Congenital Elevation of the Scapula: Comprehensive Management of Sprengel Deformity

Key Takeaway
Sprengel deformity, or congenital elevation of the scapula, is a complex anomaly characterized by a hypoplastic, superiorly displaced scapula. Often associated with Klippel-Feil syndrome and an omovertebral connection, it restricts shoulder abduction and alters cervicothoracic biomechanics. Surgical intervention, ideally performed around three years of age, aims to release tethering structures, excise the omovertebral bone, and relocate the scapula inferiorly to restore function and cosmesis while mitigating brachial plexus injury risks.
Congenital Anomalies of the Trunk and Upper Extremity
Congenital anomalies of the shoulder girdle present unique biomechanical and reconstructive challenges to the orthopedic surgeon. Among these, congenital elevation of the scapula, universally recognized as Sprengel deformity, represents the most common congenital defect of the shoulder. Successful management requires a profound understanding of embryological failure, altered periscapular anatomy, and the intricate balance required to restore function without compromising the brachial plexus.
Sprengel Deformity: Pathoanatomy and Biomechanics
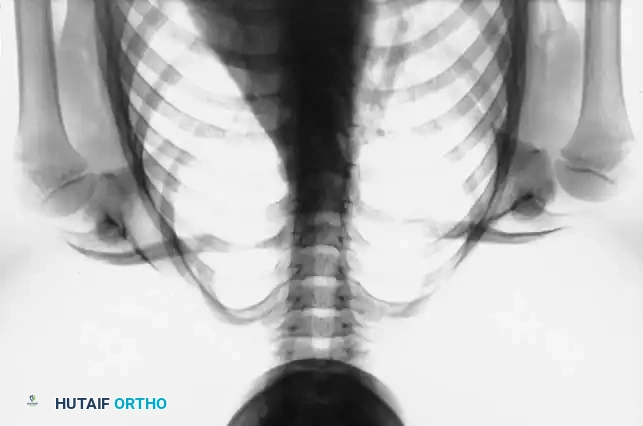
In Sprengel deformity, the scapula fails to descend during the 9th to 12th weeks of gestation, remaining abnormally elevated in relation to the thoracic cage. The affected scapula is not merely malpositioned; it is fundamentally dysplastic. It is typically hypoplastic, misshapen, and exhibits a characteristic decrease in the height-to-width ratio, making it appear broader and shorter than a normal scapula.
The Omovertebral Connection
A defining pathoanatomical feature, present in approximately one-third of patients, is the omovertebral connection. This structure tethers the superior angle or superomedial border of the scapula to the cervical spine (typically the spinous process, lamina, or transverse process of the lower cervical vertebrae).
Clinical Pearl: The omovertebral connection is not always osseous. It may present as a rhomboidal plaque of cartilage, a dense fibrous band within a strong fascial sheath, or a well-developed diarthrodial joint. Regardless of its histologic composition, it acts as an unyielding tether that restricts scapular rotation and limits glenohumeral abduction.
Morphometric Analysis and Biomechanics
Advanced three-dimensional computed tomography (3D CT) has revolutionized our understanding of scapular morphology in Sprengel deformity. Morphometric analyses, such as those conducted by Cho et al., demonstrate that the affected scapulae are often larger in overall volume than the contralateral normal scapulae, despite their hypoplastic appearance.
Cho et al. identified an inverse relationship between scapular rotation and superior displacement. The specific point of tethering by the omovertebral connection dictates the ultimate shape, rotational malalignment, and degree of superior displacement of the scapula. Interestingly, glenoid version typically remains unaffected, meaning the primary limitation in shoulder abduction stems from the inability of the scapula to rotate on the thoracic wall, rather than intrinsic glenohumeral dysplasia.
Associated Syndromes
Sprengel deformity rarely exists in isolation. The embryological insult that arrests scapular descent often affects adjacent mesodermal structures. Surgeons must maintain a high index of suspicion for:
* Klippel-Feil Syndrome: Congenital fusion of cervical vertebrae.
* Costal Anomalies: Cervical ribs, fused ribs, or absent ribs.
* Muscular Hypoplasia: Partial or complete absence of periscapular musculature (e.g., trapezius, rhomboids, serratus anterior).
* Congenital Scoliosis: Often driven by unilateral unsegmented bars or hemivertebrae.
Clinical and Radiographic Evaluation
Clinical impairment correlates directly with the severity of the deformity. In mild cases, the scapula is only slightly elevated, and shoulder motion is minimally restricted. In severe manifestations, the hypoplastic scapula may be elevated so profoundly that its superior angle nearly abuts the occiput.
Patients frequently present with torticollis or a noticeable deviation of the head toward the affected side, driven by the tethering effect of the omovertebral bone or concurrent cervical spine anomalies. The cosmetic asymmetry is often the primary concern of the parents, presenting as a prominent lump at the base of the neck and apparent shortening of the neck.
Radiographic evaluation must include standard anteroposterior and lateral views of the cervical and thoracic spine, as well as bilateral shoulder radiographs.
Surgical Warning: Standard radiographs often underestimate the complexity of the deformity. Three-dimensional CT reconstruction is highly recommended for preoperative planning. It precisely delineates the omovertebral connection, maps the altered scapular morphology, and identifies concurrent cervical spine anomalies that may complicate intubation or surgical positioning.
Indications and Timing of Surgery
The decision to operate is dictated by the severity of functional impairment and cosmetic deformity.
* Mild Deformity: No surgical intervention is indicated. Physical therapy may be utilized to maximize compensatory motion, though it will not alter the anatomical tether.
* Moderate to Severe Deformity: Surgical reconstruction is indicated to improve shoulder abduction and restore cosmetic symmetry.
Optimal Timing: The consensus for surgical intervention is approximately 3 to 8 years of age. Operating before age 3 is technically challenging due to the small size of the structures and the difficulty in achieving robust soft-tissue repairs. However, delaying surgery beyond 8 years of age significantly increases the risk of brachial plexus palsy. As the child grows, the neurovascular bundle adapts to the shortened, elevated position; aggressive caudad translation of the scapula in an older child places profound traction on the brachial plexus against the first rib and clavicle.
Evolution of Surgical Techniques
The surgical correction of Sprengel deformity is never a simple inferior translation of the bone; it requires comprehensive release of soft-tissue contractures, excision of tethering structures, and dynamic muscle transfers.
The Green Procedure and Modifications
Green originally described an extensive extraperiosteal release of the periscapular muscles, excision of the supraspinous portion of the scapula and omovertebral bone, followed by inferior translation and reattachment of the musculature.
* Leibovic, Ehrlich, and Zaleske Modification: Enhanced the Green procedure by suturing the inferior pole of the relocated scapula into a surgically created pocket within the latissimus dorsi, providing a dynamic inferior tether.
* Bellemans and Lamoureux Modification: Avoided dissection of the serratus anterior to preserve scapular protraction and allow for immediate postoperative mobilization, reporting an average abduction gain of 77 degrees.
The Woodward Procedure
Described by Woodward, this technique involves the en masse transfer of the origins of the trapezius and rhomboid muscles to a more inferior position on the spinous processes.
Greitemann, Rondhuis, and Karbowski strongly advocate for the Woodward procedure over the Green procedure for several reasons:
1. Incision Placement: The muscles are incised at their spinal origins rather than at their scapular insertions. This moves the healing interface away from the scapula, significantly lowering the risk of keloid or dense scar formation that could re-tether the scapula in a poor position.
2. Mobilization: It allows for a larger, more uniform mobilization of the entire shoulder girdle.
3. Cosmesis: The midline postoperative scar is generally thinner and more cosmetically acceptable than the periscapular scar of the Green procedure.
Borges et al. further modified the Woodward procedure by routinely excising the prominent superomedial border of the scapula, reporting an average improvement in shoulder abduction of 35 degrees with high patient satisfaction.
The Mears Procedure
Mears identified that contracture of the long head of the triceps acts as a significant antagonist to full abduction in Sprengel deformity. His procedure combines partial scapular resection, omovertebral excision, and the critical addition of releasing the long head of the triceps from the infraglenoid tubercle. This specific release has yielded dramatic improvements, with average flexion increasing from 100 to 175 degrees.
Preoperative Prophylaxis: Morcellization of the Clavicle
The most devastating complication of Sprengel deformity surgery is brachial plexus palsy, caused by traction and compression of the plexus between the clavicle and the first rib as the scapula is pulled inferiorly.
To mitigate this, prophylactic shortening of the clavicle is recommended in severe deformities or in older children. While some surgeons perform a discrete osteotomy, morcellization of the clavicle is highly effective. It functionally shortens the anterior strut of the shoulder girdle, decompressing the thoracic outlet, while the preserved periosteal sleeve ensures rapid reconstitution of the bone.
TECHNIQUE: Morcellization of the Clavicle
Note: This procedure is performed with the patient in the supine position prior to flipping prone for the scapuloplasty.
- Incision and Exposure: Make a straight transverse incision directly over the clavicle, extending from 1.5 cm lateral to the sternoclavicular joint to 1.5 cm medial to the acromioclavicular joint.
- Subperiosteal Dissection: Incise the periosteum longitudinally. Using a periosteal elevator, carefully expose the middle third of the clavicle subperiosteally. Meticulous dissection is required inferiorly to protect the subclavian vessels and brachial plexus.
- Osteotomy and Morcellization: Divide the clavicular diaphysis approximately 2 cm from each articular end. Remove the intervening diaphyseal segment to the back table and use a rongeur or bone mill to cut it into small, corticocancellous pieces (morcellization).
- Reconstitution: Pack the morcellized bone fragments back into the empty periosteal tube.
- Closure: Close the periosteal sleeve securely with interrupted absorbable sutures to contain the graft and guide regeneration. Close the subcutaneous tissues and skin in a standard layered fashion.
TECHNIQUE: The Woodward Operation for Sprengel Deformity
We generally prefer the Woodward procedure due to its superior functional outcomes and lower risk of periscapular scarring.
Positioning and Preparation
- Following clavicle morcellization (if indicated), carefully log-roll the patient into the prone position.
- Pad all bony prominences. Ensure the abdomen is free to allow adequate ventilation.
- Prepare and drape both shoulders and the entire back. It is critical that the involved shoulder girdle and arm can be freely manipulated, and the uninvolved, normal scapula can be visualized to serve as an anatomical reference for final positioning.
Surgical Approach and Muscle Release
- Incision: Make a precise midline longitudinal incision extending from the spinous process of the first cervical vertebra (C1) distally to the spinous process of the ninth thoracic vertebra (T9).
- Flap Elevation: Undermine the skin and subcutaneous tissues laterally, creating a thick fasciocutaneous flap until the entire medial border of the affected scapula is exposed.
- Trapezius Identification: Identify the lateral border of the trapezius at the distal extent of the incision. Using blunt dissection, separate the trapezius from the underlying latissimus dorsi muscle.
- Spinal Detachment: By sharp dissection, carefully free the fascial sheath and aponeurotic origin of the trapezius from the spinous processes.
- Rhomboid Detachment: Deep to the trapezius, identify the origins of the rhomboideus major and minor muscles. Sharply detach them from the spinous processes.
- Anterior Mobilization: Free the rhomboids and the superior portion of the trapezius from the underlying chest wall musculature (serratus posterior superior and erector spinae).
Excision of Tethering Structures
- Exposure of the Tether: Retract the freed, continuous sheet of the trapezius and rhomboids laterally. This exposes the deep pathoanatomy: the omovertebral bone, fibrous bands, and the contracted levator scapulae attached to the superior angle of the scapula.
- Extraperiosteal Resection: By meticulous extraperiosteal dissection, completely excise the omovertebral bone. If no bone is present, excise the dense fibrous bands and the contracted levator scapulae.
> Surgical Warning: Dissection at the superior angle of the scapula is perilous. You must stay strictly extraperiosteal on the omovertebral bone to avoid devastating injury to the spinal accessory nerve (CN XI), the dorsal scapular nerve (supplying the rhomboids), and the transverse cervical artery. - Scapular Resection: If the supraspinous portion of the scapula is severely deformed or curves anteriorly over the thorax, resect it along with its periosteum. Leaving the periosteum behind will result in rapid bone regrowth and recurrent deformity. This resection further releases the levator scapulae insertion, allowing the shoulder girdle to mobilize freely.
- Superior Release: Divide transversely the remaining narrow, superior-most attachment of the trapezius at the level of the fourth cervical vertebra (C4).
Relocation and Fixation
- Caudad Translation: Grasp the scapula and the attached sheet of muscles and displace them distally (inferiorly).
> Clinical Pearl: Do not attempt to align the inferior angles of the scapulae. Because the Sprengel scapula is hypoplastic and shorter, aligning the inferior angles will result in the glenoid being positioned too low. Instead, translate the scapula until its spine lies at the exact same horizontal level as the spine of the contralateral, normal scapula. - Reattachment: While an assistant holds the scapula firmly in this corrected, inferior position, reattach the aponeuroses of the trapezius and rhomboids to the spinous processes at their new, more inferior level using heavy, non-absorbable sutures.
- Distal Redundancy Management: The inferior translation will create a redundant fold in the origin of the trapezius at the distal end of the incision. Either excise this excess tissue or incise the fold, overlap the free edges (pants-over-vest repair), and suture them securely in place to reinforce the repair.
- Closure: Place a subfascial drain if necessary. Close the subcutaneous tissues and skin meticulously to minimize midline scarring.
Postoperative Protocol and Rehabilitation
Rigorous postoperative care is essential to maintain the surgical correction and maximize functional gains.
- Immobilization: Immediately postoperatively, the affected upper extremity is placed in a Velpeau bandage or a customized shoulder immobilizer. This removes the weight of the arm from the fresh muscle repairs and prevents early superior migration of the scapula. Immobilization is typically maintained for 2 to 3 weeks.
- Neurological Monitoring: Serial neurovascular examinations must be performed in the immediate postoperative period to rule out delayed brachial plexus palsy. If signs of plexus compromise develop, immediate removal of all restrictive dressings is required, and if symptoms persist, surgical exploration to release the tethering or remove the clavicular strut may be necessary.
- Rehabilitation: At 2 to 3 weeks, the immobilizer is discontinued. A structured physical therapy program is initiated, focusing on active and active-assisted range-of-motion exercises. Emphasis is placed on restoring glenohumeral abduction, scapulothoracic rhythm, and strengthening the newly transferred periscapular musculature.
Long-term follow-up indicates that while the scapula will never be perfectly normal anatomically, the Woodward procedure reliably provides significant improvements in neck contour, shoulder symmetry, and functional abduction, greatly enhancing the patient's quality of life.
📚 Medical References
- Sprengel deformity by a modifi ed Green’s procedure, J Pediatr Orthop 8:194, 1999.
- Borges JLP, Shah A, Tores BC, et al: Modifi ed Woodward procedure for Sprengel deformity of the shoulder: long-term results, J Pediatr Orthop 16:508, 1996.
- Cho TJ, Choi IH, Chung CY, et al: The Sprengel deformity: morphometric analysis using 3D-CT and its clinical relevance, J Bone Joint Surg 82B:7121, 2000.
- Chung SMK, Farahvar H: Surgery of the clavicle in Sprengel’s deformity, Clin Orthop Relat Res 116:138, 1976.
- Chung SMK, Nissenbaum MM: Congenital and developmental defects of the shoulder, Orthop Clin North Am 6:381, 1975.
- Galpin RD, Birch JG: Congenital elevation of the scapula (Sprengel’s deformity), Orthopedics 10:965, 1987.
- Green WT: The surgical correction of congenital elevation of the scapula (Sprengel’s deformity), J Bone Joint Surg 39A:1439, 1957.
- Green WT: Sprengel’s deformity: congenital elevation of the scapula, Instr Course Lect 21:55, 1972.
- Greitemann B, Rondhuis JJ, Karbowski A: Treatment of congenital elevation of the scapula: 10(1-18) year follow-up of 37 cases of Sprengel’s deformity, Acta Orthop Scand 64:365, 1993.
- Halley DK, Eyring EJ: Congenital elevation of the scapula in a family, Clin Orthop Relat Res 97:31, 1973.
- Leibovic SJ, Ehrlich MG, Zaleske DJ: Sprengel deformity, J Bone Joint Surg 72A:192, 1990.
- McMurty I, Bennet GC, Bradish C: Osteotomy for congenital elevation of the scapula (Sprengel’s deformity), J Bone Joint Surg 87B:986, 2005.
- Mears DC: Partial resection of the scapula and a release of the long head of the triceps for the management of Sprengel’s deformity, J Pediatr Orthop 21:242, 2001.
- Orrell KG, Bell DF: Structural abnormality of the clavicle associated with Sprengel’s deformity: a case report, Clin Orthop Relat Res 258:157, 1990.
- Robinson RA, Braun RM, Mack P, et al: The surgical importance of the clavicular component of Sprengel’s deformity, J Bone Joint Surg 49A:481, 1967 (abstract). Woodward JW: Congenital elevation of the scapula: correction by release and transplantation of muscle origins: a preliminary report, J Bone Joint Surg 43A:219, 1961.
- Zhang AM, Zhang J, Lu ML, et al: Partial scapulectomy for congenital elevation of the scapula, Clin Orthop Relat Res 457:171, 2007.
You Might Also Like


