Congenital Angular Deformities & Pseudarthrosis of the Tibia

Key Takeaway
Congenital pseudarthrosis of the tibia and fibula presents a formidable challenge in pediatric orthopedics, often associated with neurofibromatosis type 1. Management requires a deep understanding of the Boyd classification, meticulous excision of hamartomatous tissue, and robust stabilization. This guide details the pathophysiology, clinical evaluation, and step-by-step surgical interventions—including the Langenskiöld tibiofibular synostosis and intramedullary rodding—to achieve osseous union and prevent progressive ankle valgus in the growing child.
CONGENITAL ANGULAR DEFORMITIES OF THE LEG
Congenital angular deformities of the leg represent a complex spectrum of pediatric orthopedic conditions that demand precise biomechanical understanding and meticulous longitudinal management. These deformities are primarily categorized into two distinct clinical entities based on the apex of the angulation: anterior bowing and posterior bowing.
In both presentations, the tibia is rarely deformed in a single plane; the sagittal bowing is frequently accompanied by coronal plane deformities, manifesting as either medial or lateral deviation. Recognizing this multiplanar complexity, Badgley, O’Connor, and Kudner introduced the comprehensive term congenital kyphoscoliotic tibia to describe these three-dimensional deformities.
Crucially, the direction of the bowing dictates the clinical prognosis and underlying pathology. Anterior bowing of the tibia is pathognomonically associated with neurofibromatosis type 1 (NF1) and carries a high risk of progressing to congenital pseudarthrosis. Conversely, posteromedial bowing is typically a benign, self-limiting condition, though it is frequently associated with significant leg-length discrepancy, clinodactyly, and anomalous maturation of the carpal and metacarpal bones.
Fig. 26-52 Congenital posteromedial bowing of left tibia. A, Anteroposterior view. B, Lateral view.
Clinical Pearl: Always differentiate anterior from posterior bowing at birth. Anterior bowing requires immediate protective bracing (KAFO) to prevent fracture and subsequent pseudarthrosis, whereas posteromedial bowing requires observation and future management of the inevitable leg-length discrepancy.
CONGENITAL PSEUDARTHROSIS OF THE FIBULA AND TIBIA
Congenital pseudarthrosis is a specific, recalcitrant type of nonunion that is either present at birth or incipient (developing shortly after birth following a minor fracture). The exact etiology remains elusive; however, its profound association with neurofibromatosis or related stigmata strongly suggests a shared genetic or mesodermal dysplasia pathway. The condition most commonly afflicts the distal half of the tibia and frequently involves the ipsilateral fibula.
Congenital Pseudarthrosis of the Fibula
Congenital pseudarthrosis of the fibula is a critical clinical entity that often precedes or accompanies the same condition in the ipsilateral tibia. The natural history of isolated fibular pseudarthrosis is highly variable, presenting in several grades of severity:
* Bowing of the fibula without frank pseudarthrosis.
* Fibular pseudarthrosis without ankle deformity.
* Fibular pseudarthrosis with progressive ankle deformity.
* Fibular pseudarthrosis with latent (incipient) pseudarthrosis of the tibia.
Biomechanics of the Ankle Deformity:
The fibula acts as a vital lateral tether for the ankle mortise. When a pseudarthrosis occurs, the lateral malleolus loses its proximal structural support and migrates proximally with growth. This proximal migration results in a progressive, often severe, valgus deformity of the ankle. This phenomenon can even develop latently between the time of a successful tibial bone grafting procedure and skeletal maturity.
Management Strategies:
Until skeletal maturity is reached, the ankle must be stabilized using a rigid ankle-foot orthosis (AFO). If the patient reaches skeletal maturity with a significant valgus deformity, a supramalleolar osteotomy through essentially normal metaphyseal bone is indicated, and high rates of osseous union can be expected.
However, to prevent this valgus deformity or halt its progression during the critical growth years, Langenskiöld devised a highly effective prophylactic operation. The procedure creates a robust synostosis between the distal tibial and fibular metaphyses. Because securing union via bone grafting in an isolated fibular pseudarthrosis is notoriously difficult, bypassing the pseudarthrosis to stabilize the lateral malleolus directly to the tibia is the preferred biomechanical solution.
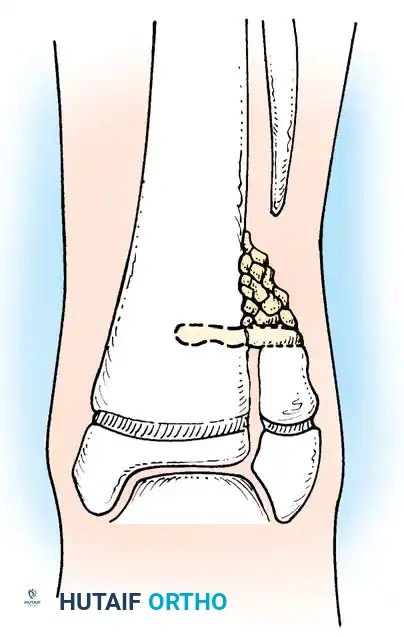
Fig. 26-53 Langenskiöld technique for creating synostosis between distal tibial and fibular metaphyses to prevent valgus deformity of ankle in congenital pseudarthrosis of fibula.
SURGICAL TECHNIQUE: Tibiofibular Synostosis (Langenskiöld)
Indications: Progressive ankle valgus in a growing child with congenital pseudarthrosis of the fibula.
Positioning: Supine with a bump under the ipsilateral hip to internally rotate the leg, bringing the lateral malleolus into clear view. A thigh tourniquet is applied.
- Surgical Approach: Make a longitudinal incision anteriorly over the distal fibula, carefully avoiding the superficial peroneal nerve.
- Fibular Resection: Divide the fibula 1 to 2 cm proximal to the level of the distal tibial physis. Excise the cone-shaped, dysplastic part of the distal fibular shaft to expose healthy bone.
- Tibial Preparation: On the lateral surface of the tibia, exactly at the level of the cut surface of the fibula and at the attachment of the interosseous membrane, create a cortical window (hole) as wide as the diameter of the fibula.
- Periosteal Stripping: Proximal to this hole, meticulously elevate and remove the periosteum and interosseous membrane from the tibia over an area of several square centimeters to provide a vascularized bed for the graft.
- Graft Harvest: From the ipsilateral iliac crest, harvest a structural corticocancellous bone graft. The graft must be the same width as the tibial hole and long enough to span from the lateral surface of the fibula deep into the spongy cancellous bone of the tibial metaphysis.
- Graft Insertion: Insert the structural graft perpendicular to the long axis of the limb. Ensure it rests securely on the cut surface of the fibula and extends deeply into the slot created in the tibial cortex.
- Cancellous Packing: Pack additional spongy autogenous iliac bone tightly into the angle between the proximal surface of the structural graft and the lateral surface of the tibia to maximize osteogenesis.
- Closure and Immobilization: Close the wound in layers. Apply a well-padded, long-leg cast from below the knee to the base of the toes, ensuring the ankle is held in a neutral position.
Postoperative Protocol:
* 0-8 Weeks: Strict non-weight bearing in the cast.
* 2 Months: Transition to full weight bearing in a walking cast or rigid AFO, provided radiographic evidence of early incorporation is present.
* 4 Months: The cast is discontinued, but protective bracing (AFO) is often maintained to protect the synostosis during high-impact activities.
CONGENITAL PSEUDARTHROSIS OF THE TIBIA (CPT)
Congenital pseudarthrosis of the tibia is an exceptionally rare and challenging condition, with an incidence of approximately 1 in 250,000 live births. It is characterized by segmental osseous dysplasia leading to anterolateral bowing and subsequent nonunion.
The association with neurofibromatosis is profound. Most large academic series report a 50% to 90% association with the stigmata of NF1 (e.g., café-au-lait spots, cutaneous neurofibromas, Lisch nodules). A definitive multicenter study from the European Paediatric Orthopaedic Society (EPOS) confirmed that 186 (55%) of 340 patients with CPT had clinical symptoms of neurofibromatosis.
Boyd Classification of Congenital Pseudarthrosis of the Tibia
Harold Boyd classified CPT into six distinct types based on radiographic appearance and natural history. This classification remains the gold standard for guiding prognosis and surgical decision-making.
Type I: Pseudarthrosis occurs with anterior bowing and a frank osseous defect in the tibia present at birth. Other congenital deformities may coexist, complicating management.
Type II (The "High-Risk" Tibia): Occurs with anterior bowing and an hourglass constriction of the tibia present at birth. The tibia is tapered, rounded, and highly sclerotic, with complete obliteration of the medullary canal. Spontaneous fracture, or fracture following trivial trauma, typically occurs before 2 years of age. This is the most common type, is heavily associated with NF1, and carries the poorest prognosis. Recurrence of fracture is frequent during the growth period but generally ceases after skeletal maturation.
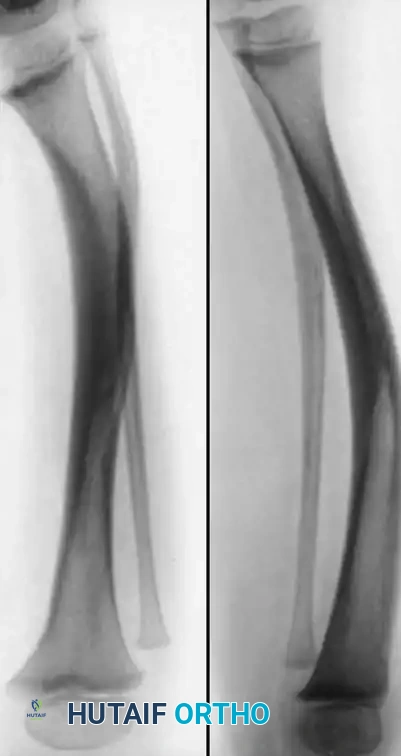
Fig. 26-54 Type II congenital pseudarthrosis of tibia. Note anterior bowing and narrow, sclerotic medullary canal.
Type III: Develops within a congenital cyst, usually located near the junction of the middle and distal thirds of the tibia. Anterior bowing may precede or follow the fracture. The prognosis is significantly better than Type II; excellent long-term results well into adulthood have been reported following a single surgical intervention.
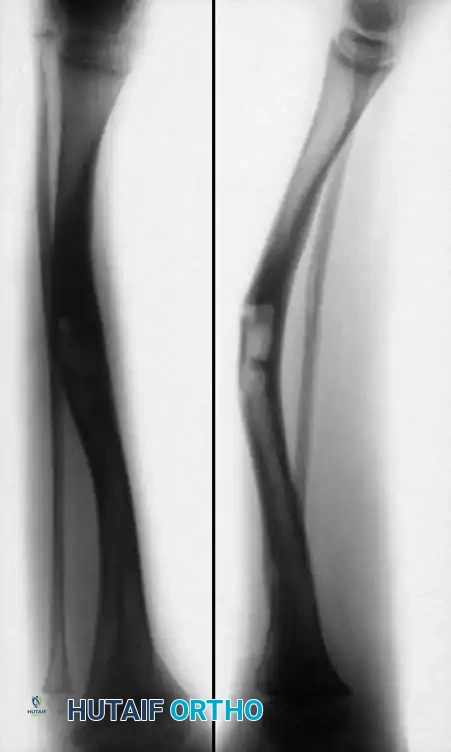
Fig. 26-55 Type III congenital pseudarthrosis of tibia. Note cyst formation in middle third of tibia with anterior bowing.
Type IV: Originates in a sclerotic segment of bone without narrowing or hourglass constriction. The medullary canal is partially or completely obliterated. An "insufficiency" or "stress" fracture develops in the anterior cortex and gradually propagates through the sclerotic bone. If untreated, the fracture widens into a frank pseudarthrosis. Prognosis is excellent if surgically addressed before the insufficiency fracture completes.

Fig. 26-56 Type IV congenital pseudarthrosis of tibia. Note fracture in anterior cortex in distal third of tibia.
Type V: Occurs in the presence of a dysplastic fibula. A pseudarthrosis of the fibula, tibia, or both may develop. If confined to the fibula, the prognosis is good. If it progresses to tibial pseudarthrosis, the clinical course mirrors that of a Type II lesion.
Type VI: An extremely rare presentation occurring as an intraosseous neurofibroma or schwannoma that directly results in pseudarthrosis. Prognosis depends entirely on the biological aggressiveness of the intraosseous lesion and the adequacy of its resection.
Principles of Management
The treatment of CPT is dictated by the patient's age, the Boyd classification, and the presence of a frank fracture.
Conservative Management (The Pre-Pseudarthrotic Stage):
A true, established congenital pseudarthrosis of the tibia will never heal with casting alone. However, Grill et al. (EPOS) demonstrated that conservative treatment plays a vital role in the pre-fracture stage. The application of a stable, custom-molded knee-ankle-foot orthosis (KAFO) with an anterior rigid shield can significantly delay the onset of fracture. Delaying the fracture allows the child to reach an older age (preferably >3 years) before undergoing surgery, which statistically correlates with higher rates of osseous union.
Surgical Intervention vs. Amputation:
Once a fracture occurs, surgical intervention is mandatory. Historically, obtaining osseous union in CPT has been one of the most formidable challenges in orthopedic surgery. Boyd and Sage reported primary union in only 56% of patients. Morrissy et al. reported union in less than 50%, and Murray and Lovell reported a dismal 31% success rate.
Because of these historical difficulties, the decision between attempting limb salvage (bone grafting/fixation) and primary amputation must be weighed carefully.
Factors favoring amputation (Symes or Boyd amputation) include:
* Anticipated leg-length discrepancy exceeding 5 to 7.5 cm (2 to 3 inches).
* A history of multiple failed surgical procedures (average of 4.7 procedures in amputated limbs per Traub et al.).
* Severe stiffness and dysfunction of the foot and ankle.
* Severe Type II lesions in very young infants where multiple surgeries would cause severe psychological and physical morbidity.
Surgical Warning: Lehman et al. strongly advocate for early primary amputation with appropriate prosthetic fitting in severe cases, emphasizing that the final evaluation of success should be based on the functional level of the child, not merely the radiographic achievement of bone union.
Advanced Surgical Strategies for Limb Salvage
For patients deemed appropriate for limb salvage, modern surgical techniques have significantly improved union rates.
1. Excision of the Hamartoma (The McElvenny Principle):
McElvenny first identified that the pseudarthrosis site is enveloped by a thick, fibrous cuff of hamartomatous tissue. This tissue is biologically inert, highly constrictive, and actively inhibits osteogenesis. Absolute, radical excision of this fibrous hamartoma back to healthy, bleeding bone is the most critical step of any CPT operation. Failure to resect this tissue guarantees recurrence.
2. Intramedullary Rodding and Bone Grafting:
The current gold standard for mechanical stabilization is intramedullary (IM) rodding, as popularized by Anderson, Schoenecker, Sheridan, and Rich. The IM rod must span the entire length of the tibia, often crossing the ankle joint into the talus or calcaneus in very distal lesions to ensure absolute rigidity.

Clinical example demonstrating intramedullary stabilization of a tibial pseudarthrosis. Note the central placement of the rod spanning the dysplastic segment.
The IM rod is combined with massive autogenous iliac crest bone grafting. The graft provides the essential osteoinductive and osteoconductive properties lacking in the dysplastic tibial segment.

Radiographic follow-up showing incorporation of bone graft and maintenance of alignment following intramedullary fixation.
3. Osteostimulators:
Baker, Cain, and Tullos reported enhanced union rates when intramedullary fixation and bone grafting were augmented with an implantable osteostimulator (direct current electrical stimulation), as originally described by Paterson and Simonis.
Postoperative Care and Refracture Management:
Even when union is achieved, the tibia remains biologically abnormal. The medullary canal often remains narrow, and the cortex lacks normal remodeling capabilities. Refracture is a constant threat until skeletal maturity.

Long-term follow-up imaging demonstrating the persistent risk of refracture or hardware migration in the biologically compromised tibia, necessitating prolonged orthotic protection.
Therefore, once union is obtained, the limb must be protected in a patellar tendon-bearing (PTB) brace or AFO until the child reaches skeletal maturity. Parents must be extensively counseled that limb salvage is a childhood-long commitment, often requiring secondary procedures for hardware exchange, management of leg-length discrepancies (via epiphysiodesis or lengthening), and correction of residual angular deformities.
You Might Also Like


