Unlock better outcomes: Pediatric hip fractures & lateral femoral cortex
Key Takeaway
This article provides essential research regarding Unlock better outcomes: Pediatric hip fractures & lateral femoral cortex. The femoral neck forms an angle of about 135 degrees with the femoral shaft. While the medial two-thirds of the femoral neck is intracapsular, the lateral third is not. This extra-articular portion of the **lateral femoral cortex** and neck region is crucial for classifying pediatric hip fractures, differentiating between intracapsular and extracapsular injuries that have distinct prognoses and treatment approaches.
Introduction and Epidemiology of Pediatric Hip Fractures
Pediatric hip fractures are rare but highly consequential injuries, representing less than 1% of all pediatric fractures. Unlike hip fractures in the elderly, which typically result from low-energy falls through osteoporotic bone, pediatric proximal femur fractures generally necessitate high-energy trauma. Mechanisms often include motor vehicle collisions, auto-versus-pedestrian accidents, or falls from significant heights. In infants and non-ambulatory toddlers, a high index of suspicion for non-accidental trauma must be maintained when a proximal femur fracture is identified.
The Delbet classification remains the standard for categorizing these injuries based on anatomic location, which directly correlates with the risk of avascular necrosis (AVN) and dictates the surgical approach. Type I fractures are transepiphyseal separations, often associated with dislocation of the capital femoral epiphysis. Type II fractures are transcervical and represent the most common pattern. Type III fractures are cervicotrochanteric, occurring at the base of the femoral neck. Type IV fractures are intertrochanteric.


Because the pediatric proximal femur possesses a thick, robust periosteum and dense trabecular bone, significant force is required to cause structural failure. Consequently, these patients frequently present with concomitant life-threatening injuries, including traumatic brain injury, visceral trauma, and other axial or appendicular fractures. Initial evaluation must strictly adhere to Advanced Trauma Life Support (ATLS) protocols. The natural history of untreated or inadequately stabilized pediatric hip fractures is uniformly poor, characterized by a high incidence of AVN, coxa vara, nonunion, and premature physeal closure.



Surgical Anatomy and Biomechanics of the Proximal Femur
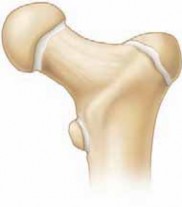
A profound understanding of the pediatric proximal femoral anatomy is critical for successful surgical intervention. The proximal femur develops from a single cartilaginous anlage. By the age of four, the capital femoral epiphysis and the greater trochanteric apophysis separate and develop their own distinct physes. The femoral neck forms an angle of approximately 135 degrees with the femoral shaft. The medial two-thirds of the femoral neck is intracapsular, while the lateral third is extracapsular.


The vascular supply to the capital femoral epiphysis is precarious and changes dynamically throughout skeletal maturation. At birth, the metaphyseal vessels cross the physis to supply the epiphysis. However, as the physis matures, it acts as a barrier, and the blood supply becomes entirely dependent on the extracapsular arterial ring formed by the medial and lateral femoral circumflex arteries. The lateral epiphyseal vessels, branches of the medial femoral circumflex artery, course along the posterosuperior aspect of the femoral neck within the retinaculum. Because the intra-articular femoral neck lacks a true cambium layer of periosteum, it has minimal capacity for primary callus formation, relying heavily on endosteal healing and absolute mechanical stability.


The lateral femoral cortex plays a paramount biomechanical role in pediatric hip fracture fixation. It serves as the critical buttress against varus collapse and provides the necessary cortical purchase for implants. In pediatric patients, the lateral cortex is highly stressed during weight-bearing. Iatrogenic damage to this structure—such as multiple drill passes, poorly positioned starting holes, or inadequate implant spacing—creates severe stress risers. This can lead to catastrophic subtrochanteric fractures. The insertion of the hip abductors on the greater trochanter and the iliopsoas on the lesser trochanter create deforming forces that must be neutralized by rigid internal fixation bridging the lateral cortex to the medial calcar.


Indications and Contraindications for Surgical Intervention
The management of pediatric hip fractures is overwhelmingly operative. Non-operative management is historically associated with unacceptable rates of varus collapse, nonunion, and malunion, even in minimally displaced fractures. The goal of surgery is anatomic reduction, stable internal fixation, and decompression of the intracapsular hematoma to mitigate the risk of AVN.


| Fracture Type / Scenario | Operative Indications | Non-Operative Indications | Contraindications to Surgery |
|---|---|---|---|
| Delbet Type I | Almost always indicated. Requires urgent reduction and stabilization. | None. | Medically unstable patient (damage control orthopedics applies). |
| Delbet Type II | Displaced or non-displaced. High risk of displacement if treated conservatively. | Extremely rare; only if patient cannot tolerate anesthesia. | Active local infection; severe hemodynamic instability. |
| Delbet Type III | Displaced or non-displaced. Requires robust fixation utilizing the lateral cortex. | None. | Inadequate soft tissue envelope (relative). |
| Delbet Type IV | Displaced fractures, or non-displaced fractures in older children/adolescents. | Truly non-displaced fractures in infants or toddlers (spica cast). | Polytrauma precluding definitive fixation (use external fixation temporarily). |
| Pathologic Fractures | Pending structural failure or completed fracture (e.g., unicameral bone cyst). | Small, asymptomatic lesions without impending fracture risk. | Untreated primary malignancy requiring neoadjuvant therapy first. |


Preoperative Planning and Patient Positioning
Thorough preoperative planning is mandatory. Standard anteroposterior (AP) and cross-table lateral radiographs of the affected hip, along with an AP pelvis radiograph, are required to assess the fracture pattern, degree of displacement, and the status of the physes. In complex fracture patterns or when there is suspicion of intra-articular comminution, a fine-cut computed tomography (CT) scan with 3D reconstructions is highly recommended to delineate the fracture geometry and plan the trajectory of fixation.


The timing of surgery is a subject of academic debate, but the prevailing consensus treats displaced pediatric hip fractures as surgical urgencies, ideally addressed within 24 hours of injury. The rationale is to decompress the intracapsular hematoma, which may cause a tamponade effect on the retinacular vessels, and to mechanically realign the kinked extraosseous blood supply.


Patient positioning depends on the age and size of the child, as well as the planned approach. For older children and adolescents, a radiolucent fracture table allows for controlled traction and multi-planar fluoroscopy. The perineal post must be well-padded to prevent pudendal nerve neurapraxia. For infants and small toddlers, a standard radiolucent flat table is preferred, as pediatric fracture tables may not accommodate their small stature. In this setup, the ipsilateral hemipelvis is bumped, and the limb is prepped and draped free to allow for manual traction and manipulation. Two fluoroscopy units (or a highly mobile C-arm) should be positioned to obtain orthogonal views without moving the reduced limb.


Detailed Surgical Approach and Fixation Techniques
The surgical approach must facilitate anatomic reduction, capsular decompression, and stable fixation while respecting the delicate vascular anatomy.
Closed Reduction and Capsulotomy
Initial management involves an attempt at gentle closed reduction. Forceful or repeated manipulations are strictly prohibited, as they can further disrupt the tenuous retinacular vessels. A gentle Leadbetter maneuver or longitudinal traction with internal rotation is typically employed. If anatomic reduction is achieved closed, a percutaneous or mini-open approach can be used for fixation. However, an open capsulotomy is strongly advocated by many pediatric orthopedic surgeons to evacuate the fracture hematoma and relieve intracapsular pressure, regardless of whether the reduction was achieved closed.


Open Reduction
If closed reduction is unsuccessful, an open reduction is mandatory. The Watson-Jones (anterolateral) approach is highly effective. The internervous plane lies between the tensor fasciae latae (superior gluteal nerve) and the gluteus medius (superior gluteal nerve). While not a true internervous plane, it provides excellent access to the lateral femoral cortex and the anterior hip capsule. The capsule is incised longitudinally in line with the femoral neck. A T-type capsulotomy can be added for greater exposure, taking care to avoid the posterosuperior retinacular vessels. Direct visualization allows for precise anatomic reduction using dental picks or small pointed reduction forceps.


Fixation Strategies and Lateral Femoral Cortex Management
The choice of implant depends on the age of the patient, the Delbet classification, and the size of the femoral neck.
For infants and small children (typically under 3-4 years), smooth Kirschner wires or small partially threaded Steinmann pins are utilized to minimize physeal damage. These are often supplemented with a spica cast.
For older children and adolescents, cannulated screws (4.0 mm, 4.5 mm, or 6.5 mm depending on bone size) or pediatric dynamic hip screws (DHS) are the implants of choice. The lateral femoral cortex is the keystone of this fixation.


When placing cannulated screws, the starting point on the lateral femoral cortex must be meticulously planned. Screws should be placed in an inverted triangle configuration to maximize biomechanical stability. The inferior screw must rest on the dense bone of the calcar femorale. It is imperative to avoid creating multiple drill holes in the lateral cortex. The pediatric lateral cortex is brittle; multiple passes or closely clustered holes create a severe stress riser, significantly increasing the risk of a postoperative subtrochanteric fracture. If the lateral cortex is thin or compromised, washers should be used to prevent screw head penetration.


In Delbet Type III and IV fractures, where the fracture line exits distally, a pediatric DHS or a proximal femoral locking plate provides superior biomechanical control of varus forces compared to multiple screws. The side plate distributes the load along the lateral femoral cortex, neutralizing the deforming forces of the abductors and iliopsoas.


Complications and Salvage Management
Pediatric hip fractures carry a notoriously high complication rate, primarily due to the vulnerable vascular anatomy and the high-energy nature of the injury. Anticipation, early recognition, and aggressive management of these complications are essential.


| Complication | Incidence / Risk Factors | Clinical Presentation | Salvage and Management Strategies |
|---|---|---|---|
| Avascular Necrosis (AVN) | Up to 40% in Type I, 30% in Type II. Highest risk with delayed reduction or severe initial displacement. | Pain, limp, progressive joint space narrowing, fragmentation of the epiphysis on radiographs. | Protected weight-bearing. Proximal femoral osteotomy (varus/valgus or rotational) to contain the head. Core decompression (controversial in pediatrics). Total hip arthroplasty for end-stage collapse in older adolescents. |
| Coxa Vara | 10-20%. Associated with non-operative treatment, inadequate fixation, or failure of the lateral cortex. | Leg length discrepancy, Trendelenburg gait, restricted abduction. | Subtrochanteric valgus-producing osteotomy to restore the neck-shaft angle and improve abductor mechanics. |
| Premature Physeal Closure | 15-30%. Caused by the initial trauma or iatrogenic hardware crossing the physis. | Progressive leg length discrepancy (LLD), articular deformity. | Contralateral epiphysiodesis for LLD < 5 cm. Ipsilateral limb lengthening for LLD > 5 cm. |
| Nonunion | 5-10%. Higher in Delbet Type II and III without rigid internal fixation. | Persistent pain, hardware failure, visible radiolucent line at fracture site > 6 months post-op. | Revision internal fixation with bone grafting. Valgus osteotomy to convert shear forces into compressive forces across the fracture site. |
| Subtrochanteric Fracture | Rare but catastrophic. Caused by stress risers in the lateral femoral cortex from drill holes or hardware. | Acute pain and deformity distal to the primary fixation site. | Revision surgery utilizing a longer side plate or intramedullary device bypassing the stress riser. |


Avascular necrosis is classified using the Ratliff system. Type I involves diffuse necrosis of the entire capital femoral epiphysis and carries the worst prognosis. Type II involves partial necrosis, typically the anterolateral portion. Type III involves necrosis confined to the femoral neck from the fracture line to the physis, generally sparing the epiphysis.


Postoperative Rehabilitation Protocols
Postoperative protocols must be tailored to the patient's age, the stability of the fixation, and the integrity of the lateral femoral cortex.
In infants and children under the age of 8 to 10 years, compliance with non-weight-bearing instructions is highly unreliable. Therefore, supplemental immobilization with a 1.5-spica cast or a single-leg spica cast with an anti-rotation bar is routinely utilized for 4 to 6 weeks. This protects the internal fixation from the immense lever-arm forces generated during uncontrolled activity.

For older, compliant adolescents, strict non-weight-bearing mobilization using crutches or a walker is implemented for 6 to 8 weeks. Serial radiographs are obtained at 2 weeks, 6 weeks, and 12 weeks to assess for maintenance of reduction, hardware integrity, and signs of callus formation or endosteal healing. Weight-bearing is progressively advanced only after definitive radiographic evidence of bridging bone is observed.
Routine hardware removal is a subject of debate. If implants cross the capital femoral physis in a young child with significant remaining growth, removal is indicated once the fracture has solidly healed (typically 4 to 6 months) to prevent premature physeal tethering. If the hardware does not cross the physis and is asymptomatic, it may be left in situ. However, if the hardware creates a significant stress riser on the lateral femoral cortex, elective removal may be considered after 12 to 18 months, followed by a period of protected weight-bearing to allow the screw tracts to fill with woven bone.
Summary of Key Literature and Guidelines
The foundational literature governing the treatment of pediatric hip fractures emphasizes the urgency of anatomic reduction and the critical need for rigid internal fixation.
The Delbet classification, popularized by Colonna in the early 20th century, remains the most robust prognostic tool for predicting AVN. Ratliff's seminal work in 1962 established the definitive classification for AVN patterns following these injuries and highlighted the devastating natural history of Type I total head necrosis.
Current guidelines from the Pediatric Orthopaedic Society of North America (POSNA) and the American Academy of Orthopaedic Surgeons (AAOS) advocate for prompt surgical intervention. The debate regarding the necessity of an open capsulotomy continues; however, biomechanical and clinical studies increasingly support capsular decompression to lower intracapsular pressure, thereby theoretically reducing the incidence of AVN.

Furthermore, recent literature heavily emphasizes the biomechanical preservation of the lateral femoral cortex. Studies demonstrating the failure modes of cannulated screws in pediatric models underscore the necessity of precise starting points and the avoidance of cortical breaches, which drastically reduce the load-to-failure of the proximal femur. Mastery of these anatomical and biomechanical principles is essential for the orthopedic surgeon to unlock better outcomes in this challenging patient population.
Clinical & Radiographic Imaging
You Might Also Like