This is the most critical and technically demanding stage of the reconstruction.
- Surgical Approach: A posterior longitudinal or paramedian approach is utilized to access the sacroiliac (SI) joint, sacrum, and posterior ilium.
- Posterior Osteotomy: The posterior pelvic deformities (e.g., a healed sacral fracture or a malunited SI joint fracture-dislocation) are osteotomized. The cuts must follow the original fracture lines.
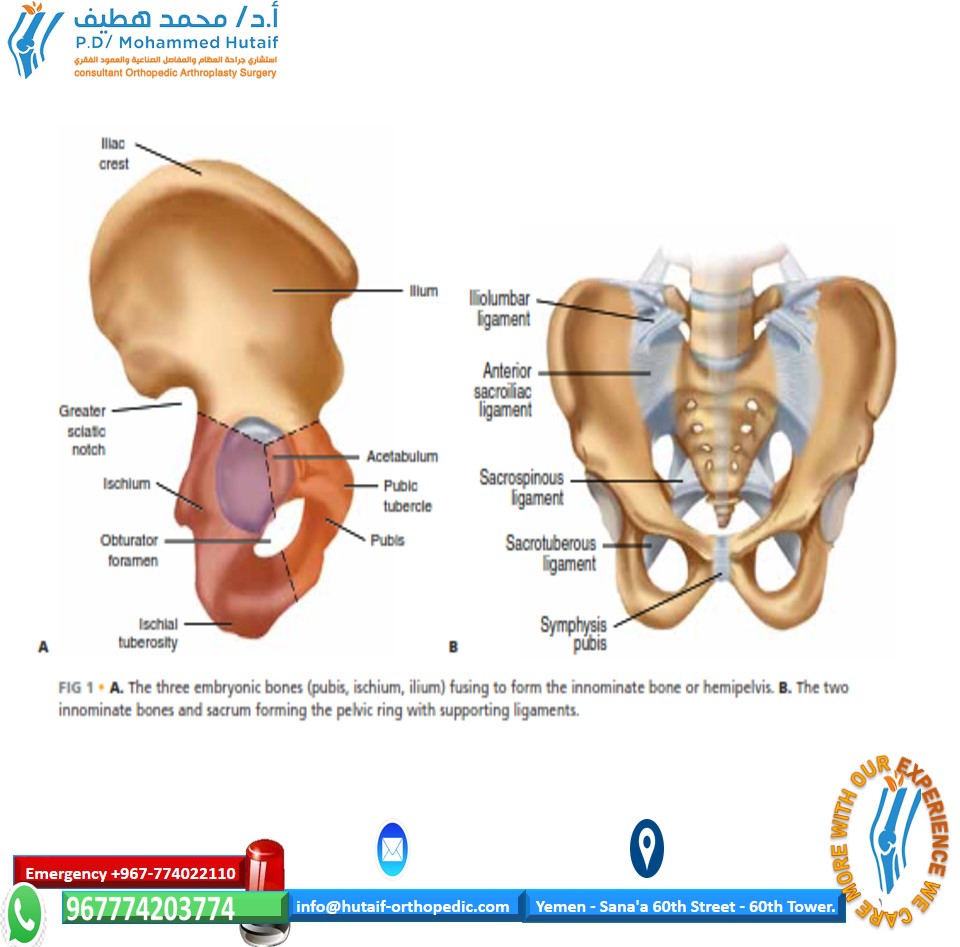
- Ligamentous Release (The Key to Cranial Correction): Correction of cranial displacement is notoriously difficult. It is made significantly easier by dividing the attachments of the sacrospinous and sacrotuberous ligaments to the sacrum. These ligaments act as massive tethers; releasing them allows the hemipelvis to be mobilized caudally.
- Reduction:
- Schanz pins (5.0mm or 6.0mm) are placed into the posterior ilium to act as joysticks.
- An intraoperative external fixator or a specialized pelvic reduction frame (e.g., a Farabeuf clamp or Jungbluth clamp) is applied to manipulate the hemipelvis.
- Longitudinal traction is applied to correct cranial migration, while rotational forces are applied to correct internal/external rotation.
- Posterior Fixation: Once anatomical or near-anatomical reduction is confirmed via fluoroscopy (inlet/outlet views), rigid internal fixation is applied.
- Implants: Large iliosacral screws (7.0mm or 7.3mm) are placed into the S1 and/or S2 vertebral bodies.
- Supplemental Fixation: Because old deformities are highly resistant to correction and exert massive deforming forces, stronger fixation is required compared to acute fractures. Posterior tension band plates or transiliac-transsacral screws are often necessary to prevent loss of reduction.
- Closure: The posterior wound is irrigated, drained, and closed in layers.
Stage 3: Anterior Reduction and Fixation (Supine Position)
The patient is returned to the supine position for the final stage.
- Reopening: The initial anterior wound is reopened.
- Final Reduction: Because the posterior ring is now anatomically reduced and rigidly fixed, the anterior ring will often fall into a much-improved alignment. Minor adjustments are made using Weber clamps or pelvic reduction forceps.
- Anterior Fixation: The anterior structures are stabilized using robust plate fixation. Multi-hole symphyseal plates or 3.5mm reconstruction plates (often double-plated) are utilized.
- Bone Grafting: Any residual osseous defects at the osteotomy sites are packed with autologous bone graft (typically harvested from the iliac crest) or high-quality allograft to promote union.
- Final Closure: The wound is closed meticulously over suction drains.
ALTERNATIVE SEQUENCING: PRONE-SUPINE-PRONE
While the Supine-Prone-Supine sequence is standard, the procedure can be performed in the opposite order:
1. Mobilizing the posterior pelvis first.
2. Mobilizing, reducing, and internally fixing the anterior pelvis.
3. Completion of reduction and fixation of the posterior pelvis.
Indications for Alternative Sequencing:
This sequence is highly beneficial when the primary driver of the malunion is a massive posterior deformity (e.g., a severely impacted sacral fracture) that requires extensive initial debridement and mobilization before any anterior work can be conceptualized. It allows the surgeon to assess the mobility of the posterior ring before committing to anterior fixation.
THE TWO-STAGE ALTERNATIVE: EVIDENCE AND OUTCOMES
While the three-stage procedure is the historical gold standard, some authors advocate for a streamlined two-stage approach to reduce operative time and morbidity.
The Rousseau et al. Study
Rousseau et al. reported a prone-supine, two-stage procedure in a cohort of eight patients with a 10-month follow-up.
* Stage 1 (Prone): The surgery consisted of opening the sacroiliac joint and cutting the sacrotuberous and sacrospinous ligaments through a posterior approach.
* Stage 2 (Supine): The pubic symphysis and the anterior aspect of the sacroiliac joint were released through an ilioinguinal approach. Reduction was achieved, followed by osteosynthesis of the pubic symphysis and sacroiliac joint, including bone graft harvesting and grafting.
Outcomes of the Two-Stage Approach:
* Anatomical reduction was achieved in six of the eight patients.
* In the two patients without anatomical reduction, mechanical problems stemming from persistent leg-length inequality remained.
Pitfall: The two-stage approach requires the surgeon to achieve posterior reduction from an anterior approach (during Stage 2). This is technically demanding and may not provide the same mechanical leverage as direct posterior manipulation, potentially leading to the residual leg-length discrepancies noted in the study.
COMPLICATIONS AND RISK MANAGEMENT
Pelvic malunion reconstruction is fraught with potential complications due to the extensive surgical exposures, prolonged operative times, and the massive forces required to mobilize contracted tissues.
In a landmark study evaluating the three-stage technique, 36 of 37 patients achieved stable unions of the pelvic ring. However, the overall incidence of complications was 19%. No infections were reported in this specific cohort, but the complication profile remains significant:
1. Neurological Injury (Lumbosacral Plexus)
- Mechanism: The most common neurological complication is a motor deficit, frequently presenting as a footdrop (L5/S1 nerve root injury). In the Rousseau study, three patients developed motor deficits with footdrop.
- Pathophysiology: This occurs due to acute traction on the lumbosacral trunk during the correction of severe cranial displacement. The nerve, having shortened during the malunion phase, is acutely stretched when the hemipelvis is pulled caudally.
- Prevention: Intraoperative neuromonitoring (SSEP and MEP) is highly recommended. If nerve signals degrade during traction, the surgeon must accept a sub-optimal reduction to preserve neurological function.
2. Vascular Injury
- Mechanism: Laceration or avulsion of the iliac vessels, obturator artery, or superior gluteal artery.
- Prevention: Meticulous dissection, preoperative CTA, and avoiding blind placement of retractors (such as Hohmann retractors over the pelvic brim).
3. Loss of Reduction and Persistent Nonunion
- Mechanism: Inadequate fixation strength against the massive deforming forces of contracted soft tissues.
- Prevention: As noted, old deformities require stronger fixation than acute fractures. Use multiple large-diameter iliosacral screws, supplemental posterior plating, and generous autologous bone grafting at all osteotomy sites.
4. Urological Injury
- Mechanism: Bladder or urethral injury during anterior mobilization (one bladder injury was reported in the Rousseau cohort).
- Prevention: Preoperative placement of a Foley catheter to decompress the bladder. Careful sharp dissection of the retropubic space (Space of Retzius), as the bladder is often densely adherent to the posterior aspect of a malunited pubic symphysis.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of a three-stage pelvic reconstruction requires a delicate balance between protecting the extensive osteosyntheses and preventing the complications of prolonged immobility.
- Weight-Bearing Status: Patients are typically restricted to strict non-weight-bearing or toe-touch weight-bearing (TTWB) on the affected side for a minimum of 8 to 12 weeks.
- Deep Vein Thrombosis (DVT) Prophylaxis: Given the extensive pelvic surgery and prolonged operative time, patients are at an exceptionally high risk for venous thromboembolism. Chemical prophylaxis (e.g., Low Molecular Weight Heparin) is mandatory for 4 to 6 weeks postoperatively, barring any contraindications.
- Physical Therapy: Early mobilization out of bed to a chair is encouraged. Passive and active-assisted range of motion exercises for the hip, knee, and ankle are initiated immediately to prevent contractures and promote gliding of the lumbosacral nerve roots.
- Radiographic Follow-up: Serial radiographs (AP, inlet, outlet) are obtained at 2, 6, and 12 weeks to monitor for loss of reduction and assess the progression of bony union at the osteotomy sites.
CONCLUSION
The three-stage reconstruction for pelvic malunions is a master-level orthopedic procedure that demands a profound understanding of pelvic anatomy, biomechanics, and soft-tissue behavior. By meticulously planning the sequence of osteotomies and soft-tissue releases—particularly the critical division of the sacrospinous and sacrotuberous ligaments—surgeons can overcome rigid deformities. While the complication rates reflect the inherent complexity of the pathology, successful execution of this sequential approach reliably restores pelvic ring stability, corrects leg-length discrepancies, and significantly improves the patient's quality of life.
You Might Also Like