Shoulder-Spine Syndrome: Comprehensive Diagnosis & Management
Key Takeaway
Shoulder-Spine Syndrome refers to overlapping neck and shoulder pain, often posing diagnostic challenges due to anatomical proximity and shared neural pathways. It requires a thorough understanding of cervical spine and shoulder anatomy, biomechanics, and epidemiology to accurately identify the primary pain source, ensuring effective, targeted therapeutic strategies.
Shoulder-Spine Syndrome: Understanding Overlapping Neck & Shoulder Pain
Introduction & Epidemiology
Patients presenting with neck and shoulder pain frequently pose significant diagnostic challenges due to the anatomical proximity, shared neural pathways, and biomechanical interdependence of the cervical spine and glenohumeral joint complex. This constellation of overlapping symptoms, presentations, and complaints is often referred to as "Shoulder-Spine Syndrome." Clinicians, particularly spine and shoulder surgeons, must possess a thorough understanding of common pathologies affecting both regions, their characteristic presentations, appropriate examination techniques, and judicious use of diagnostic imaging to avoid inadequate diagnostic evaluations and potential mismanagement.
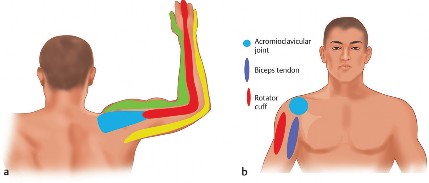
Shoulder pain is a remarkably common complaint in the general population, with a lifetime prevalence approaching 70% and a 1-year prevalence ranging from 15% to 25%. Patients often struggle to precisely localize the pain, describing a broad discomfort spanning the upper extremity, shoulder, and neck. While primary glenohumeral, acromioclavicular, or biceps tendon pathologies are frequent culprits, the cervical spine plays a critical role in differential diagnosis. Degenerative cervical spine disease and radiculopathy are well-established sources of referred shoulder pain. Epidemiological data suggest that approximately one-quarter of patients presenting with cervical radiculopathy concurrently exhibit symptomatic shoulder impingement, highlighting a significant overlap. Furthermore, cervical facetogenic pain, often less recognized, can also manifest as shoulder and scapular region discomfort, complicating the diagnostic picture.
The intricate interplay of pain patterns and neural connections between joint articulations often makes it difficult to definitively differentiate referred cervical radiculopathy from primary glenohumeral or subacromial shoulder pain. Beyond direct neural referral, an increasingly recognized aspect involves the biomechanical relationship between spinal posture and shoulder function. For instance, an association between increased thoracic kyphosis and scapular impingement syndrome has been identified. Elevated thoracic kyphosis and altered spinal inclination angles have been shown to be significant risk factors for limitations in active shoulder motion and the development of scapular dyskinesis.
The prevalence of undiagnosed or misdiagnosed shoulder-spine syndrome components is not precisely quantified, but the potential for unnecessary or ineffective surgical interventions in either domain due to an incomplete diagnostic workup remains a concern. A meticulous approach is imperative to correctly attribute the primary pain generator, thereby guiding effective therapeutic strategies.
Surgical Anatomy & Biomechanics
A profound understanding of the intricate anatomy and biomechanics of both the cervical spine and the shoulder complex is fundamental to diagnosing and treating shoulder-spine syndrome.
Cervical Spine Anatomy & Biomechanics
The cervical spine comprises seven vertebrae, C1-C7, responsible for supporting the head and providing a wide range of motion. Key structures include:
*
Vertebrae:
Body, pedicles, laminae, transverse processes, spinous processes, and articular pillars.
*
Intervertebral Discs:
Annulus fibrosus and nucleus pulposus, providing shock absorption and flexibility. Disc herniations are common sources of nerve root compression.
*
Facet Joints (Zygapophyseal Joints):
Synovial joints between the articular processes, guiding motion and weight-bearing. Degenerative changes here can cause localized and referred pain.
*
Spinal Cord and Nerve Roots:
Eight pairs of cervical nerve roots (C1-C8) exit the neural foramina. The C5, C6, C7, and C8 nerve roots are particularly relevant due to their innervation of the shoulder and upper extremity.
*
C5:
Deltoid, biceps (partial); sensation over lateral shoulder.
*
C6:
Biceps, wrist extensors; sensation over thumb and index finger.
*
C7:
Triceps, wrist flexors; sensation over middle finger.
*
C8:
Intrinsic hand muscles; sensation over ring and little fingers.
*
Musculature:
Paraspinal muscles (e.g., multifidus, semispinalis), sternocleidomastoid, scalenes, trapezius, levator scapulae. Spasm or trigger points in these muscles can refer pain to the shoulder.
Biomechanically, the cervical spine allows flexion, extension, lateral bending, and rotation. Pathologies such as disc herniation, osteophyte formation, ligamentous hypertrophy, or instability can lead to nerve root compression (radiculopathy) or spinal cord compression (myelopathy). Referred pain mechanisms involve the convergence of somatic afferents from both the cervical spine (e.g., facet joints, discs) and shoulder structures onto the same dorsal horn neurons, leading to misinterpretation of pain origin by the brain. Sclerotogenous pain patterns, specifically from cervical facet joints, can mimic subacromial or rotator cuff pathology.

This image may depict cervical spinal anatomy or a specific pathology such as disc herniation compressing a nerve root.
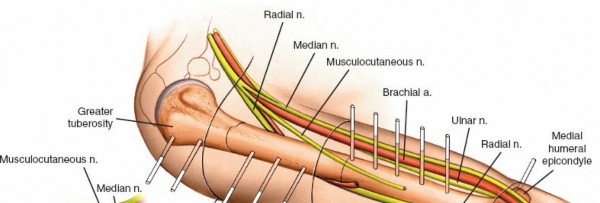
Shoulder Anatomy & Biomechanics
The shoulder complex is comprised of four joints: glenohumeral (GH), acromioclavicular (AC), sternoclavicular (SC), and the scapulothoracic articulation.
*
Glenohumeral Joint:
A highly mobile ball-and-socket joint. Key structures include:
*
Humeral Head & Glenoid:
Articular cartilage, glenoid labrum.
*
Rotator Cuff:
Supraspinatus, infraspinatus, teres minor, subscapularis. These muscles are critical for stability and dynamic motion. Tendinopathy or tears are common pain generators.
*
Biceps Tendon (Long Head):
Originates from the supraglenoid tubercle, courses through the bicipital groove. Tendinopathy or instability is a frequent source of anterior shoulder pain.
*
Capsule and Ligaments:
Superior, middle, inferior glenohumeral ligaments provide static stability.
*
Subacromial Space:
Contains the supraspinatus tendon, subacromial bursa, and long head of the biceps tendon. Impingement here is a common cause of shoulder pain.
*
Scapulothoracic Articulation:
Critical for coordinated shoulder motion, allowing glenoid positioning. Muscles include serratus anterior, rhomboids, trapezius, levator scapulae. Dysfunctional scapular mechanics (dyskinesis) can contribute to impingement and instability.
The shoulder's biomechanics are inherently linked to the cervical and thoracic spine. Scapular movement, essential for full shoulder range of motion, is directly influenced by cervical and thoracic spinal posture. For example, increased thoracic kyphosis can cause the scapula to protract and internally rotate, decreasing the subacromial space and predisposing to impingement. Conversely, chronic shoulder pain and dysfunction can lead to altered cervical muscle recruitment and posture, creating a vicious cycle. The C5-C6 dermatomes broadly encompass the lateral shoulder, making differentiation from rotator cuff pathology particularly challenging.

This image could illustrate shoulder anatomy, particularly the rotator cuff or subacromial space, highlighting potential impingement sites.
Indications & Contraindications
The management of shoulder-spine syndrome mandates a systematic diagnostic approach to identify the primary pain generator.
Diagnostic Workup
- History: Detailed history including pain character (sharp, dull, aching, burning), radiation patterns (dermatomal, non-dermatomal), aggravating/alleviating factors, onset, duration, and prior treatments. Specific inquiries regarding sensory changes (numbness, paresthesias), motor weakness, bowel/bladder dysfunction, and myelopathic symptoms are crucial.
-
Physical Examination:
-
Cervical Spine:
- Observation: Posture, muscle atrophy, scapular position.
- Palpation: Paraspinal muscles, facet joints, trapezius.
- Range of Motion (ROM): Active and passive flexion, extension, rotation, lateral bending.
- Neurological Exam: Motor strength (deltoid, biceps, triceps, wrist extensors/flexors, hand intrinsics), sensory assessment (light touch, pinprick in C5-T1 dermatomes), reflexes (biceps, triceps, brachioradialis).
- Special Tests: Spurling's maneuver (compression of nerve root), Distraction test (relief of radicular symptoms), Upper Limb Tension Tests (ULTTs).
-
Shoulder:
- Observation: Scapular position, muscle atrophy, symmetry.
- Palpation: AC joint, GH joint line, subacromial bursa, biceps groove, rotator cuff insertions.
- Range of Motion (ROM): Active and passive flexion, abduction, external rotation, internal rotation. Assess for painful arc, scapulothoracic rhythm.
- Strength Testing: Isolated testing of rotator cuff muscles (empty can, external rotation lag sign, lift-off test), deltoid, biceps.
- Special Tests: Neer's, Hawkins-Kennedy (impingement), Jobe's (supraspinatus), Speed's, Yergason's (biceps), Apprehension/Relocation (instability), O'Brien's (SLAP). Assess for scapular dyskinesis.
-
Cervical Spine:
-
Imaging:
-
Radiographs (X-rays):
- Cervical Spine: AP, lateral, oblique views (foramen visualization), flexion/extension views (instability). Look for degenerative changes, osteophytes, disc space narrowing, kyphosis.
- Shoulder: AP, scapular Y, axillary views. Look for degenerative changes, AC joint pathology, calcific tendinitis, fractures.
-
Magnetic Resonance Imaging (MRI):
- Cervical Spine: Gold standard for visualizing disc herniations, nerve root compression, spinal cord pathology, ligamentous injury, intrinsic cord lesions.
- Shoulder: Excellent for soft tissue pathology (rotator cuff tears, labral tears, biceps pathology, bursitis, synovitis).
- Computed Tomography (CT): Useful for bony detail, osteophytes, congenital anomalies, postoperative assessment of fusion or hardware. CT myelogram for complex nerve root impingement when MRI is contraindicated.
- Electromyography (EMG) and Nerve Conduction Studies (NCS): Differentiates radiculopathy from peripheral nerve entrapment (e.g., suprascapular neuropathy, brachial plexopathy) or primary myopathy. Essential in equivocal cases.
-
Radiographs (X-rays):
-
Diagnostic Injections:
- Cervical Spine: Cervical epidural steroid injection, selective nerve root block, cervical facet joint injection (medial branch block). Can confirm a spinal pain generator and provide therapeutic benefit.
-
Shoulder:
Subacromial injection, AC joint injection, glenohumeral joint injection. Can confirm a shoulder pain generator. A positive response to a well-localized diagnostic injection is a strong indicator of the pain source.

This image could be a cervical spine MRI, showing a specific pathology like a large disc herniation, guiding diagnostic decision-making.
Indications for Intervention
| Indication Type | Non-Operative Management | Operative Management |
|---|---|---|
| Cervical Spine | Acute radiculopathy (initial 6-12 weeks), mild to moderate myelopathy without progressive neurological deficit, axial neck pain, positive response to diagnostic injections. Includes physical therapy, NSAIDs, muscle relaxants, oral steroids, cervical traction, bracing, and epidural steroid injections/selective nerve root blocks. | Persistent radiculopathy (typically >6-12 weeks) despite adequate non-operative treatment, progressive neurological deficit (motor weakness), evidence of spinal cord compression (myelopathy) with clinical symptoms, intractable pain, significant functional impairment. Surgical options: ACDF, posterior foraminotomy/laminectomy, cervical arthroplasty, laminoplasty. |
| Shoulder | Acute tendinitis/bursitis, mild rotator cuff tendinopathy, small partial rotator cuff tears (non-full thickness), adhesive capsulitis (early stages), mild AC joint arthritis, symptomatic labral tears without significant instability. Includes physical therapy (ROM, strengthening, scapular stabilization), NSAIDs, activity modification, steroid injections (subacromial, AC joint, GH joint). | Full-thickness rotator cuff tears (acute/chronic), large partial-thickness rotator cuff tears, persistent impingement symptoms despite conservative management (typically >3-6 months), significant glenohumeral instability (recurrent dislocations, Bankart/Hill-Sachs lesions), advanced AC joint arthritis with failure of conservative measures, symptomatic labral tears requiring repair/debridement, severe adhesive capsulitis refractory to therapy. |
| Combined Syndrome | When primary pain generator is clearly identified and manageable conservatively, or when both pathologies are mild and not rapidly progressive. Coordinated physical therapy addressing both regions simultaneously. | When both cervical and shoulder pathologies are significant and symptomatic, requiring surgical intervention. Decision on sequential vs. simultaneous surgery based on symptoms, severity, risks. For example, severe cervical radiculopathy may need to be addressed first to prevent neurological deterioration, even if shoulder pain is also present. |
Contraindications for Surgery
- Absolute: Uncontrolled infection, severe coagulopathy, medical instability precluding safe anesthesia.
- Relative: Unrealistic patient expectations, severe psychiatric comorbidities, active smoking (for fusion procedures), mild, non-progressive symptoms responding to conservative care, poor surgical candidacy due to other systemic health issues.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for optimal outcomes in patients with shoulder-spine syndrome, especially when considering surgery for either or both regions.
Pre-Operative Assessment
- Comprehensive History and Physical: Re-evaluation of symptoms, neurological status, and physical examination findings to confirm the primary pain generator.
- Review of Imaging: Thorough review of cervical spine and shoulder radiographs, MRI, and potentially CT scans to understand the full extent of pathology.
- Anesthetic Consultation: Assessment of comorbidities and optimization of patient health. Considerations for potential prone or lateral positioning.
- Blood Management: Type and screen, considerations for cell saver or transfusion.
- Informed Consent: Detailed discussion of risks, benefits, alternatives, and potential for staged procedures if both spine and shoulder pathology require surgical intervention.
Patient Positioning
Proper positioning is paramount to ensure surgical access, patient safety, and optimal outcomes.
Cervical Spine Surgery (e.g., ACDF, Posterior Foraminotomy)
-
Anterior Approach (ACDF):
- Supine position: Head in neutral or slight extension, supported by a specialized headrest or gel donut. May use a Mayfield skull clamp for rigid fixation if deemed necessary.
- Shoulders taped caudally: To depress the shoulders, facilitating better visualization of the lower cervical spine on fluoroscopy.
- Arm tucking: Arms tucked at the sides to minimize obstruction and allow access for peripheral IVs.
- Image intensifier: Positioned for intraoperative fluoroscopy, typically for AP and lateral views.
-
Neuromonitoring:
Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs) are standard for most cervical spine surgeries, requiring careful electrode placement.

This image could depict a patient positioned for anterior cervical spine surgery, showing the head support and shoulder taping.
-
Posterior Approach (Laminectomy, Foraminotomy):
- Prone position: Torso on chest rolls or a specialized frame (e.g., Jackson table) to allow abdominal free-fall and reduce epidural venous pressure.
- Head fixation: Typically in a Mayfield skull clamp or horseshoe headrest, ensuring the neck is in a neutral or slightly flexed position to open the posterior elements. Care must be taken to avoid over-flexion, which can stretch the spinal cord.
- Arm positioning: Arms abducted and flexed, supported on armrests, or tucked at the sides.
- Neuromonitoring: As with anterior approach.
Shoulder Surgery (e.g., Rotator Cuff Repair, Decompression)
-
Beach Chair Position:
- Semi-Fowler's position: Torso elevated 30-70 degrees, knees slightly flexed.
- Head secured: In a gel donut or headrest, ensuring neutral cervical alignment.
- Operative arm: Freely draped, suspended in a traction tower for arthroscopic procedures, or resting on a padded arm board for open procedures.
- Contra-lateral arm: Tucked or on a separate arm board.
- Physiological monitoring: Special attention to potential hypotensive episodes (beach chair hypotension), especially in patients with pre-existing cerebrovascular disease.
-
Lateral Decubitus Position:
- Patient on side: Operative shoulder up, non-operative side down. Axillary roll placed to protect the brachial plexus.
- Operative arm: Suspended in a traction tower with weights (typically 10-15 lbs).
- Head and neck: Maintained in neutral alignment.
- Padding: Careful padding of all pressure points (e.g., fibular head, ulnar nerve, olecranon).
Detailed Surgical Approach / Technique
Given the nature of "Shoulder-Spine Syndrome," there is no single surgical technique to address both pathologies simultaneously in most cases. Surgical intervention is typically directed at the primary pain generator identified through a rigorous diagnostic process. If both pathologies are significant, staged procedures are usually preferred, with the more neurologically urgent or debilitating condition addressed first. Below, we discuss common surgical approaches for the primary pathologies implicated in shoulder-spine syndrome.
Addressing Cervical Radiculopathy (Primary Spinal Pain Generator)
Anterior Cervical Discectomy and Fusion (ACDF)
This is a workhorse procedure for cervical radiculopathy and myelopathy due to disc herniation or osteophyte formation.
1.
Incision:
A transverse incision (e.g., at C5-C6 level) is typically made in a skin crease on the right side of the neck (to avoid recurrent laryngeal nerve on the left, though some prefer left).
2.
Dissection:
The platysma muscle is divided. The sternocleidomastoid muscle is retracted laterally, and the strap muscles (sternohyoid, sternothyroid) medially. The carotid sheath is identified laterally and the trachea/esophagus medially. The prevertebral fascia is incised longitudinally.

This image could show the anterior neck dissection, identifying key anatomical landmarks during an ACDF.
3.
Localization:
Fluoroscopy is used to confirm the correct level.
4.
Discectomy:
Using microsurgical technique, the anterior longitudinal ligament (ALL) is incised, and the disc material is removed from the uncinate processes to the posterior longitudinal ligament (PLL). Careful decompression of nerve roots and spinal cord is performed, removing osteophytes if present, often utilizing high-speed burrs and kerrisons.
5.
Graft Placement:
An appropriately sized interbody cage, typically filled with autograft, allograft, or bone morphogenetic protein (BMP), is inserted into the disc space to restore disc height and promote fusion.
6.
Plate Fixation:
An anterior cervical plate is applied to provide immediate stability and enhance fusion rates, secured with screws into the vertebral bodies above and below the fused segment.
7.
Closure:
Layered closure of platysma and skin.
Posterior Cervical Foraminotomy
Indicated for unilateral radiculopathy due to soft disc herniation or lateral osteophyte formation, particularly when motion preservation is desired or fusion is contraindicated.
1.
Incision:
A small posterior midline incision is made over the affected level.
2.
Dissection:
Paraspinal muscles are subperiosteally elevated unilaterally to expose the lamina and facet joint.
3.
Localization:
Fluoroscopy confirms the level.
4.
Decompression:
A high-speed burr or kerrison rongeurs are used to remove a portion of the lamina and medial facet, creating a wider opening for the nerve root (keyhole foraminotomy). The nerve root is gently mobilized, and compressive disc fragments or osteophytes are removed.
5.
Closure:
Layered closure.
Addressing Shoulder Pathology (Primary Shoulder Pain Generator)
Arthroscopic Subacromial Decompression and Rotator Cuff Repair
This is a common approach for chronic impingement and rotator cuff tears, particularly relevant when shoulder pain is primary.
1.
Positioning:
Beach chair or lateral decubitus.
2.
Diagnostic Arthroscopy:
Standard posterior viewing portal is established, and the glenohumeral joint is thoroughly inspected for labral tears, biceps pathology, chondral lesions, and synovitis.
3.
Subacromial Decompression:
*
Bursectomy:
The subacromial bursa is debrided to improve visualization.
*
Acromioplasty:
The undersurface of the anterior acromion is resected using a burr to remove osteophytes and flatten the acromial undersurface, increasing the subacromial space. The coracoacromial ligament may also be released.

This image could show an arthroscopic view of the subacromial space during decompression, or an anatomical representation of the acromion.
4.
Rotator Cuff Repair (if indicated):
*
Tear Assessment:
The size, shape, and quality of the torn tendon are assessed.
*
Footprint Preparation:
The greater tuberosity footprint is débrided to bleeding bone.
*
Suture Anchor Placement:
Suture anchors (typically bioabsorbable or metal) are placed into the bone.
*
Suture Management:
Sutures are passed through the torn tendon.
*
Tendon Fixation:
The tendon is tensioned and secured to the bone using various repair configurations (single-row, double-row, transosseous equivalent techniques) to maximize contact pressure and promote healing.
5.
Biceps Tenodesis/Tenotomy (if indicated):
For symptomatic biceps pathology.
6.
Closure:
Portals are closed with suture or sterile strips.
Open Rotator Cuff Repair
Occasionally preferred for very large or complex tears, revision surgeries, or when extensive capsular work is needed.
1.
Incision:
Deltoid splitting or deltoid-sparing approach, depending on tear location and size.
2.
Dissection:
Deltoid muscle is carefully retracted to expose the rotator cuff. Acromioplasty and bursectomy are performed as needed.
3.
Tear Repair:
Similar principles to arthroscopic repair, but with direct visualization. Tendon is mobilized, débrided, and directly sutured to the bone footprint.

This image could be an intraoperative photo of an open rotator cuff repair, showing the tendon being reattached to the greater tuberosity.
Considerations for Concurrent Pathologies
When both cervical radiculopathy and significant shoulder pathology exist, the decision for sequential versus simultaneous surgery is complex:
*
Neurological Urgency:
If cervical myelopathy or progressive neurological deficit from radiculopathy is present, cervical spine surgery generally takes precedence. Addressing the spinal component first may improve neurological function and potentially alleviate referred shoulder pain, sometimes obviating the need for shoulder surgery.
*
Dominant Pain Generator:
If the patient's primary complaint is clearly either neck or shoulder, addressing that first is logical.
*
Patient Factors:
Age, comorbidities, functional demands, and patient preference play a role.
*
Technical Feasibility:
Performing extensive surgery on both regions simultaneously is typically avoided due to increased operative time, blood loss, and anesthetic risks. However, a minor, concomitant shoulder procedure (e.g., simple decompression) might be considered if the cervical spine procedure is straightforward.
Complications & Management
Both cervical spine and shoulder surgeries carry distinct risks. In the context of shoulder-spine syndrome, complications can be compounded or diagnostically challenging if overlapping symptoms persist or new ones arise.
General Surgical Complications
- Infection: Superficial or deep wound infection.
- Bleeding: Hematoma, excessive blood loss requiring transfusion.
- Nerve Injury: Peripheral nerve palsy (e.g., brachial plexus, ulnar nerve), spinal cord injury.
- Anesthetic Complications: Allergic reactions, cardiac events, pulmonary complications.
Cervical Spine Surgery Complications
| Complication | Incidence (Approximate) | Salvage Strategy / Management |
|---|---|---|
| Dysphagia (Anterior Approach) | 10-70% (transient) | Usually transient, manage with soft diet, speech therapy. Persistent cases may require swallow studies, endoscopy, or rarely, re-exploration to rule out hardware impingement or pharyngeal injury. |
| Dysphonia / Hoarseness (Recurrent Laryngeal Nerve Palsy) | 1-10% (transient) | Often transient. Speech therapy, ENT evaluation for vocal cord paralysis. May require vocal cord injection for persistent deficits. |
| C5 Palsy (Posterior Approach more common) | 2-10% | Usually motor-dominant weakness (deltoid, biceps). Often resolves spontaneously within 6-12 months. Physical therapy, bracing. Rarely requires surgical exploration. |
| Pseudarthrosis / Non-Union | 2-20% | Continued axial neck pain, hardware failure. Managed with prolonged immobilization, electrical stimulation. Revision surgery with bone grafting, plate exchange, or posterior fusion for persistent non-union. |
| Hardware Failure (Screw pull-out, plate fracture) | <5% | Pain, instability. Revision surgery for hardware removal, replacement, or supplementary fusion. |
| Dural Tear / CSF Leak | 1-3% | Intraoperative repair, bed rest, lumbar drain. For persistent leaks, re-exploration and patch. |
| Spinal Cord Injury / Worsening Myelopathy | Rare (<1%) | Immediate re-exploration, steroid administration. Often devastating, may lead to permanent neurological deficit. |
| Adjacent Segment Disease | 2-4% per year | Symptoms similar to original pathology at a new level. Managed with conservative treatment, injections. Surgical intervention (fusion or arthroplasty) if refractory. |
Shoulder Surgery Complications
| Complication | Incidence (Approximate) | Salvage Strategy / Management |
|---|---|---|
| Stiffness / Adhesive Capsulitis | 5-20% | Aggressive physical therapy, stretching, NSAIDs. Corticosteroid injections, manipulation under anesthesia, or arthroscopic capsular release for refractory cases. |
| Rotator Cuff Re-Tear | 5-25% (depending on tear size, patient factors) | Persistent pain, weakness. Revision surgery with repair, augmentation (e.g., dermal allograft), or muscle transfer (e.g., latissimus dorsi) for functional improvement. |
| Axillary Nerve Injury | Rare (<1%) | Deltoid weakness, lateral shoulder numbness. Expectant management, physical therapy. EMG/NCS for diagnosis. Surgical exploration for complete transections or non-recovering palsies. |
| Infection | <1% | Debridement, irrigation, antibiotics. Implant removal if necessary, followed by reimplantation in a staged manner. |
| Biceps Tenodesis Failure | <5% | Persistent pain in biceps groove, "Popeye" deformity. Revision tenodesis. |
| Glenohumeral Chondrolysis (Arthroscopy) | Rare | Post-operative pain and stiffness. Management includes activity modification, NSAIDs, potentially arthroplasty for severe cases. |
| Hardware Irritation (Suture anchors) | Rare | Palpable anchors, pain. Surgical removal of hardware. |
| Deltoid Detachment (Open Procedures) | Rare | Weakness, cosmetic deformity. Surgical repair with reattachment to acromion. |
Management of Persistent Symptoms in Shoulder-Spine Syndrome
If symptoms persist or worsen post-operatively, a structured re-evaluation is crucial:
1.
Re-assess Primary Pain Generator:
Was the initial diagnosis correct? Could the "secondary" pathology now be the primary issue?
2.
Rule Out Complications:
Address surgical complications first.
3.
Advanced Imaging:
Repeat MRI or CT.
4.
Diagnostic Injections:
Carefully targeted injections may help localize pain.
5.
Neurological Consultation:
If spinal symptoms are prominent.
6.
Pain Management Referral:
For chronic pain that is refractory to surgical or conservative management.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing outcomes following surgery for cervical spine or shoulder pathologies. In the context of shoulder-spine syndrome, it is imperative that rehabilitation programs are coordinated and address the potential interplay between the two regions, even if only one was surgically addressed. The goal is to restore function, reduce pain, and prevent secondary complications.
Cervical Spine Rehabilitation (Post-ACDF or Posterior Foraminotomy)
Phase 1: Acute Protection (0-6 Weeks)
*
Goals:
Protect surgical site, control pain and inflammation, gentle ROM, patient education.
*
Bracing:
Soft cervical collar often used for comfort, especially after fusion. Rigid collar may be used for specific fusion constructs or instability. Worn for 2-6 weeks depending on surgeon preference and stability.
*
Activity Restrictions:
No lifting >5-10 lbs, no repetitive neck movements, avoid prolonged static postures. No driving (especially if narcotics prescribed).
*
Therapeutic Exercise:
*
Gentle Neck ROM:
Active-assisted and active non-painful cervical flexion, extension, rotation, lateral bending (within surgeon's specified limits, especially for fusion).
*
Scapular Retractions:
To promote good posture and activate peri-scapular muscles.
*
Deep Neck Flexor Strengthening:
Isometric exercises (e.g., chin tucks) to stabilize the cervical spine.
*
Thoracic Extension Mobility:
To counteract forward head posture and prevent compensatory kyphosis.
*
Pain Management:
NSAIDs (avoid for fusion initially due to delayed bone healing), muscle relaxants, analgesics.
Phase 2: Subacute Mobility & Strengthening (6-12 Weeks)
*
Goals:
Increase cervical ROM, initiation of progressive strengthening, improve endurance.
*
Bracing:
Wean off collar if used.
*
Activity Progression:
Gradual increase in lifting limits and light daily activities.
*
Therapeutic Exercise:
*
Progressive Cervical ROM:
Full active range, gentle stretching.
*
Advanced Cervical Strengthening:
Progressive resistance for deep neck flexors, extensors, and rotators.
*
Scapular Stabilizers:
Continued emphasis on rhomboids, middle and lower trapezius.
*
Posture Correction:
Ergonomic education, postural exercises.
*
Upper Extremity Strengthening:
Initiation of light exercises, ensuring no undue strain on the cervical spine.
Phase 3: Advanced Strengthening & Return to Activity (12+ Weeks)
*
Goals:
Maximize strength and endurance, functional return, prepare for higher-level activities.
*
Therapeutic Exercise:
*
Sport-Specific/Work-Specific Training:
Gradually increase resistance and complexity of movements.
*
Core Strengthening:
To support overall spinal stability.
*
Proprioception and Balance:
Neuromuscular control exercises.
*
Return to Work/Sport:
Gradual return, guided by physical therapist and surgeon. Fusion typically takes 3-6 months for solid bony union, with full unrestricted activity often allowed at 6-12 months.
Shoulder Rehabilitation (Post-Rotator Cuff Repair or Decompression)
Phase 1: Protection & Early Passive Motion (0-6 Weeks)
*
Goals:
Protect repair, minimize pain, prevent stiffness, begin passive ROM.
*
Immobilization:
Abduction sling worn continuously (except for hygiene and exercises) for 4-6 weeks for rotator cuff repairs. Decompressions may use sling for comfort for a shorter period.
*
Activity Restrictions:
No active shoulder motion, no lifting, pushing, pulling. Avoid external rotation past neutral.
*
Therapeutic Exercise:
*
Passive Range of Motion (PROM):
Pendulum exercises, supine passive flexion, external rotation in the scapular plane (within limits to protect repair).
*
Elbow, Wrist, Hand ROM:
Active exercises to prevent stiffness.
*
Scapular Mobility:
Gentle scapular glides and protraction/retraction.
*
Pain Management:
NSAIDs, analgesics, cryotherapy.
Phase 2: Early Active Motion & Moderate Strengthening (6-12 Weeks)
*
Goals:
Restore full passive ROM, initiate active ROM, early strengthening.
*
Sling Weaning:
Gradual weaning from sling.
*
Therapeutic Exercise:
*
Active-Assistive ROM (AAROM):
Pulleys, cane exercises.
*
Active Range of Motion (AROM):
Gradually progress from gravity-eliminated positions.
*
Isometric Strengthening:
Rotator cuff, deltoid (submaximal).
*
Scapular Stabilization:
Emphasis on controlled movement, seated rows, prone extension.
*
Biceps Strengthening:
Gentle progression if not involved in repair, or delayed if tenodesis performed.
Phase 3: Advanced Strengthening & Functional Return (12-24 Weeks)
*
Goals:
Progress strength, power, endurance, return to functional and sport-specific activities.
*
Therapeutic Exercise:
*
Progressive Resistance Training:
Elastic bands, light weights for all shoulder planes, emphasizing rotator cuff and deltoid.
*
Proprioception:
PNF patterns, dynamic stabilization exercises.
*
Plyometrics:
For high-demand athletes.
*
Work/Sport-Specific Drills:
Gradual simulation of required movements.
*
Return to Activity:
Full return to unrestricted activities typically at 4-6 months, depending on tear size, repair quality, and patient progress.
Coordinated Rehabilitation for Shoulder-Spine Syndrome
When both regions are implicated, rehabilitation must be carefully tailored:
*
Sequential vs. Concurrent:
If one region was operated on, the rehab for the non-operative region can proceed concurrently, provided it does not compromise the surgical repair. For example, after cervical spine surgery, gentle shoulder ROM (especially passive) can often be initiated early. Conversely, after shoulder surgery, maintaining good cervical posture and gentle cervical ROM is important.
*
Posture Integration:
Always incorporate postural re-education to address thoracic kyphosis and scapular dyskinesis, as these biomechanical factors influence both neck and shoulder health.
*
Communication:
Close communication between the surgeon, physical therapist, and patient is paramount to ensure safe and effective progression through rehabilitation.
Summary of Key Literature / Guidelines
The understanding and management of Shoulder-Spine Syndrome continue to evolve, with increasing recognition of the complex interplay between the cervical spine and shoulder. Key literature underscores the necessity of a meticulous diagnostic approach and evidence-based treatment strategies.
Diagnostic Principles:
*
Differentiating Radiculopathy vs. Shoulder Pathology:
Studies consistently emphasize the diagnostic utility of a comprehensive history and physical examination. Specific tests, such as Spurling's maneuver for cervical radiculopathy and Neer's/Hawkins-Kennedy for shoulder impingement, possess varying sensitivities and specificities but are crucial initial screens. Diagnostic injections (e.g., subacromial lidocaine, selective nerve root blocks) remain powerful tools for localizing the primary pain generator.
*
Imaging Modalities:
MRI is universally recognized as the gold standard for soft tissue evaluation of both the cervical spine (disc herniation, myelopathy) and the shoulder (rotator cuff tears, labral pathology). Radiographs provide essential bony context. EMG/NCS are indispensable for distinguishing true radiculopathy from peripheral nerve entrapments or brachial plexopathy, as highlighted by numerous neurophysiological studies.
*
Biomechanical Links:
A growing body of literature, including studies by Lewis and McClure, has elucidated the critical role of scapular dyskinesis and thoracic posture in the development and perpetuation of shoulder pain, including impingement and rotator cuff pathology. These findings emphasize that shoulder dysfunction may not solely originate within the glenohumeral joint. Similarly, the influence of cervical and thoracic spine kinematics on upper extremity function is increasingly recognized, particularly in occupational and sports medicine settings.
Treatment Guidelines:
*
Conservative Management First:
For most cases of both cervical radiculopathy and common shoulder pathologies (e.g., tendinopathy, small partial tears, mild impingement), a trial of conservative therapy, including physical therapy, NSAIDs, and activity modification, is the first-line recommendation. Clinical practice guidelines from organizations like the North American Spine Society (NASS) and the American Academy of Orthopaedic Surgeons (AAOS) support this approach.
*
Surgical Indications:
Surgical indications for cervical radiculopathy (e.g., ACDF, posterior foraminotomy) are well-defined and typically include failure of conservative management, progressive neurological deficit, or signs of myelopathy. For shoulder pathologies, surgical intervention (e.g., arthroscopic subacromial decompression, rotator cuff repair) is typically reserved for full-thickness rotator cuff tears, persistent impingement refractory to conservative care, or significant instability.
*
Staged vs. Simultaneous Surgery:
The literature generally supports a staged approach when significant pathologies exist in both the cervical spine and the shoulder, especially if one pathology presents with neurological urgency. Addressing the more critical or neurologically threatening condition first is often favored. Decisions are highly individualized, weighing the patient's symptoms, surgical risks, and potential for one procedure to alleviate symptoms of the other. There is limited high-level evidence supporting routine simultaneous surgery for distinct significant pathologies in both regions, and caution is typically advised.
Rehabilitation:
*
Structured Protocols:
Evidence-based rehabilitation protocols, individualized to the specific surgical procedure and patient factors, are critical for optimal recovery. These protocols emphasize phased progression, focusing on pain control, restoring range of motion, progressive strengthening, and functional return.
*
Integrated Approach:
For patients with shoulder-spine syndrome, rehabilitation often requires an integrated approach, even if only one region was surgically treated. Physical therapists trained in both spinal and shoulder rehabilitation are best equipped to manage the interplay of these regions, incorporating postural correction, scapular stabilization, and gentle cervical mobility exercises as appropriate.
The ongoing challenge lies in accurately parsing the contributions of each anatomical region to the patient's overall symptomatology. Continual refinement of diagnostic algorithms and adherence to evidence-based treatment and rehabilitation protocols are paramount to effectively manage patients presenting with shoulder-spine syndrome.

This final image could represent a summary algorithm for diagnosis, or a graphic highlighting the interconnectedness of the shoulder and spine, reinforcing the comprehensive nature of this academic review.
Clinical & Radiographic Imaging


You Might Also Like