Distal Humerus Fractures: Epidemiology, Advanced Anatomy & Biomechanics

Key Takeaway
Distal humerus fractures are complex elbow injuries, primarily categorized by AO/OTA classification. Successful management demands deep understanding of surgical anatomy, including medial/lateral columns and neurovascular structures, alongside biomechanical principles of fixation. Dual plating, often orthogonal or parallel, is standard to restore stability, enabling early rehabilitation and preserving functional range of motion for improved patient outcomes.
Mastering Distal Humerus Fractures: Diagnosis & Treatment
Introduction & Epidemiology
Distal humerus fractures (DHFs) represent a challenging subset of elbow trauma, accounting for approximately 2-7% of all adult fractures and up to 30% of elbow fractures. Their incidence exhibits a bimodal distribution: affecting younger individuals primarily due to high-energy trauma (e.g., motor vehicle accidents, falls from height) and the elderly population secondary to low-energy falls, often in the context of osteopenia or osteoporosis. The anatomical complexity of the distal humerus, involving the intricate articular surface of the trochlea and capitellum, coupled with the proximity of vital neurovascular structures, renders these injuries significant. Prognosis is heavily dependent on achieving and maintaining an anatomical reduction of the articular surface and stable fixation, allowing for early rehabilitation and restoration of functional range of motion (ROM).
The primary goal of managing DHFs is to achieve a stable, pain-free elbow with a functional arc of motion (typically 30-130 degrees of flexion-extension and 50 degrees of pronation-supination). Historically, outcomes have been variable, with high rates of stiffness, pain, and post-traumatic arthritis. However, advancements in surgical techniques, implant design, and rehabilitation protocols have significantly improved patient outcomes.
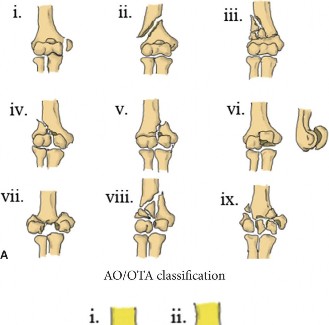
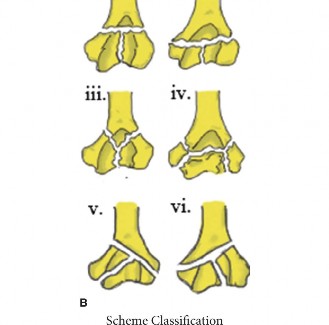
Classification systems are crucial for guiding treatment and predicting prognosis. The AO/OTA classification is widely accepted, categorizing fractures by their complexity:
*
Type A:
Extra-articular (A1 simple, A2 wedge, A3 multifragmentary).
*
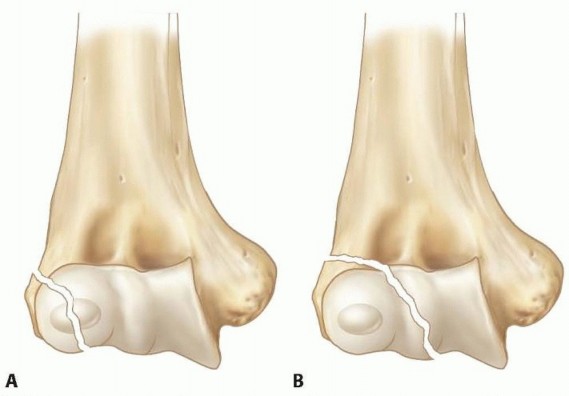
Type B:
Partial articular (B1 lateral sagittal, B2 medial sagittal, B3 frontal).
*
Type C:
Complete articular (C1 articular simple, metaphyseal simple; C2 articular simple, metaphyseal multifragmentary; C3 articular multifragmentary, metaphyseal multifragmentary).
Type C fractures, particularly C2 and C3, present the greatest reconstructive challenge due to the involvement of both articular and metaphyseal components. Other systems, such as the Riseborough and Radin classification, categorize based on the degree of comminution and displacement, but the AO/OTA system offers a more detailed surgical blueprint.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the distal humerus is paramount for successful management of these fractures.
Surgical Anatomy
The distal humerus forms the proximal aspect of the elbow joint. Key anatomical features include:
*
Articular Surface:
The trochlea medially articulates with the trochlear notch of the ulna, and the capitellum laterally articulates with the radial head. Both are covered with articular cartilage. The trochlea extends further distally and anteriorly than the capitellum, forming the medial column.
*
Columns:
The distal humerus is classically described as a "three-column" structure by Riseborough and Radin, later simplified to "two columns" (medial and lateral) for surgical planning.
*
Medial Column:
Formed by the medial epicondylar ridge, medial epicondyle, and trochlea. It is significantly stronger and broader than the lateral column and is crucial for varus stability.
*
Lateral Column:
Formed by the lateral epicondylar ridge, lateral epicondyle, and capitellum. It is more slender and prone to comminution.
*
Fossae:
The olecranon fossa posteriorly and the coronoid and radial fossae anteriorly accommodate the olecranon, coronoid process, and radial head during elbow flexion and extension, respectively. These fossae are separated by a thin bony septum, which is often perforated.
*
Neurovascular Structures:
*
Ulnar Nerve:
Lies in the cubital tunnel posterior to the medial epicondyle. It is highly susceptible to injury during exposure, reduction, and fixation, and can be irritated by hardware or post-operative scarring.
*
Radial Nerve:
Winds around the posterior aspect of the humeral shaft, proximally to the distal humerus, making it less vulnerable in direct distal humeral exposures but at risk during more proximal shaft extension of fracture patterns or during lateral column plating.
*
Median Nerve and Brachial Artery:
Located anterior to the distal humerus, protected by the brachialis muscle. They are at risk during anterior approaches or extensive anterior dissection.
*
Musculotendinous Attachments:
The common flexor origin arises from the medial epicondyle, and the common extensor origin from the lateral epicondyle. The triceps inserts onto the olecranon, providing posterior stability and power for extension.
Biomechanics
The biomechanical principles of distal humerus fracture fixation are derived from its columnar anatomy:
*
Load Bearing:
The medial and lateral columns bear compressive loads from the ulna and radius, respectively. The trochlea (medial column) transmits the majority of axial load (60%), while the capitellum (lateral column) transmits approximately 40%.
*
Fixation Stability:
Stable fixation must counteract bending, torsional, and shear forces across the fracture site to allow for early, protected motion. The concept of dual plating, utilizing two plates on the medial and lateral columns, has become the standard of care. This construct aims to restore stability to both columns and rigidly fix the articular segment to the humeral shaft.
*
Orthogonal (90/90) Plating:
One plate along the posterior aspect of the lateral column and a second plate along the medial aspect of the medial column. The screws from each plate are designed to engage the opposite column. This configuration provides excellent stability against varus/valgus and shear forces.
*
Parallel Plating:
Both plates are applied to the posterior aspect of the medial and lateral columns. This technique offers biomechanical equivalence or superiority to orthogonal plating in some studies, particularly in resisting torsional loads, and may reduce hardware prominence laterally.
*
Articular Congruity:
Restoration of the articular surface is paramount. Any step-off or gap exceeding 1-2 mm can lead to accelerated post-traumatic arthritis. Lag screw fixation of articular fragments is crucial before column fixation.
*
Muscle Forces:
The powerful triceps muscle can exert significant distractive forces on the fracture, necessitating robust fixation. Early mobilization helps prevent capsular contracture and muscle atrophy.
Indications & Contraindications
The decision to proceed with operative versus non-operative management for distal humerus fractures is based on a multitude of factors, including fracture morphology, patient demographics, comorbidities, and functional demands.
Indications for Operative Management (ORIF)
- Displaced Intra-articular Fractures (AO/OTA Type B & C): The vast majority of these fractures require anatomical reduction and stable internal fixation to restore articular congruity and allow for early motion.
- Significantly Displaced Extra-articular Fractures (AO/OTA Type A): Displacement leading to unacceptable angulation or shortening, or compromising neurovascular structures.
- Open Fractures: Require urgent debridement and stabilization.
- Fracture-Dislocations of the Elbow: Concurrent dislocation often necessitates surgical stabilization of the humeral fracture.
- Neurovascular Compromise: Urgent surgical exploration and repair of vessels or nerves, often requiring concomitant fracture stabilization.
- Failure of Non-Operative Treatment: Progressive displacement in a previously stable fracture managed conservatively.
- Multiple Trauma Patients: Early stabilization of elbow fractures can facilitate overall patient management and rehabilitation.
Indications for Non-Operative Management
- Non-Displaced or Minimally Displaced Extra-articular Fractures (AO/OTA Type A): Stable fractures that can be managed with a brief period of immobilization followed by early motion.
- Medically Unstable Patients: Those with significant comorbidities (e.g., severe cardiac or pulmonary disease, advanced dementia) for whom the risks of general anesthesia and surgery outweigh the potential benefits of ORIF.
- Non-Ambulatory Patients / Low Functional Demands: Elderly, frail patients with very limited functional expectations who would not tolerate extensive rehabilitation. For complex intra-articular fractures in this subgroup, total elbow arthroplasty (TEA) may be considered, but some may still be managed non-operatively with prolonged immobilization for comfort.
Contraindications to Operative Management
-
Absolute Contraindications:
- Severe active infection at the surgical site.
- Extensive soft tissue loss or devitalization precluding safe wound closure and increasing infection risk (may necessitate external fixation as a temporary measure).
-
Relative Contraindications:
- Severe medical comorbidities that significantly increase surgical risk (ASA IV/V status).
- Extreme osteoporosis where stable fixation is unlikely, potentially making total elbow arthroplasty a more viable primary option.
- Patients with documented non-compliance with rehabilitation protocols, as early motion is critical for successful outcomes.
Summary of Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Type | Displaced intra-articular fractures (AO/OTA Type B & C) | Non-displaced or minimally displaced extra-articular fractures (AO/OTA Type A) with minimal comminution and stable alignment. |
| Significantly displaced extra-articular fractures (AO/OTA Type A) | ||
| Associated Injuries | Open fractures, fracture-dislocations, neurovascular compromise | Isolated fractures without significant soft tissue compromise or neurovascular injury. |
| Patient Factors | Young, active patients with high functional demands | Medically unfit patients with high surgical risk (ASA ≥ III) |
| Patients with good bone quality amenable to stable fixation | Elderly, frail patients with very low functional demands (comfort-based management) | |
| Treatment Course | Failed non-operative treatment (e.g., progressive displacement) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful distal humerus fracture management.
Pre-Operative Planning
-
Imaging:
- Standard Radiographs: Anteroposterior (AP), lateral, and oblique views of the elbow are the initial imaging modalities. These provide basic information regarding fracture type, displacement, and comminution.
- Computed Tomography (CT) Scan: Essential for complex intra-articular fractures (AO/OTA Type B and C). Fine-cut CT scans with 2D and 3D reconstructions provide invaluable detail regarding the articular surface, fragment orientation, and the extent of comminution. This allows for precise identification of the capitellum and trochlea fragments, guiding reduction strategy. Angiography may be indicated if a vascular injury is suspected (e.g., absent pulse, expanding hematoma).
-
Templating:
- Using the CT scans and radiographs, surgeons should pre-operatively template the surgical approach, plate selection (length, width, contour), and screw trajectories.
- Identify the key articular fragments and plan their reduction sequence. Determine whether an olecranon osteotomy will be necessary for adequate visualization.
- Pre-bend reconstruction plates or select pre-contoured locking plates to match the distal humerus anatomy.
-
Implants:
- Ensure availability of a comprehensive distal humerus plating system, including small fragment screws (2.0, 2.4, 2.7 mm) for articular reconstruction, and 3.5 mm locking and non-locking screws for column fixation.
- K-wires (1.6 mm or 2.0 mm) are critical for temporary reduction and stabilization of articular fragments.
- If an olecranon osteotomy is planned, have tension band wiring kits or partially threaded cancellous screws available for osteotomy fixation.
- Ulnar Nerve Management Plan: Decide pre-operatively whether the ulnar nerve will be transposed or left in situ after protection, considering the chosen approach and extent of planned hardware. For most olecranon osteotomies, anterior transposition is often favored.
- Tourniquet: Plan for a pneumatic tourniquet to achieve a bloodless field, which is critical for accurate identification of structures and precise articular reduction.
Patient Positioning
The choice of patient position is dictated by the chosen surgical approach and surgeon preference.
1.
Lateral Decubitus Position:
*
Advantages:
Most commonly used position for posterior approaches. Allows the arm to be draped freely across a chest roll or support, facilitating dynamic intraoperative imaging (C-arm) and manipulation of the elbow joint. The unaffected arm can be positioned on an arm board.
*
Setup:
Patient is placed on their side, with the affected arm draped over a sterile arm rest or bolster. The ipsilateral hip is flexed, and the contralateral leg is straight or slightly flexed. Adequate padding of all pressure points is essential.
2.
Prone Position:
*
Advantages:
Provides excellent posterior access and allows for simultaneous bilateral arm access if needed. It can be useful for very proximal extensions of the fracture.
*
Setup:
Patient is prone on the operating table. The affected arm is typically positioned on an arm board or hangs freely, allowing for flexion/extension and pronation/supination.
3.
Supine Position:
*
Advantages:
Less commonly used for complex distal humerus fractures requiring posterior exposure. It may be considered for simple extra-articular fractures or specific anterior approaches.
*
Setup:
Patient is supine with the affected arm on an arm board, often with the elbow flexed to 90 degrees.
4.
C-arm Positioning:
Ensure the C-arm can obtain adequate AP and lateral views of the distal humerus and elbow joint without repositioning the patient or breaking sterility. This typically involves positioning the C-arm perpendicular to the limb axis for AP views and parallel for lateral views.
Detailed Surgical Approach / Technique
The goal of surgical fixation for distal humerus fractures is to achieve anatomic reduction of the articular surface and provide stable internal fixation to the medial and lateral columns, allowing for early controlled motion. The posterior approach is most commonly employed.
Posterior Surgical Approaches
1. Olecranon Osteotomy (Gold Standard for Complex Intra-articular Fractures)
This approach provides unparalleled visualization of the articular surface and is typically preferred for complex AO/OTA Type C fractures.
- Incision: A straight posterior midline incision is made from approximately 8-10 cm proximal to the olecranon to the tip of the olecranon, extending distally along the ulnar crest.
-
Ulnar Nerve Identification and Transposition:
- The subcutaneous tissue is carefully dissected. The ulnar nerve must be identified early in the procedure, typically found posterior to the medial epicondyle, exiting the cubital tunnel.
- It is then carefully dissected free from its bed for a sufficient length (approximately 6-8 cm proximally and distally) to allow for mobilization.
- The nerve is protected with a vessel loop or Penrose drain and is typically transposed anteriorly at the conclusion of the case, especially with hardware placement that might impinge on its posterior course.
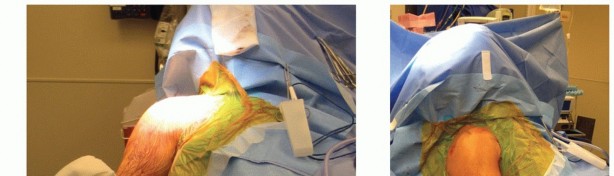
-
- Caption: Careful identification and protection of the ulnar nerve is paramount during posterior approaches, often requiring formal anterior transposition.
- Triceps Dissection: The triceps tendon is separated from the posterior capsule and periosteum on either side of the olecranon.
-
Olecranon Osteotomy:
- Technique: A chevron or transverse osteotomy is performed in the olecranon, typically at the base of the trochlear notch or slightly more proximally. This allows the olecranon fragment, with the attached triceps, to be reflected proximally, providing excellent exposure of the distal humerus and articular surface.
- Pre-drill screw holes for subsequent re-fixation if using screws. Use an oscillating saw under copious irrigation. Protect the articular cartilage of the trochlear notch during the osteotomy.
-

- Caption: Intraoperative view following an olecranon osteotomy, providing wide exposure of the distal humeral articular surface.
2. Triceps-Sparing / Triceps-Reflecting Approaches (e.g., Bryan-Morrey, Triceps Elevation)
These approaches avoid an olecranon osteotomy, potentially reducing associated complications, but may offer less comprehensive articular visualization, particularly for highly comminuted intra-articular fractures.
- Bryan-Morrey Approach: The triceps tendon is incised sharply off the olecranon along its lateral or medial border and reflected, typically exposing the posterior aspect of the distal humerus. The triceps can then be repaired back to the olecranon through drill holes.
- Triceps Elevation: The triceps is elevated subperiosteally or with a thin cuff of periosteum from the posterior aspect of the distal humerus and olecranon. This maintains the integrity of the triceps tendon insertion.
- Advantages: Avoids osteotomy-related complications (nonunion, hardware prominence, pain).
- Disadvantages: May limit exposure of the most distal articular fragments, especially the capitellum and trochlea, in highly comminuted fractures.
-
- Caption: Illustration of a triceps-sparing approach, elevating the triceps muscle to expose the distal humerus without an olecranon osteotomy.
Reduction and Fixation Principles
Regardless of the approach, the general principles of open reduction and internal fixation (ORIF) remain consistent:
-
Articular Surface Reconstruction:
- This is the critical first step. Identify and reduce the largest articular fragments (capitellum, trochlea).
- Use K-wires for temporary stabilization. Small lag screws (2.0 or 2.4 mm) are then used to achieve interfragmentary compression and create a smooth, anatomic articular surface.
- Ensure no step-off or gap greater than 1-2 mm. Intraoperative fluoroscopy and direct visualization are crucial.
-

- Caption: Articular reduction achieved with temporary K-wires, followed by lag screw fixation to restore a smooth joint surface.
-
Columnar Fixation (Medial and Lateral Columns):
- Once the articular block is reconstructed, it must be rigidly fixed to the humeral shaft. Dual plating is the standard.
- Plate Selection: Pre-contoured locking plates are generally preferred, as they match the complex anatomy of the distal humerus and provide enhanced stability, especially in osteoporotic bone. Plates should be sufficiently long to gain adequate purchase in the humeral diaphysis.
-
Orthogonal (90/90) Plating:
- A plate is applied to the medial aspect of the medial column, extending proximally along the supracondylar ridge.
- A second plate is applied to the posterior aspect of the lateral column, extending proximally along the lateral supracondylar ridge.
- Screws from the lateral plate are directed medially into the medial column, and vice versa. This creates a strong construct resisting varus/valgus and shear forces.
-

- Caption: Orthogonal (90/90) plating construct. Note the plate on the medial epicondyle and the plate on the posterolateral column, with screws crossing into the opposing column.
-
Parallel Plating:
- Both plates are placed on the posterior aspect of the medial and lateral columns. This arrangement is often preferred for its ease of application, reduced hardware prominence laterally, and excellent biomechanical stability, particularly against torsional loads.
- Screws are directed to engage the opposite column or to maximize bone purchase within their respective columns.
-
- Caption: Parallel plating construct. Both plates are positioned on the posterior aspect of the medial and lateral columns, providing robust fixation.
- Screw Selection: Locking screws are typically used in the distal fragment where bone purchase may be limited due to comminution or osteoporosis. Cortical screws are used more proximally in the diaphysis. Ensure bicortical screw purchase where possible.
- Diaphyseal Fixation: Once the distal articular block is stably fixed, the plates are secured to the humeral shaft using appropriate screws.
-
Final Assessment:
- Check for stability of the construct with full elbow range of motion.
- Confirm anatomical reduction and hardware position with intraoperative fluoroscopy in multiple planes.
- Ensure full range of motion without impingement of hardware.
Closure
- Olecranon Osteotomy Repair: If an osteotomy was performed, it is meticulously repaired. This can be done with two or three partially threaded cancellous screws (often 4.0 mm or 4.5 mm) augmented by a figure-of-eight tension band wire, or with dedicated olecranon plating systems. Ensure stable fixation to allow early triceps activation.
- Ulnar Nerve Repositioning: Decide whether to transpose the ulnar nerve anteriorly. Most surgeons prefer anterior submuscular transposition to prevent irritation from hardware and to place it in a softer tissue bed.
- Layered Closure: Repair the triceps if incised or elevated. Close the deep fascia, subcutaneous tissue, and skin in layers.
- Dressings: Apply a sterile dressing and a well-padded posterior splint with the elbow flexed at approximately 90 degrees for initial comfort and protection, allowing for slight pronation/supination.
Complications & Management
Distal humerus fractures are associated with a significant rate of complications due to the complexity of the injury, the surgical exposure, and the intensive rehabilitation required.
Common Complications and Management
| Complication | Incidence | Description & Management / Salvage Strategy |
|---|---|---|
| Ulnar Neuropathy | 10-30% |
Can be transient (traction injury, swelling, hematoma, contusion) or persistent (entrapment, transection, hardware impingement).
Presentation: Numbness/tingling in small finger/ulnar half of ring finger, weakness of intrinsic hand muscles. Management: Initial observation for transient symptoms (nerve usually recovers within 3-6 months with conservative management including NSAIDs, nerve gliding exercises). For persistent or progressive symptoms, consider electrodiagnostic studies. If non-resolving or worsening, surgical exploration, neurolysis, and formal anterior transposition (if not already performed) may be indicated. Hardware removal may be necessary if it is the source of impingement. |
| Elbow Stiffness / Loss of ROM | 20-50% |
A major concern, often due to arthrofibrosis, capsular contracture, heterotopic ossification (HO), or inadequate early rehabilitation. Limited flexion/extension and/or pronation/supination.
Management: Aggressive physical therapy is key, often starting within days of surgery. Dynamic progressive splinting may be used. If stiffness persists despite maximal non-operative efforts after 6-9 months, consider manipulation under anesthesia (MUA) or arthroscopic/open arthrolysis (capsular release, removal of impinging HO). Prevention includes meticulous soft tissue handling, early motion, and HO prophylaxis. |
| Nonunion / Malunion | 5-15% |
Nonunion:
Failure of fracture to heal after 6-9 months.
Malunion:
Healing in an unacceptable position (e.g., severe angulation, rotation, articular step-off).
Causes: Inadequate reduction or fixation, infection, poor bone quality, extensive comminution, early weight-bearing. Management: Nonunion: Revision ORIF with plate exchange, bone grafting (autograft or allograft), and enhanced fixation stability. In elderly, low-demand patients, total elbow arthroplasty (TEA) can be an excellent salvage option. Malunion: May require corrective osteotomy if symptomatic and severe. For severe articular malunion with pain and functional deficit, TEA is often considered. |
| Post-traumatic Arthritis | 10-25% (long-term) |
Progressive articular cartilage degeneration due to residual articular incongruity, instability, or chronic inflammation.
Presentation: Chronic pain, crepitus, loss of motion. Management: Initial conservative management (NSAIDs, activity modification, steroid injections). For advanced symptomatic arthritis, treatment options include arthroscopic debridement, interposition arthroplasty, or ultimately, total elbow arthroplasty (TEA) in older, low-demand patients, or distal humeral hemiarthroplasty in specific cases. |
| Infection | 2-5% |
Superficial or deep surgical site infection.
Presentation: Pain, redness, swelling, fever, purulent drainage. Management: Prompt identification. Superficial infections may respond to oral antibiotics. Deep infections require surgical debridement, irrigation, tissue cultures, intravenous antibiotics, and potentially hardware removal (if union has occurred). In severe cases with hardware involvement and nonunion, a staged approach (debridement, external fixation, delayed reconstruction) may be necessary. |
| Hardware Prominence / Failure | 5-10% |
Plates or screws becoming palpable, causing pain, skin irritation, or impinging on soft tissues. Screws breaking or plates bending/breaking.
Causes: Inadequate contouring, poor bone quality, high stress on hardware. Management: Prominence: Hardware removal after fracture union (typically 12-18 months post-op) if symptomatic. Failure: Indicates underlying instability or nonunion; requires revision surgery with more robust fixation and/or bone grafting. |
| Heterotopic Ossification (HO) | 5-20% |
Ectopic bone formation in soft tissues around the elbow, leading to mechanical blockade of motion.
Management: Prophylaxis with NSAIDs (e.g., Indomethacin for 3-6 weeks) or single-dose radiation therapy (7-8 Gy within 24-72 hours post-op), particularly in high-risk patients (e.g., concomitant head injury, burns, open fractures). Once mature and symptomatic, surgical excision may be performed, ideally after 9-12 months when the HO has fully matured and vascularity is reduced. Concurrent prophylactic measures are again utilized after excision. |
| Olecranon Osteotomy Complications | 5-10% |
Nonunion or symptomatic hardware (prominence, irritation).
Management: Nonunion: Revision fixation (e.g., plating), bone grafting. Symptomatic hardware: Removal after osteotomy union. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as surgical fixation for achieving optimal outcomes following distal humerus fracture repair. The protocol aims to restore joint motion, strength, and function while protecting the surgical repair. Close collaboration between the surgeon and physical therapist is essential.
General Principles
- Early Motion: The primary goal of stable internal fixation is to permit early, controlled range of motion to prevent stiffness and promote cartilage health.
- Gradual Progression: Exercises are advanced gradually based on fracture stability, patient tolerance, and healing progress.
- Pain Management: Adequate pain control is crucial to facilitate participation in therapy.
- Patient Education: Patients must understand the importance of adherence to the protocol and the potential for long-term recovery.
Phased Rehabilitation Protocol
Phase I: Immediate Post-Operative (Weeks 0-2)
- Goals: Control pain and swelling, protect surgical repair, initiate gentle range of motion.
-
Protection:
- Initially, a well-padded posterior splint (elbow at 90 degrees flexion, neutral forearm) is applied for comfort and protection from inadvertent movements. It may be removed for hygiene and exercises.
- Avoid direct pressure on the ulnar nerve pathway.
-
Motion:
- Active-Assisted Range of Motion (AAROM): Begin with gentle, pain-free AAROM and passive range of motion (PROM) for elbow flexion/extension and forearm pronation/supination.
- Gravity-assisted exercises (e.g., pendulums) can be introduced cautiously.
- Avoid: Lifting, carrying, pushing, or pulling. No active strengthening.
-
Other:
- Cryotherapy and elevation to minimize edema.
- Scar massage initiated once the wound is well-healed.
Phase II: Early Motion & Gentle Strengthening (Weeks 2-6)
- Goals: Progressively increase range of motion, begin light strengthening.
-
Motion:
- Continue to increase PROM and AROM for flexion, extension, pronation, and supination. Aim for increased functional arc of motion.
- Continuous Passive Motion (CPM) machine may be used by some therapists, though evidence for routine use is mixed.
-
Strengthening:
- Initiate light isometric exercises for elbow flexors (biceps), extensors (triceps), pronators, and supinators.
- Gentle grip strengthening.
- Avoid any exercises involving resistance or weight-bearing through the elbow.
-
Activities:
- Continue scar management.
- Progress with activities of daily living (ADLs) within protected limits.
Phase III: Progressive Strengthening & Functional Activities (Weeks 6-12)
- Goals: Restore full functional range of motion, increase strength and endurance.
-
Motion:
- Continue to work towards full elbow ROM. Dynamic splinting may be introduced for persistent flexion or extension deficits.
-
Strengthening:
- Progress to light isotonic exercises for biceps, triceps, forearm muscles (flexion, extension, pronation, supination).
- Begin with low weights and high repetitions, gradually increasing resistance.
- Initiate shoulder strengthening exercises to support overall upper extremity function.
-
Activities:
- Functional strengthening exercises relevant to work or hobbies.
- Gradual increase in weight-bearing through the extremity.
Phase IV: Advanced Strengthening & Return to Activity (Weeks 12+)
- Goals: Maximize strength, power, and endurance; return to sport/work-specific activities.
-
Strengthening:
- Continue progressive resistive exercises.
- Introduce eccentric strengthening.
- Plyometric exercises may be considered for athletes.
-
Activities:
- Gradual return to unrestricted activities, including sport-specific drills or heavy labor, once adequate strength, motion, and stability are achieved (typically 6-12 months post-surgery).
- Full recovery can take up to a year or more.
- Long-term Monitoring: Continue to monitor for signs of post-traumatic arthritis, heterotopic ossification, or neurological symptoms.
Key Considerations:
- Bone Healing: Radiographic evidence of fracture healing (callus formation, bridging bone) is important, but clinical stability and pain are primary drivers for rehabilitation progression.
- Ulnar Nerve Symptoms: Monitor for any signs of ulnar nerve irritation, which may require modification of exercises or further intervention.
- Individualization: Each patient's recovery trajectory is unique. The protocol must be tailored to the individual's progress, pain levels, and surgical findings (e.g., bone quality, extent of comminution).
Summary of Key Literature / Guidelines
The literature on distal humerus fractures continually evolves, refining surgical techniques and patient management strategies. Several key concepts and recent advancements underpin current best practices.
-
AO/OTA Classification and Surgical Principles:
- The AO/OTA classification remains the most widely accepted system for categorizing distal humerus fractures, providing a standardized language for communication and guiding treatment algorithms.
- The fundamental principles of anatomical reduction of the articular surface and stable internal fixation of the medial and lateral columns continue to be the cornerstone of surgical management for most displaced fractures.
-
Dual Plating Constructs:
- Numerous biomechanical studies have consistently demonstrated the superiority of dual-plate fixation over single-plate fixation for complex distal humerus fractures.
- Orthogonal (90/90) vs. Parallel Plating: Early biomechanical studies often favored orthogonal plating for its robust resistance to varus/valgus bending. However, more recent biomechanical and clinical studies suggest that parallel plating constructs (both plates on the posterior aspect of the columns) offer comparable or even superior biomechanical stability, particularly against torsional forces, with potentially fewer issues related to hardware prominence. The choice often comes down to surgeon preference and the specific fracture pattern. Both are acceptable strategies.
-
Locking Plate Technology:
- The advent of locking plate technology has significantly improved fixation stability, especially in comminuted fractures and osteoporotic bone. Locking screws create a fixed-angle construct, resisting pullout and maintaining reduction even in poor bone quality. This has been a major contributing factor to improved outcomes, allowing for earlier and more aggressive rehabilitation.
-
Surgical Approaches:
- Olecranon Osteotomy: Remains the gold standard for achieving optimal visualization and anatomical reduction of complex intra-articular fractures (Type C). While associated with potential complications (osteotomy nonunion, hardware pain), its benefits in achieving precise articular reconstruction often outweigh these risks.
- Triceps-Sparing Approaches: Are gaining popularity for less comminuted fractures or in specific situations where osteotomy complications are a major concern. They offer the advantage of avoiding olecranon osteotomy-related morbidity but may compromise the extent of articular visualization. The choice depends on the fracture pattern and surgeon experience.
-
Role of Total Elbow Arthroplasty (TEA):
- For severely comminuted intra-articular distal humerus fractures in elderly, low-demand patients with osteoporotic bone where stable ORIF is unlikely to be achieved, primary total elbow arthroplasty (TEA) has emerged as a viable and often superior option. TEA can provide immediate stability, allow early motion, and often results in reliable pain relief and functional outcomes in this specific patient population, bypassing the challenges and potential complications of complex ORIF.
-
Rehabilitation:
- The literature consistently emphasizes the critical role of early, protected range of motion protocols post-ORIF. Prolonged immobilization is detrimental and leads to severe stiffness. Close collaboration with physical therapists is essential for gradual progression of exercises tailored to the fracture stability and patient tolerance.
-
Complication Management:
- Ulnar neuropathy remains the most common complication. Routine ulnar nerve identification and consideration for anterior transposition are widely recommended, especially with olecranon osteotomy or extensive hardware.
- Heterotopic ossification (HO) is a recognized complication, particularly in high-energy trauma, often managed with prophylactic NSAIDs or radiation in at-risk patients.
The AO Foundation, through its educational programs and publications, continues to provide widely accepted guidelines and recommendations for the management of distal humerus fractures, emphasizing a systematic approach to diagnosis, planning, and surgical execution. Continued research focuses on improving implant design, refining surgical techniques, and optimizing rehabilitation strategies to further enhance outcomes and minimize complications.
Clinical & Radiographic Imaging

You Might Also Like