Adolescent Tibial Tuberosity Fractures: What Parents Need to Know
Key Takeaway
Your ultimate guide to Adolescent Tibial Tuberosity Fractures: What Parents Need to Know starts here. Tibial tuberosity fractures are rare apophyseal fractures primarily affecting adolescent boys during the onset of proximal tibial physeal closure. These injuries typically occur with a forceful quadriceps contraction, often at the initiation of a jump, when the foot is fixed. They involve the anterolateral tibial tubercle, where the patellar ligament inserts, sometimes associated with Osgood-Schlatter syndrome.
Introduction and Epidemiology
Tibial tuberosity fractures represent a rare but highly significant subset of pediatric orthopedic injuries, predominantly affecting adolescents nearing the completion of proximal tibial physeal closure. Accounting for approximately 0.4% to 2.7% of all epiphyseal injuries, these apophyseal avulsion fractures occur almost exclusively in adolescent males, typically between the ages of 13 and 16 years. While the incidence in females is markedly lower, cases are documented, usually occurring at a slightly younger age demographic (11 to 14 years) commensurate with their earlier skeletal maturation.
The injury mechanism is intimately linked to athletic participation. Most commonly, the fracture occurs during the initiation of a jump or upon a forceful landing, activities ubiquitous in sports such as basketball, volleyball, and track and field. The association with prior tibial tuberosity traction apophysitis, clinically recognized as Osgood-Schlatter syndrome, is a well-documented predisposing factor. Chronic traction apophysitis induces microtrauma and subsequent structural weakening of the secondary ossification center, rendering the tuberosity susceptible to acute catastrophic failure under maximal eccentric quadriceps loading.
Understanding the epidemiology and the unique temporal vulnerability of the tibial apophysis is critical for the orthopedic surgeon. The transition from a cartilaginous apophysis to a fused bony structure creates a transient mechanical weak point. As sports participation and training intensities among adolescents continue to rise, the clinical index of suspicion for these fractures and their associated complications must remain high.
Surgical Anatomy and Biomechanics
The anatomical development and biomechanical environment of the proximal tibia dictate the pathogenesis and fracture patterns observed in adolescent tibial tuberosity avulsions. The tibial tubercle is situated in an anterolateral location on the proximal tibia, just distal to the main proximal tibial physis.
Apophyseal Development and Ossification
The development of the tibial tubercle progresses through four distinct anatomical stages, which are paramount to understanding the etiology of these fractures.
Stage 1 is the cartilaginous stage, where the tubercle exists entirely as a cartilage anlage without a secondary center of ossification.
Stage 2, known as the apophyseal stage, occurs between ages 8 and 12 years in girls and 9 and 14 years in boys. During this phase, the secondary center of ossification appears but remains anatomically separate and not contiguous with the epiphyseal ossification of the proximal tibia.
Stage 3, the epiphyseal stage, represents the period of highest vulnerability. This occurs when the apophyseal ossification coalesces and connects with the epiphyseal bone, typically between ages 10 and 15 years for girls and 11 and 17 years for boys.
Stage 4 is defined by the complete fusion of the tubercle and the definitive closure of the apophyseal cartilage.

The closure of the proximal tibial physis and the tubercle apophysis follows a highly predictable and specific spatial pattern. The proximal tibial physis closes in a posteromedial to anterolateral direction, advancing toward the tubercle apophysis. Simultaneously, the tubercle apophysis closes in a proximal to distal direction. This converging pattern of physeal closure leaves the anterolateral and distal aspects of the apophysis as the final segments to fuse, explaining the characteristic fracture propagation pathways.
Extensor Mechanism Integration and Vascular Anatomy
The patellar ligament inserts into the apophysis, extending distally with a robust periosteal insertion. The superficial fibers of the patellar tendon insert further distally into the periosteum of the anterior tibial diaphysis, while the deep fibers insert directly into the apophysis. This differential insertion plays a role in the degree of displacement and the integrity of the periosteal sleeve following a fracture.
Vascular anatomy is of critical surgical importance. The anterior tibial recurrent artery, a branch of the anterior tibial artery, courses superiorly through the tibialis anterior muscle to anastomose with the inferior lateral genicular artery. This vessel is highly vulnerable to rupture during a displaced tibial tuberosity fracture. If the artery is torn and retracts into the unyielding fascial confines of the anterolateral compartment, the resulting hemorrhage can rapidly precipitate acute compartment syndrome.
Biomechanical Forces
The pathogenesis of the fracture relies on a massive failure of the extensor mechanism at its weakest link. The injury typically occurs via a forceful quadriceps contraction while the foot is fixed and the knee is in varying degrees of flexion. The significant eccentric force generated by the quadriceps mechanism overcomes the tensile strength of the maturing apophysis and the surrounding periosteum. Alternatively, a sudden, violent passive flexion of the knee against a maximally contracted quadriceps can yield the same catastrophic failure. It is widely hypothesized that adolescents sustaining this injury possess quadriceps muscle strength that disproportionately exceeds the tensile strength of their maturing physeal cartilage.
Indications and Contraindications
Management of tibial tuberosity fractures is dictated by the degree of displacement, the presence of intra-articular extension, and the integrity of the extensor mechanism. The Ogden classification system, a modification of the original Watson-Jones classification, is the standard framework used to guide treatment decisions.
Type I fractures involve the distal portion of the tuberosity. Type II fractures propagate proximally to involve the junction of the apophysis and the proximal tibial epiphysis. Type III fractures extend proximally through the epiphysis and into the knee joint, creating an intra-articular fracture. Type IV fractures involve a fracture through the entire proximal tibial physis, and Type V fractures represent a periosteal sleeve avulsion. Each type is further subdivided into A (non-displaced) and B (displaced).

Non-operative management is strictly reserved for fractures with minimal displacement where the extensor mechanism remains functionally intact. Operative intervention is required to restore the extensor mechanism, anatomically reduce the articular surface, and prevent long-term functional deficits.
| Clinical Scenario | Operative Management | Non Operative Management |
|---|---|---|
| Displacement | > 2 mm displacement of the fracture fragment | < 2 mm displacement |
| Articular Involvement | Type III fractures with articular step-off | Type I or II non-displaced fractures |
| Extensor Mechanism | Inability to perform an active straight leg raise | Intact active straight leg raise |
| Associated Soft Tissue | Compartment syndrome or vascular compromise | Intact neurovascular status |
| Meniscal Pathology | Suspected meniscal entrapment | No mechanical joint blocks |
| Patient Status | Medically optimized for surgical intervention | High surgical risk or active local infection |
Contraindications to immediate internal fixation include active superficial or deep soft tissue infections over the anterior knee, severe medical comorbidities precluding anesthesia, or a non-ambulatory baseline status where extensor mechanism restoration is not functionally required. In cases of acute compartment syndrome, the immediate priority is fasciotomy, with fracture fixation performed concurrently or in a delayed fashion depending on patient stability.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is essential for achieving anatomic reduction and avoiding complications. The native anterolateral position of the tubercle must be accounted for when planning the surgical approach, particularly when intra-articular visualization is required.
Diagnostic Imaging Modalities
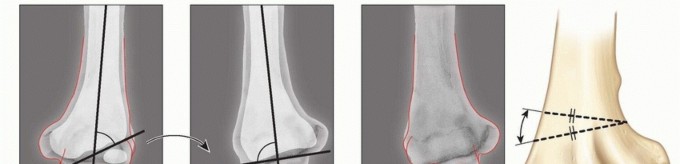
Standard orthogonal radiographs, including anteroposterior and lateral views of the knee, are the primary diagnostic modalities. The lateral radiograph is particularly critical for assessing the degree of superior displacement of the avulsed fragment and evaluating for patella alta, which indicates complete disruption of the extensor mechanism.
For Ogden Type III fractures, a computed tomography scan with three-dimensional reconstructions is highly recommended. CT imaging provides precise mapping of the fracture propagation through the epiphysis, quantifies the degree of articular step-off, and identifies occult comminution that may alter the fixation strategy. Magnetic resonance imaging is generally reserved for cases where there is a high clinical suspicion of associated soft tissue injuries. Literature reports indicate that tibial tuberosity fractures can be accompanied by quadriceps tendon injuries, anterior cruciate ligament tears, and meniscal injuries. The lateral meniscus is particularly prone to avulsion or interposition within the fracture site in Type III patterns.
Patient Positioning and Setup
The patient is positioned supine on a radiolucent operating table to facilitate unhindered fluoroscopic imaging. A small bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, counteracting the natural external rotation of the lower extremity.
A non-sterile tourniquet is applied to the proximal thigh. However, the use of a tourniquet must be carefully considered and potentially avoided if there is any clinical suspicion of evolving compartment syndrome, as tourniquet inflation can exacerbate ischemic injury and obscure the diagnosis. The entire lower extremity is prepped and draped in a standard sterile fashion to allow for full manipulation of the knee joint. A sterile bump or triangle may be placed under the knee to assist with positioning during reduction, though full extension is required to relieve tension on the extensor mechanism during the definitive fixation.
Detailed Surgical Approach and Technique
The surgical objective is anatomic reduction of the articular surface, rigid internal fixation of the apophysis, and meticulous repair of the periosteal sleeve and retinaculum.
Fracture Exposure and Joint Inspection
An anterior longitudinal midline incision or a slightly anterolateral incision is utilized, centered over the tibial tubercle and extending proximally to the inferior pole of the patella. The choice of incision should account for the native anterolateral position of the tubercle. Full-thickness fasciocutaneous flaps are elevated to preserve the tenuous blood supply to the anterior skin.

The deep dissection involves identifying the avulsed tibial tubercle and the attached patellar tendon. The fracture hematoma is meticulously evacuated. It is imperative to identify and protect the medial and lateral retinacular structures, which are often torn longitudinally.
In Ogden Type III fractures, a submeniscal arthrotomy is required to directly visualize the articular surface. The lateral meniscus must be carefully inspected, as its anterior horn can become entrapped within the fracture gap, preventing anatomic reduction. If the meniscus is entrapped, it is gently extracted using a nerve hook or small retractor. Any associated meniscal tears are addressed concurrently with appropriate repair techniques.
Reduction and Internal Fixation
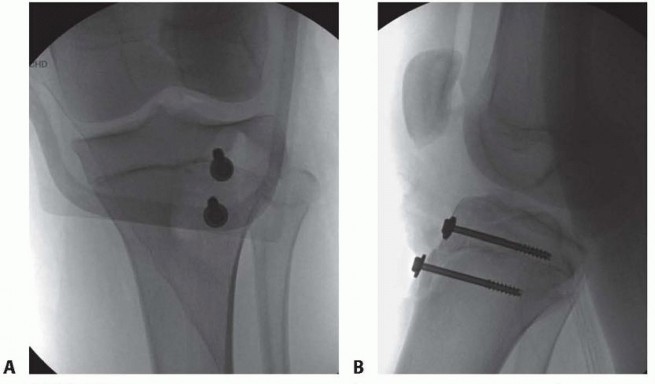
Fracture reduction is achieved by extending the knee fully to eliminate the proximal pull of the quadriceps mechanism. A pointed reduction forceps (Weber clamp) is applied to provisionally hold the fragment in its anatomic bed. Care must be taken to ensure the clamp does not crush the fragile apophyseal bone.
Once provisional reduction is confirmed visually and fluoroscopically, definitive fixation is performed. The standard of care involves the use of 4.0 mm or 4.5 mm cannulated, partially threaded cancellous screws. The trajectory of the screws is critical. Guide wires are advanced from anterior to posterior, and slightly proximal, to engage the dense metaphyseal bone of the posterior tibia.
If the patient has significant remaining growth potential (which is rare, given the typical age of onset), smooth Kirschner wires or fully threaded screws placed parallel to the physis may be considered to minimize the risk of premature physeal arrest. However, in the vast majority of adolescent cases, the physis is nearing imminent closure, and crossing the physis with lag screws is clinically acceptable and provides superior biomechanical stability.
Screws are placed with washers to prevent the screw head from burying into the cartilaginous apophysis. The screws must be lagged to provide interfragmentary compression. Following hardware placement, the knee is ranged through a full arc of motion under direct visualization and fluoroscopy to confirm the stability of the fixation and the absence of intra-articular hardware penetration.
Periosteal and Retinacular Repair
Rigid bony fixation must be supplemented with a robust soft tissue repair. The periosteal sleeve, which is often stripped distally, is repaired back to the tibial diaphysis using heavy non-absorbable or long-lasting absorbable sutures. The medial and lateral retinacular tears are meticulously closed to restore the dynamic stability of the extensor mechanism. This soft tissue repair is paramount for preventing postoperative extensor lag and facilitating early rehabilitation.
Complications and Management
Despite a generally favorable prognosis following anatomic reduction, tibial tuberosity fractures carry a distinct profile of severe complications that demand strict vigilance from the orthopedic surgeon.
Acute Compartment Syndrome
The most devastating acute complication is anterior compartment syndrome of the leg. As previously noted, the anterior tibial recurrent artery is highly susceptible to rupture during the initial displacement of the fracture. Bleeding from its proximal branches, as the vessel retracts into the tightly bound anterolateral compartment, leads to a rapid increase in intracompartmental pressure.
Surgeons must maintain a high index of suspicion. Clinical signs such as pain out of proportion to the injury, pain with passive stretch of the extensor hallucis longus, and a tense, woody compartment require immediate attention. If intracompartmental pressure monitoring confirms the diagnosis, or if clinical suspicion is overwhelmingly high, an emergent four-compartment fasciotomy is mandatory. Delay in recognition leads to irreversible muscle necrosis, ischemic contracture, and severe permanent disability.
Physeal Arrest and Genu Recurvatum
Premature closure of the anterior portion of the proximal tibial physis can lead to a progressive genu recurvatum deformity. Because the posterior physis continues to grow while the anterior aspect is tethered by the fracture or the surgical hardware, the proximal tibia develops an abnormal posterior slope.
While the risk is mitigated by the fact that most patients are near skeletal maturity at the time of injury, younger adolescents (e.g., Ogden Type I or II injuries in 11-year-olds) require close radiographic follow-up. If a recurvatum deformity develops and becomes symptomatic, corrective proximal tibial osteotomy is the salvage procedure of choice.

Hardware Prominence and Bursitis
Due to the sparse subcutaneous tissue overlying the anterior proximal tibia, prominent screw heads and washers frequently cause mechanical irritation and localized bursitis. Patients often report pain when kneeling or during direct impact. This is the most common delayed complication. Management is initially conservative, utilizing knee pads and anti-inflammatory medications. If symptoms persist after complete fracture consolidation (typically 6 to 12 months postoperatively), elective hardware removal is performed.
| Complication | Estimated Incidence | Pathophysiology | Salvage Strategy |
|---|---|---|---|
| Compartment Syndrome | 10% to 20% | Rupture of anterior tibial recurrent artery | Emergent 4-compartment fasciotomy |
| Hardware Prominence | 30% to 50% | Lack of anterior soft tissue coverage | Elective hardware removal after union |
| Genu Recurvatum | < 5% | Premature anterior physeal arrest | Proximal tibial opening wedge osteotomy |
| Loss of Knee Flexion | 5% to 10% | Arthrofibrosis from prolonged immobilization | Aggressive physical therapy, manipulation under anesthesia |
| Nonunion | < 1% | Inadequate fixation or vascular compromise | Revision open reduction internal fixation with bone grafting |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must balance the need for early mobilization to prevent arthrofibrosis with the necessity of protecting the fracture fixation and extensor mechanism repair.
Phase 1 encompasses the first 0 to 4 weeks postoperatively. The patient is placed in a hinged knee brace locked in full extension. Weight-bearing status is typically restricted to toe-touch weight-bearing or non-weight-bearing with crutches to minimize reactive forces through the patellar tendon. Rehabilitation focuses on edema control, patellar mobilization to prevent infrapatellar contracture, and isometric quadriceps sets. Active straight leg raises are generally avoided in the early phase to prevent excessive tensile stress on the repair.
Phase 2 occurs from 4 to 8 weeks. Serial radiographs are obtained to confirm maintenance of reduction and early callus formation. The hinged knee brace is unlocked to allow progressive, controlled range of motion. The goal is to achieve 90 degrees of flexion by week 6 and full flexion by week 8. Weight-bearing is progressively advanced to full as tolerated. Active-assisted and active range of motion exercises are initiated, focusing on closed kinetic chain exercises.
Phase 3, spanning 8 to 12 weeks, focuses on restoring quadriceps strength and muscular endurance. The brace is typically discontinued once the patient demonstrates normalized gait mechanics and sufficient quadriceps control (e.g., ability to perform a controlled single-leg stance). Resistance training is introduced, emphasizing eccentric quadriceps control.
Phase 4, from 3 to 6 months, involves sport-specific training and return-to-play progression. Return to competitive sports is permitted only when radiographic union is complete, the patient has achieved full, painless range of motion, and isokinetic strength testing demonstrates quadriceps and hamstring strength at least 90% of the contralateral, uninjured limb.
Summary of Key Literature and Guidelines
The academic foundation for managing tibial tuberosity fractures is heavily rooted in the anatomical studies and classification systems developed in the late 20th century, augmented by modern systematic reviews focusing on complication profiles.
The Ogden modification of the Watson-Jones classification remains the universally accepted standard for categorizing these injuries and dictating surgical indications. Ogden's seminal work highlighted the complex interplay between the cartilaginous apophysis, the advancing ossification centers, and the mechanical forces of the extensor mechanism.
Subsequent literature has heavily emphasized the critical risk of acute compartment syndrome. Studies by Frey et al. and Pesl et al. established the anatomical basis for this complication, identifying the anterior tibial recurrent artery as the primary culprit. Their work mandates that orthopedic surgeons maintain a high clinical suspicion for compartment syndrome in any displaced tibial tuberosity fracture, regardless of the apparent energy of the injury mechanism.
Recent systematic reviews by Pretell-Mazzini et al. have aggregated outcome data, confirming that while the complication profile is severe, the long-term functional outcomes following anatomic surgical reduction and rigid internal fixation are excellent. The literature consistently demonstrates that restoring the articular congruity in Type III fractures and repairing the periosteal sleeve in all displaced variants are the most critical technical steps for ensuring a return to pre-injury athletic function. Future research is directed toward optimizing postoperative rehabilitation timelines and identifying biomechanical risk factors in adolescent athletes to prevent the occurrence of these catastrophic apophyseal failures.
Clinical & Radiographic Imaging
You Might Also Like