Open Reduction of Supracondylar Fractures of the Humerus
Open Reduction of Supracondylar Fractures of the Humerus
Introduction & Epidemiology
Supracondylar fractures of the humerus represent the most common elbow fracture in the pediatric population, accounting for approximately 60-70% of all elbow fractures in children. While less common in adults, their occurrence in older individuals often indicates higher energy trauma and frequently involves greater comminution or intra-articular extension, posing unique challenges. The vast majority of these fractures, particularly in children, are extension-type injuries resulting from a fall on an outstretched hand, leading to hyperextension of the elbow. Flexion-type injuries are less frequent but tend to be more unstable and are often associated with direct trauma to the posterior elbow.
The classification system by Gartland remains a widely utilized clinical tool for pediatric supracondylar fractures:
*
Type I:
Nondisplaced.
*
Type II:
Displaced with an intact posterior cortex.
*
Type III:
Completely displaced with no cortical contact.
*
Type IV (recently added):
Multidirectionally unstable in both flexion and extension.
The primary goal of treatment is to achieve and maintain anatomical reduction, restore normal elbow function, and prevent complications. The standard of care for displaced supracondylar fractures (Gartland Types II, III, and IV) is typically closed reduction and percutaneous pinning (CRPP) . This approach offers favorable outcomes with minimal soft tissue disruption.
However, a supracondylar fracture that necessitates open reduction is one that cannot be adequately or safely managed with closed reduction and percutaneous pinning. This inability may arise from severe displacement, soft tissue interposition, associated neurovascular compromise requiring direct intervention, or an open fracture. The decision to proceed with an open reduction is therefore a critical one, often indicating a more complex injury pattern or failed less invasive attempts. While open reduction is often associated with higher complication rates, it remains an indispensable technique for specific, challenging presentations to ensure optimal fracture healing and functional recovery.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy surrounding the distal humerus is paramount for safe and effective open reduction of supracondylar fractures. The distal humerus itself consists of medial and lateral columns converging proximally at the supracondylar ridges, forming a triangular cross-section. The trochlea (medially) articulates with the ulna, and the capitellum (laterally) articulates with the radial head. The olecranon fossa posteriorly and the coronoid/radial fossae anteriorly accommodate the respective processes of the ulna and radius during elbow motion.
Neurovascular Anatomy
The neurovascular structures around the elbow are highly susceptible to injury during fracture displacement or iatrogenically during surgical intervention.
- Brachial Artery and Median Nerve: These structures pass through the antecubital fossa, medial to the biceps tendon. In cases of severe fracture displacement, particularly extension-type fractures where the distal fragment displaces posteriorly and proximally, the proximal humeral shaft fragment can buttonhole through the anterior capsule and brachialis muscle, tenting the skin and bringing the brachial artery and median nerve into immediate subcutaneous proximity anteriorly. This places them at significant risk during skin incision for an anterior approach, and meticulous dissection is required. The median nerve also gives off the anterior interosseous nerve distally, which innervates the deep flexors of the forearm.
- Ulnar Nerve: The ulnar nerve passes behind the medial epicondyle, within the cubital tunnel. It is particularly vulnerable during medial approaches, medial K-wire insertion, or in flexion-type fractures where the distal fragment displaces anteriorly and medially. Pre-existing ulnar nerve palsy can occur due to acute trauma or delayed presentation due to malunion (tardy ulnar nerve palsy).
- Radial Nerve: The radial nerve courses from posterior to anterior in the spiral groove of the humerus, then divides into the superficial (sensory) and deep (posterior interosseous, motor) branches just proximal to the lateral epicondyle. It lies in close proximity to the lateral column of the distal humerus and can be at risk during lateral surgical approaches or with excessive soft tissue stripping laterally. The posterior interosseous nerve wraps around the radial neck and can be entrapped.
Musculoskeletal and Ligamentous Anatomy
The surrounding musculature also plays a role in fracture displacement and can act as interposing tissue preventing closed reduction.
*
Anteriorly:
The brachialis muscle attaches to the coronoid process and ulna. The biceps brachii inserts via its tendon into the radial tuberosity. The pronator teres originates from the medial epicondyle and inserts into the radial shaft.
*
Medially:
The common flexor origin muscles (pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris) originate from the medial epicondyle.
*
Laterally:
The common extensor origin muscles (extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, extensor carpi ulnaris, supinator) originate from the lateral epicondyle.
*
Posteriorly:
The triceps brachii inserts into the olecranon.
The medial (ulnar) and lateral (radial) collateral ligaments provide primary elbow stability. While direct injury to these ligaments is less common in pure supracondylar fractures, their integrity is crucial for overall elbow function and joint stability once the fracture is reduced and fixed.
Biomechanics
The common hyperextension mechanism results in an extension-type fracture, where the distal fragment is typically displaced posteriorly and often medially, with varying degrees of rotation. The pull of the forearm flexors and extensors on the distal fragment and the triceps on the proximal fragment can contribute to displacement and often makes reduction challenging. Excessive posterior displacement, as noted, can lead to impingement or entrapment of the brachial artery and median nerve. The degree of soft tissue injury, including muscle tears and periosteal stripping, correlates with the energy of injury and can impact fracture stability and healing.
Indications & Contraindications
The decision to proceed with an open reduction of a supracondylar humerus fracture is made when conventional, less invasive methods are deemed inadequate or unsafe. This typically implies a complex presentation that cannot be resolved by closed reduction and percutaneous pinning (CRPP).
Indications for Open Treatment of a Supracondylar Fracture
The primary indications for open reduction include:
*
Irreducible fracture by closed methods:
This is the most common indication. It may be due to:
* Significant soft tissue interposition (e.g., periosteum, brachialis muscle, median nerve, brachial artery) preventing anatomical alignment.
* Buttonholing of the proximal fragment through the anterior capsule or brachialis muscle.
* Severe rotational displacement that cannot be corrected closed.
* Inability to maintain reduction for stable pinning.
*
Open fractures:
Regardless of reducibility, open fractures require surgical debridement and typically open reduction to thoroughly clean the wound, assess soft tissue damage, and achieve stable fixation.
*
Vascular compromise requiring exploration and repair:
* Pulseless but perfused hand ("pink pulseless hand") that does not regain pulse after closed reduction.
* Ischemic hand ("white pulseless hand") with signs of impending ischemia (pallor, poikilothermia, paresthesia, paralysis, pain).
* Any evidence of arterial injury (e.g., intimal tear, thrombosis, complete transection) requiring surgical exploration and often vascular reconstruction (e.g., primary repair, vein graft).
*
Associated neurological deficit requiring direct decompression or repair:
While most nerve palsies are neurapraxias and resolve spontaneously, some may require open exploration if persistent or if nerve entrapment is suspected.
*
Compartment Syndrome:
Evidence of evolving compartment syndrome in the forearm necessitates urgent fasciotomy, which may be combined with open reduction and fixation of the supracondylar fracture.
*
Delayed Presentation / Chronic Fractures:
Fractures presenting more than 7-10 days after injury often develop significant callus formation and soft tissue contractures, making closed reduction impossible. Open reduction may be necessary to achieve reduction, albeit with increased challenges and potential for stiffness.
*
Floating Elbow:
Concurrent ipsilateral forearm fracture (Monteggia, Galeazzi, or both bone forearm fracture) often mandates open reduction of at least one of the fractures to ensure stable fixation of both segments.
Contraindications
Absolute contraindications to open reduction are rare when an indication exists for limb salvage or restoration of function. However, relative contraindications include:
*
Unstable medical comorbidities:
Patients unable to tolerate general anesthesia or the physiological stress of prolonged surgery. These situations necessitate medical optimization prior to surgery, if possible.
*
Active local infection:
Untreated infection at the surgical site would increase the risk of osteomyelitis and should be addressed prior to definitive fracture fixation, if feasible.
*
Minor displacement that is amenable to non-operative treatment:
Gartland Type I fractures do not require open reduction.
*
Successful closed reduction and stable percutaneous pinning:
If a satisfactory reduction and stable fixation can be achieved by closed means, open reduction is unnecessary and contraindicated due to increased morbidity.
Table of Operative vs. Non-Operative Indications
| Indication Type | Operative Approach (Open Reduction) | Non-Operative Approach (Closed Reduction & Pinning / Cast) |
|---|---|---|
| Fracture Reducibility & Stability |
- Failed closed reduction (irreducible fracture)
- Inability to maintain reduction - Significant soft tissue interposition |
- Gartland Type I (Nondisplaced)
- Gartland Type II, III, IV successfully reduced closed with stable pinning |
| Vascular Status |
- Pulseless hand not regaining pulse after reduction
- Ischemic hand (white pulseless) - Confirmed arterial injury requiring repair |
- Pink pulseless hand with return of pulse after reduction
- Perfused limb with intact distal pulses and capillary refill |
| Neurological Status |
- Persistent severe neurological deficit
- Suspected nerve entrapment - Open nerve injury requiring repair |
- Transient neurapraxia
- Resolving nerve palsy - Intact neurological examination |
| Fracture Type & Soft Tissue |
- Open fractures (Gustilo-Anderson Grade I-III)
- Associated compartment syndrome - Severe displacement with skin tenting |
- Closed fractures
- No signs of compartment syndrome - Adequate soft tissue envelope without impending compromise |
| Timing of Presentation | - Delayed presentation (>7-10 days) with early callus formation making closed reduction impossible | - Acute presentation (<7 days) allowing for easier manipulation and reduction |
| Associated Injuries | - Floating elbow (ipsilateral forearm fracture requiring stable fixation) | - Isolated supracondylar fracture without other significant musculoskeletal injuries requiring open intervention |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and anticipating potential challenges in open reduction of supracondylar humerus fractures.
Pre-Operative Planning
-
Clinical Assessment:
- Detailed History: Mechanism of injury, time since injury, prior medical history, allergies, medications.
- Neurovascular Examination: This is paramount. Document all pulses (radial, ulnar), capillary refill, skin color, temperature, sensation (median, ulnar, radial nerve distributions), and motor function (finger flexion/extension, wrist flexion/extension, forearm pronation/supination). Any deficits must be thoroughly documented as a baseline.
- Soft Tissue Assessment: Evaluate for skin integrity, open wounds, tenting, or signs of impending compromise.
-
Radiographic Evaluation:
- Plain Radiographs: Anteroposterior (AP) and true lateral views of the elbow are essential. Obtain views of the entire humerus, forearm, wrist, and hand if associated injuries are suspected. Assess fracture pattern, degree and direction of displacement, comminution, and any intra-articular extension. Specific radiographic measurements like Baumann's angle and the anterior humeral line are crucial for assessing reduction quality.
-
Computed Tomography (CT) Scan:
While not routinely indicated for acute pediatric supracondylar fractures, CT may be invaluable for:
- Complex fracture patterns, especially in older children or adults.
- Suspected intra-articular extension or subtle comminution.
- Assessment of chronic or neglected fractures to understand callus formation and deformity.
- Pre-operative planning for plate fixation.
- Anesthetic Consultation: Assess patient's fitness for general anesthesia, especially in pediatric patients or those with comorbidities.
-
Equipment Preparation:
- Standard orthopedic surgical tray.
- Small fragment instrument set.
- K-wire driver and assorted K-wires (1.6 mm, 2.0 mm typically).
- Image intensifier (C-arm) with lead aprons.
- Vessel loops, vascular clamps, micro-vascular instruments if vascular repair is anticipated.
- Nerve stimulator, nerve protectors.
- Tourniquet.
- Bone graft substitutes (for chronic cases/non-union).
- Prophylactic antibiotics, usually a first or second-generation cephalosporin.
- Informed Consent: Discuss the risks and benefits of open reduction, including potential complications such as infection, bleeding, nerve injury, vascular injury, malunion (e.g., cubitus varus), nonunion, stiffness, need for revision surgery, and hardware issues.
Patient Positioning
Proper patient positioning is critical for maximizing surgical exposure, ensuring C-arm access, and preventing iatrogenic injury.
*
General Anesthesia:
Administered after securing airway.
*
Tourniquet:
Applied to the proximal arm, ensuring adequate padding. A sterile tourniquet may be considered if a posterior approach is anticipated to avoid repeated draping.
*
Supine Position:
The patient is typically positioned supine on a radiolucent operating table.
*
Arm Positioning:
The affected arm is usually placed on a radiolucent hand table, allowing for free movement and projection for C-arm imaging. Alternatively, the arm can be draped across the chest, which is convenient for a medial or lateral approach, providing good access for imaging without repositioning. The shoulder should be abducted to 90 degrees and the elbow flexed to allow full range of motion.
*
Padding:
All pressure points, especially around the contralateral elbow and heels, must be meticulously padded to prevent pressure neuropathies or skin breakdown.
*
C-arm Access:
Ensure the C-arm can be freely moved to obtain AP, lateral, and oblique views of the elbow without contamination of the sterile field or interference with surgical instruments. It's often helpful to pre-position the C-arm and perform a dry run to confirm adequate imaging capability.
Detailed Surgical Approach / Technique
The choice of surgical approach for open reduction of a supracondylar humerus fracture depends largely on the specific indication, fracture pattern, and structures at risk. Regardless of the approach, meticulous soft tissue handling, careful identification and protection of neurovascular structures, and accurate anatomical reduction are paramount.
General Principles
- Prophylactic Antibiotics: Administer intravenous antibiotics prior to incision.
- Tourniquet: Inflate the tourniquet on the proximal arm after exsanguination.
- Sterile Technique: Standard sterile preparation and draping.
- C-arm: Have the image intensifier readily available throughout the procedure for confirmation of reduction and hardware placement.
Surgical Approaches
1. Anterior Approach (Modified Henry's Approach or Brachialis Split)
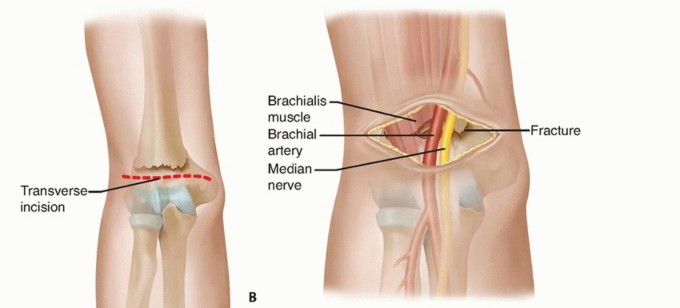
- Indications: Primarily for vascular exploration and repair (e.g., pulseless limb), or for irreducibility due to anterior soft tissue interposition (e.g., brachialis muscle or median nerve entrapment).
- Incision: A longitudinal incision centered over the antecubital fossa, extending proximally along the anterior aspect of the humerus and distally into the forearm.
-
Internervous Plane:
- Medial to Biceps/Brachialis: Develop the interval between the biceps/brachialis (musculocutaneous innervation) and the pronator teres (median nerve innervation). This approach places the median nerve and brachial artery at high risk and requires careful identification and retraction.
- Brachialis Split: A more direct approach to the fracture site by splitting the brachialis muscle longitudinally. This can be performed between its radial and ulnar innervations.
-
Dissection:
- Incise skin and subcutaneous tissue. Identify and protect superficial veins and cutaneous nerves (e.g., medial cutaneous nerve of the forearm, lateral cutaneous nerve of the forearm).
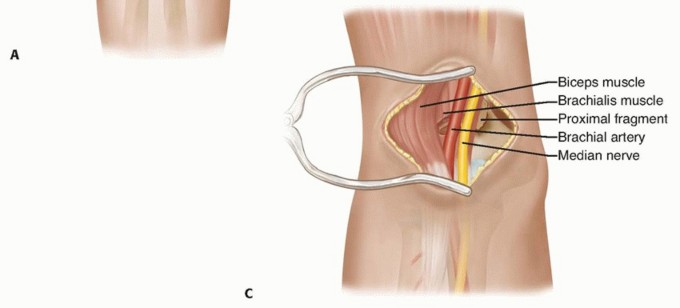
- Carefully identify the brachial artery and median nerve. These structures are often displaced and may be draped over the proximal fragment or entrapped within the fracture hematoma. Use vessel loops to gently retract and protect them.
- Ligate or coagulate small perforating vessels.
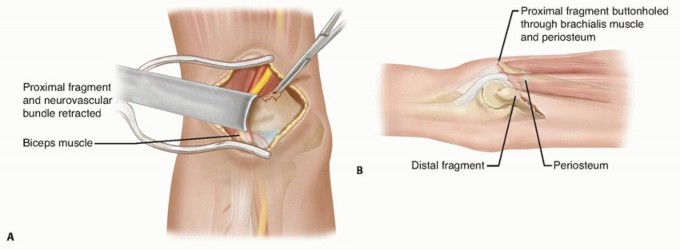
- If the brachialis muscle is torn or buttonholed, identify its edges. The fracture site will be deep to or through the brachialis.
- Once neurovascular structures are identified and protected, the fracture site is exposed.
-
Reduction:
Direct visualization allows for removal of any interposing soft tissue. Gentle traction, leverage with elevators, and direct manipulation can be used to achieve anatomical reduction. Rotational alignment is critical.
-
Integrate
here, ideally depicting the anterior neurovascular bundle or a relevant anterior view of the fracture.
-
Integrate
2. Medial Approach
- Indications: Medial column comminution, medial epicondyle fracture, ulnar nerve exploration/decompression, or when a medial pin is deemed necessary for stability in open cases.
- Incision: A longitudinal incision centered over the medial epicondyle, extending proximally along the supracondylar ridge.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Identify and isolate the ulnar nerve, which lies in the cubital tunnel posterior to the medial epicondyle. It should be carefully protected, potentially transposed anteriorly if extensive exposure or fixation on the medial column is required.
- Incise the common flexor origin from the medial epicondyle and reflect it anteriorly, or split the flexor carpi ulnaris (FCU) muscle.
- Expose the medial supracondylar ridge and fracture site.
- Reduction: Direct reduction of the medial column.
- Fixation: Primarily K-wires, potentially small fragment plates depending on the patient's age and fracture pattern.
3. Lateral Approach (Kocher's Approach Variation)
- Indications: Often preferred for lateral column comminution or for irreducible extension-type fractures where the lateral column requires direct visualization. It generally carries a lower risk to major neurovascular structures (brachial artery, median nerve) compared to an anterior approach.
- Incision: A longitudinal incision centered over the lateral epicondyle, extending proximally along the lateral supracondylar ridge.
-
Dissection:
- Incise skin and subcutaneous tissue. Identify and protect superficial nerves (e.g., lateral cutaneous nerve of the forearm, posterior cutaneous nerve of the forearm).
- Incise the common extensor origin from the lateral epicondyle and reflect it anteriorly or posteriorly.
- Alternatively, the interval between the anconeus and the extensor carpi ulnaris (both radial nerve innervated) can be developed, but this is more distal. For supracondylar fractures, the dissection usually proceeds more proximally, reflecting muscle off the lateral column.
- Carefully identify and protect the radial nerve and its branches as they course anteriorly to the capitellum and posteriorly in the spiral groove proximally.
- Expose the lateral supracondylar ridge and fracture site.
- Reduction: Direct reduction of the lateral column and overall fracture alignment.
-
Fixation:
K-wires are typically inserted from the lateral epicondyle/metaphysis. For complex adult fractures, lateral column plates may be used.
-
Integrate
here, likely depicting a lateral approach or K-wire configuration from the lateral side.
-
Integrate
4. Posterior Approach (Triceps Sparing or Olecranon Osteotomy)
- Indications: Highly comminuted fractures, severe intra-articular extension, chronic non-unions, or situations requiring extensive exposure of the distal humerus, especially for posterior plating. More common in adults or very complex pediatric cases.
- Incision: A posterior longitudinal incision centered over the olecranon, extending proximally along the triceps tendon and distally over the ulna.
-
Dissection:
- Triceps Sparing: Develop the interval between the medial and lateral heads of the triceps. The ulnar nerve must be identified and carefully protected, often requiring anterior transposition. This approach offers limited distal exposure.
-
Olecranon Osteotomy:
This provides the widest exposure to the distal humerus and articular surface.
- Identify and protect the ulnar nerve.
- Perform an osteotomy of the olecranon (e.g., chevron or transverse) and reflect the entire triceps-olecranon complex proximally.
- Expose the posterior aspect of the distal humerus.
- Reduction: Excellent direct visualization for reconstruction of complex fractures.
-
Fixation:
K-wires, often supplemented by small fragment plates (medial and lateral column plating is common for adults). The olecranon osteotomy must be anatomically reduced and stably fixed (e.g., tension band wiring, plate and screws).
-
Integrate
here, likely illustrating a posterior approach or plate fixation strategy.
-
Integrate
Reduction and Fixation Techniques
-
Reduction:
- After exposing the fracture, remove any interposing soft tissue.
- Apply gentle longitudinal traction to disimpact the fragments.
- Address the displacement in a systematic manner: correct sagittal plane (extension/flexion), then coronal plane (valgus/varus), and finally rotational deformity.
- Use reduction clamps, pointed reduction forceps, or bone hooks to achieve and maintain anatomical alignment.
- Confirm reduction visually and with C-arm imaging (AP and lateral views). Ensure the anterior humeral line passes through the middle third of the capitellum on the lateral view and Baumann's angle (angle between the lateral humeral epicondylar physis and a line along the capitellum) is restored to within normal range (typically 65-75 degrees, compare to contralateral side if possible).
-
Fixation (K-wires for pediatric, Plates for complex/adult):
-
K-wires (Pediatric):
- Lateral Entry Pins: Two or three divergent pins inserted from the lateral epicondylar region, engaging both cortices of the proximal fragment. This technique minimizes the risk to the ulnar nerve. Optimal configurations include two lateral divergent pins or three pins (two lateral, one medial) carefully placed.
- Crossed Pins: A lateral pin and a medial pin (from the medial epicondyle). While biomechanically stronger, the medial pin carries a risk of ulnar nerve injury. If a medial pin is necessary, a mini-open technique or direct visualization of the ulnar nerve is highly recommended.
- Technique: Drive K-wires using a power drill or hand chuck, aiming for bicortical purchase. Ensure pin trajectories provide maximal stability. Bend the pins and cut them externally for easy removal, or bury them subcutaneously if prolonged fixation is needed.
-
Plates (Adult/Complex Pediatric):
- Mini-fragment plates or specialized distal humerus plates may be used, particularly for comminuted fractures or in older adolescents/adults where K-wire fixation may not be sufficient.
- Dual plating (medial and lateral columns) is often preferred for stable fixation of complex supracondylar fractures. These plates can be applied from a combined medial and lateral approach, or a posterior approach with an olecranon osteotomy.
- Ensure appropriate screw length and purchase.
-
K-wires (Pediatric):
Closure
- Release the tourniquet and achieve meticulous hemostasis.
- Irrigate the wound thoroughly.
- Close the soft tissues in layers. Repair any incised muscle or fascia.
- Consider a drain if there is significant dead space or concern for hematoma formation.
- Close skin with staples or sutures.
- Apply a sterile dressing and a well-padded long arm posterior splint with the elbow flexed to approximately 60-90 degrees and the forearm in neutral rotation.
Complications & Management
Open reduction of supracondylar humerus fractures, while often necessary for complex presentations, is associated with a higher rate of complications compared to closed reduction and percutaneous pinning. Vigilant monitoring and prompt management are crucial.
General Surgical Complications
- Infection: Superficial or deep surgical site infection. Incidence is generally low (1-5%) but higher than for closed cases. Management includes antibiotics, debridement, and potentially hardware removal.
- Hematoma: Collection of blood within the surgical site, potentially leading to swelling, pain, and increased pressure. Management involves observation, aspiration, or surgical evacuation.
- Anesthetic Complications: Standard risks associated with general anesthesia (e.g., allergic reactions, respiratory or cardiovascular events).
Specific Complications of Supracondylar Fractures (and Open Reduction)
| Complication | Incidence (General Estimates) | Salvage Strategy / Management |
|---|---|---|
| Neurovascular Injury |
Pre-op nerve injury: 10-20%
Iatrogenic nerve injury: 1-5% Vascular injury: 0.5-1% (higher in open fractures or severe displacement) |
Nerve:
- Pre-existing: Most are neurapraxias; observe for resolution (typically 6-12 weeks). Electrophysiological studies (EMG/NCS) if no recovery. - Iatrogenic: Immediate exploration if discovered intraoperatively. Post-op, if new deficit, consider early exploration to rule out entrapment or transection. Nerve repair/grafting if transected. Transposition for ulnar nerve irritation. Vascular: - Ischemic limb: Immediate surgical exploration, thrombectomy, primary repair, or interposition vein graft. Consider fasciotomy. - Pink pulseless limb: If no pulse after successful reduction, observe closely for perfusion; if signs of ischemia, explore. If absent radial pulse persists but hand is well perfused, typically observe, but discuss with vascular surgeon. |
| Malunion |
Cubitus varus: 5-15% (can be higher for open cases)
Cubitus valgus: Rare Rotational: 1-5% |
Cubitus Varus ("Gunstock Deformity"):
Most common. Primarily cosmetic, but can lead to tardy ulnar nerve palsy. Corrective osteotomy (supracondylar dome or wedge osteotomy) indicated for significant deformity or functional issues.
Cubitus Valgus: Less common, but can impact elbow mechanics. Corrective osteotomy. Rotational Malunion: May be tolerated unless functionally limiting. |
| Nonunion |
Rare in pediatric supracondylar (<0.1%)
Higher in adults, open fractures, or re-operations. |
Debridement of fibrous tissue, bone grafting (autograft or allograft), stable internal fixation (plates and screws), potentially with external fixation if severe bone loss. |
| Stiffness / Loss of Motion | 10-20% (higher after open reduction and prolonged immobilization) | Early, gentle active and active-assisted range of motion (ROM) exercises. Physical therapy. Avoid forced manipulation. Manipulation under anesthesia or arthrolysis may be considered for refractory cases. |
| Compartment Syndrome | <1% (but higher risk with vascular injury, severe swelling, or unrecognized ischemia) | Urgent fasciotomy (typically forearm volar and dorsal compartments). Monitor tissue viability and subsequent wound management. |
| Hardware Complications |
Pin migration: 1-2%
Pin tract infection: 2-5% Breakage/Prominence: Varies |
Pin Migration/Breakage:
Removal of offending hardware. Revision fixation if fracture stability is compromised.
Pin Tract Infection: Local wound care, oral antibiotics. Pin removal once fracture healed. If deep infection, surgical debridement. Hardware Prominence/Irritation: Elective hardware removal after fracture healing. |
| Volkmann's Ischemic Contracture | <0.1% (end-stage, severe complication of unresolved ischemia/compartment syndrome) | Prevention is key (early recognition and treatment of vascular compromise/compartment syndrome). Salvage often involves extensive reconstructive procedures (e.g., tendon transfers, muscle slides, neurolysis, fasciotomy release) to improve function, but full recovery is rare. |
Management Principles
- Early Recognition: High index of suspicion for developing complications, especially neurovascular compromise and compartment syndrome. Regular neurovascular checks are paramount post-operatively.
- Documentation: Meticulous documentation of pre-operative, intra-operative, and post-operative neurovascular status.
- Multidisciplinary Approach: Collaborate with vascular surgeons, neurologists, and rehabilitation specialists as needed.
- Patient and Family Education: Inform about potential complications and signs/symptoms to watch for.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following open reduction of supracondylar humerus fractures is crucial for restoring elbow function, minimizing stiffness, and optimizing long-term outcomes. The protocol must be tailored to the individual patient, considering age, fracture stability, quality of fixation, and presence of any complications.
Phase 1: Immobilization and Protection (Approximately 0-4 weeks)
-
Immediate Post-Op:
- Immobilization: A well-padded long arm posterior splint or cast is applied. The elbow is typically positioned in 60-90 degrees of flexion, and the forearm in neutral rotation. This position is generally considered safe and comfortable.
- Elevation: Keep the arm elevated to minimize swelling, especially in the first 48-72 hours.
- Ice: Apply ice packs to the elbow region to help reduce swelling and pain.
- Pain Management: Administer appropriate analgesia.
- Neurovascular Checks: Perform frequent and thorough neurovascular checks for at least 48-72 hours post-surgery to monitor for any signs of neurovascular compromise or compartment syndrome.
- Pin Site Care (if K-wires used): Keep pin sites clean and dry. Monitor for signs of infection.
- Duration of Immobilization: Typically 3-4 weeks for simple fractures, possibly longer (up to 6 weeks) for complex, comminuted, or unstable fractures, or if plate fixation was used. Radiographic evidence of early callus formation is a guide.
- Early Motion (Non-Fracture Related): Encourage active range of motion of the shoulder, wrist, and hand to prevent stiffness in these joints.
Phase 2: Controlled Mobilization (Approximately 4-8 weeks)
- Initiation: This phase typically begins after removal of K-wires (if applicable) and/or confirmation of adequate fracture stability on radiographs.
- Hardware Removal (K-wires): K-wires are usually removed in the clinic setting around 3-4 weeks post-operatively once clinical and radiographic healing is evident.
-
Gentle Range of Motion (ROM):
- Active-Assisted ROM (AAROM): Begin gentle, active-assisted elbow flexion and extension exercises. Patients can use their unaffected hand to assist the affected arm.
- Active ROM (AROM): Progress to active elbow flexion and extension as tolerated, within pain-free limits.
- Forearm Rotation: Begin gentle pronation and supination exercises.
- Avoid Forced Manipulation: Crucially, avoid aggressive or forced stretching, as this can exacerbate inflammation, increase pain, and potentially lead to heterotopic ossification or refracture.
- Physical Therapy: Referral to a physical therapist is highly recommended to guide and monitor the rehabilitation process.
- Splinting: A removable splint may be used between exercise sessions for comfort and protection, especially at night.
- Initiate Light Strengthening (Isometric): Gentle isometric exercises for elbow flexors and extensors may be introduced if fracture stability is excellent and without pain.
Phase 3: Progressive Strengthening and Functional Recovery (Approximately 8-12+ weeks)
- Progression: As ROM improves and pain subsides, focus shifts towards regaining full strength and functional use of the arm.
-
Strengthening Exercises:
- Progressive resistive exercises for elbow flexors, extensors, pronators, and supinators.
- Incorporate light weights, resistance bands, or bodyweight exercises.
- Gradually increase intensity and repetitions.
-
Functional Activities:
- Introduce activities that mimic daily tasks (e.g., reaching, lifting light objects).
- Sport-specific drills may be initiated for athletes.
- Addressing Residual Stiffness: If residual stiffness persists, the therapist may employ techniques such as joint mobilizations or sustained stretching. Dynamic or static progressive splinting may be considered for recalcitrant contractures.
- Monitoring: Continue to monitor for any signs of delayed complications (e.g., tardy ulnar nerve palsy due to cubitus varus).
- Hardware Removal (Plates): For plate fixation, hardware removal is typically considered 12-18 months post-operatively, usually after full fracture consolidation and when the patient has regained satisfactory function, or if symptoms related to hardware irritation arise.
Return to Activity
- Light Activities: Return to light, non-contact activities can generally begin once full pain-free ROM is achieved, and strength is approaching normal (typically 3-4 months post-op).
- Full Contact Sports/Heavy Lifting: Return to full contact sports or heavy manual labor is usually delayed until 4-6 months post-operatively, or when the patient has regained full strength, ROM, and confidence, and there is clear radiographic evidence of fracture union.
Summary of Key Literature / Guidelines
The management of supracondylar humerus fractures, particularly the indications for and techniques of open reduction, has evolved significantly over decades. Current literature and clinical guidelines emphasize a stepwise approach, reserving open intervention for specific, challenging scenarios.
-
Shift Towards Minimally Invasive Management: Historically, open reduction was more common. However, the seminal work by authors like Gartland (1959) describing the classification system, and subsequent advancements in surgical techniques, particularly closed reduction and percutaneous pinning (CRPP) , have firmly established CRPP as the gold standard for displaced pediatric supracondylar fractures. Numerous studies have demonstrated excellent outcomes with CRPP, citing lower complication rates, less soft tissue disruption, and faster rehabilitation compared to open methods.
-
Indications for Open Reduction: Current consensus, supported by bodies like the American Academy of Orthopaedic Surgeons (AAOS) , reiterates that open reduction is indicated primarily when closed reduction fails, for open fractures, or when there is associated neurovascular compromise requiring direct exploration.
- Irreducible Fractures: Studies by Skaggs et al. (1998) and others have highlighted that soft tissue interposition (brachialis muscle, median nerve, anterior capsule) is a common cause of irreducibility, necessitating an open approach.
- Vascular Injury: The management of a pulseless limb associated with supracondylar fractures remains a topic of debate. The "pink pulseless hand" (good perfusion despite absent pulse) often resolves with closed reduction and observation, as documented by Blake and McBryde (1975) and Campbell et al. (1995) . However, the "white pulseless hand" or persistent pulselessness despite adequate reduction, particularly with signs of ischemia, mandates urgent vascular exploration via an anterior approach, as emphasized by Flynn et al. (1975) . The long-term outcomes of observed pink pulselessness without vascular repair are generally favorable, but close monitoring is paramount.
- Open Fractures: Gustilo and Anderson's (1976) classification for open fractures guides the principle that these injuries require surgical debridement and appropriate fixation, often favoring open reduction for thorough wound management and stable fixation.
-
Surgical Approaches:
- Anterior Approach: While historically associated with higher rates of stiffness, the anterior approach remains critical for vascular exploration and repair. Schoenecker et al. (2018) provides a comprehensive review, acknowledging its utility in specific vascular scenarios.
- Medial/Lateral Approaches: Direct medial or lateral approaches are less common for primary open reduction of the entire fracture but are useful for addressing specific column comminution or for facilitating K-wire placement when a direct approach is needed to protect the ulnar nerve (medial side).
- Posterior Approach (Olecranon Osteotomy): This approach, often used in adults with complex distal humerus fractures, provides excellent visualization for comminuted supracondylar fractures, particularly when dual plating is indicated. Ring et al. (2006) demonstrated good results with parallel plating for complex adult distal humerus fractures, a technique adaptable to supracondylar patterns.
-
Fixation Principles:
- K-wires: For pediatric patients, K-wire fixation after open reduction follows similar biomechanical principles as CRPP. Gordon et al. (2001) reviewed various pinning configurations, generally favoring lateral divergent pins or crossed pins with careful ulnar nerve protection.
- Plate Fixation: In older adolescents and adults, small fragment plates, particularly medial and lateral column plating, provide superior stability for comminuted fractures. This approach aims to reconstruct the architectural integrity of the distal humerus, as described by O'Driscoll et al. (2001) for distal humerus fractures.
-
Outcomes and Complications: Open reduction, while effective, generally carries a higher risk of complications than CRPP. Malunion , particularly cubitus varus, remains a concern, with incidence rates varying but generally higher than with CRPP. Stiffness is also more prevalent due to increased soft tissue dissection and potentially longer immobilization. Neurological injury , both pre-existing and iatrogenic, requires diligent monitoring and management. Flynn et al. (1962) highlighted the risks of Volkmann's ischemic contracture as a devastating, albeit rare, complication of severe supracondylar fractures.
In summary, the contemporary management of supracondylar humerus fractures emphasizes a staged approach. Open reduction is a valuable, and at times indispensable, surgical tool reserved for complex, irreducible, or compromised fractures. Adherence to meticulous surgical technique, careful neurovascular protection, and a structured rehabilitation protocol are crucial for achieving optimal patient outcomes and mitigating the inherent risks associated with this challenging injury.
Clinical & Radiographic Imaging
You Might Also Like