Solving Unstable SCFE: Subcapital Realignment with Extended Retinacular Flap
Key Takeaway
This topic focuses on Solving Unstable SCFE: Subcapital Realignment with Extended Retinacular Flap, The extended retinacular flap is a vital part of the subcapital realignment with surgical dislocation technique, chosen to treat unstable Slipped Capital Femoral Epiphysis (SCFE). This advanced surgical method facilitates gentle reduction and stabilization of severe hip slips, aiming to restore proper femoral head alignment while carefully preserving vascularity for optimal patient outcomes.
Introduction and Epidemiology
Slipped Capital Femoral Epiphysis represents one of the most common adolescent hip disorders, characterized by the displacement of the proximal femoral epiphysis from the metaphysis through the hypertrophic zone of the physis. The condition is classically categorized by temporal duration, morphological severity, and functional stability. The Loder classification dictates functional stability, defining unstable Slipped Capital Femoral Epiphysis as the inability of the patient to ambulate even with crutches. Unstable slips are associated with a significantly higher risk of avascular necrosis of the femoral head, historically reported to be as high as fifty percent following traditional in situ pinning or closed reduction maneuvers.
The epidemiological profile of Slipped Capital Femoral Epiphysis typically involves adolescents undergoing rapid pubertal growth spurts, generally occurring between the ages of ten and sixteen years. There is a well-documented predilection for males and a strong association with obesity, which alters the mechanical forces acting across the proximal femoral physis. Endocrine abnormalities, such as hypothyroidism, growth hormone deficiency, and renal osteodystrophy, are frequently implicated, particularly in atypical presentations, bilateral cases, or patients outside the standard age demographic.
Historically, the management of unstable Slipped Capital Femoral Epiphysis focused on preventing further displacement through in situ pinning. However, this approach inherently accepts a severe residual deformity of the proximal femur. The unreduced metaphysis creates a profound cam morphology, leading to obligatory femoroacetabular impingement, early chondral damage, and rapid progression to secondary osteoarthritis. To mitigate these long term sequelae, the surgical paradigm has shifted toward anatomical reduction. The modified Dunn procedure, utilizing surgical hip dislocation and an extended retinacular soft tissue flap as popularized by Ganz and Leunig, has emerged as the premier technique for true anatomical restoration. This highly complex procedure permits direct visualization of the physis, evacuation of the intraarticular hematoma, and meticulous debridement of the metaphyseal callus, all while preserving the tenuous vascular supply to the epiphysis.
Surgical Anatomy and Biomechanics
Proximal Femoral Vascularity
A profound understanding of the vascular anatomy of the proximal femur is the absolute prerequisite for executing the subcapital realignment with an extended retinacular flap. The primary blood supply to the adolescent femoral head is derived from the medial femoral circumflex artery. The deep branch of the medial femoral circumflex artery courses posterior to the obturator externus tendon and anterior to the quadratus femoris, ascending along the posterior aspect of the femoral neck.
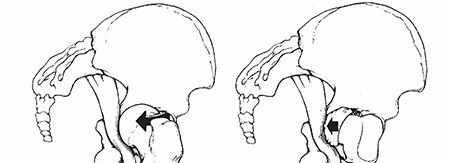
As detailed by Gautier et al, the main terminal branches of the medial femoral circumflex artery perforate the joint capsule near the superior gemellus and obturator internus insertions. These vessels travel within the synovial retinaculum along the posterosuperior and posteroinferior aspects of the femoral neck before penetrating the epiphysis. In Slipped Capital Femoral Epiphysis, the epiphysis displaces posteriorly and inferiorly relative to the metaphysis. Consequently, the anterior retinacular vessels are often ruptured, making the femoral head entirely dependent on the intact posterior retinacular vessels. The extended retinacular flap technique is specifically designed to mobilize this posterior periosteal and retinacular tissue as a continuous sleeve attached to the epiphysis, thereby preventing iatrogenic tension or transection of the medial femoral circumflex artery during reduction.
Biomechanical Considerations
The proximal femoral physis is subjected to complex shear and compressive forces during normal ambulation. In the setting of an unstable slip, the mechanical integrity of the perichondrial ring and the physeal cartilage is acutely compromised. The resultant deformity alters the center of rotation of the hip joint. The prominent anterior and superior metaphyseal neck abuts against the acetabular rim during flexion and internal rotation. This cam impingement not only damages the acetabular labrum and adjacent articular cartilage but also acts as a fulcrum that can further destabilize the physis or stress the posterior retinacular vessels.
Anatomical reduction via subcapital realignment restores the normal spherical congruency of the femoral head within the acetabulum. By re establishing the normal anatomical neck shaft angle and eliminating the metaphyseal step off, normal hip biomechanics are restored, and the mechanical triggers for early onset osteoarthritis are removed.
Indications and Contraindications
The decision to proceed with a subcapital realignment via a surgical dislocation approach requires careful consideration of the patient characteristics, the morphology of the slip, and the surgical expertise available. This is a technically demanding procedure with a steep learning curve, and inappropriate patient selection or technical errors can lead to catastrophic outcomes, most notably iatrogenic avascular necrosis.
Patient Selection Criteria
The primary indication for the modified Dunn procedure with an extended retinacular flap is an unstable Slipped Capital Femoral Epiphysis where the degree of displacement precludes safe and functional in situ pinning. It is also indicated in severe stable slips (typically defined as a slip angle greater than sixty degrees) where the residual cam deformity would result in severe, immediate femoroacetabular impingement and restricted range of motion.
Contraindications include established avascular necrosis prior to surgical intervention, active joint infection, and severe systemic comorbidities that preclude prolonged anesthesia. Relative contraindications encompass moderate stable slips where in situ pinning combined with a later arthroscopic osteochondroplasty may offer a lower risk profile, and situations where the surgical team lacks the requisite training in surgical hip dislocation techniques.
| Parameter | Operative Subcapital Realignment | Non Operative or Alternative Management |
|---|---|---|
| Slip Stability | Unstable slips | Mild to moderate stable slips |
| Slip Severity | Severe displacement (>60 degrees) | Mild displacement (<30 degrees) |
| Impingement | Severe obligate anterior impingement | Minimal or correctable via arthroscopy |
| Vascular Status | Viable head on pre operative MRI | Established AVN (requires salvage procedure) |
| Surgical Expertise | Fellowship trained in hip preservation | General orthopedic trauma coverage |
Pre Operative Planning and Patient Positioning
Imaging Modalities
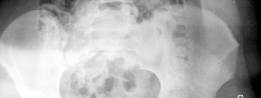
Comprehensive radiographic evaluation is mandatory. Standard imaging includes an anteroposterior view of the pelvis and a cross table lateral view of the affected hip. The frog leg lateral view is strictly contraindicated in unstable slips due to the risk of exacerbating the displacement and causing iatrogenic vascular injury.
Advanced imaging is heavily relied upon in contemporary practice. Magnetic Resonance Imaging is utilized to assess the pre operative perfusion status of the femoral head. T1 weighted and short tau inversion recovery sequences, often supplemented with gadolinium contrast, can identify pre existing ischemia. A pre operative diagnosis of avascular necrosis fundamentally alters the surgical discussion and prognosis. Computed Tomography with three dimensional reconstruction is occasionally utilized to quantify the exact degree of retroversion and the volume of the metaphyseal step off, aiding in the spatial conceptualization of the required osteotomy.

Patient Positioning and Setup
The patient is placed in the lateral decubitus position on a standard radiolucent operating table. Meticulous padding of all bony prominences, particularly the dependent axilla and the common peroneal nerve, is essential. The pelvis is rigidly secured using anterior and posterior supports to prevent rolling during the procedure, which is critical for maintaining accurate anatomical orientation during the surgical dislocation and subsequent reduction.
The entire affected lower extremity is prepped and draped free to allow for unrestricted manipulation. The ability to freely flex, extend, abduct, adduct, and rotate the hip is a fundamental requirement for the surgical dislocation approach. Intraoperative fluoroscopy is positioned to allow for orthogonal views of the proximal femur and acetabulum without compromising the sterile field. The fluoroscopic monitor should be positioned in the surgeon direct line of sight.
Detailed Surgical Approach and Technique
The surgical execution of the subcapital realignment with an extended retinacular flap is a multi stage, highly choreographed procedure. It combines the principles of surgical hip dislocation with meticulous soft tissue handling to preserve the medial femoral circumflex artery.
The Incision and Superficial Dissection
A straight lateral incision is made centered over the greater trochanter, extending proximally toward the posterior superior iliac spine and distally along the femoral shaft. The fascia lata is incised in line with the skin incision. Proximally, the gluteus maximus is split bluntly in line with its fibers. The Gibson interval, located between the anterior border of the gluteus maximus and the posterior border of the gluteus medius, is developed to expose the greater trochanter and the short external rotators.
Trochanteric Flip Osteotomy
To access the joint without damaging the abductor musculature or the medial femoral circumflex artery, a trochanteric flip osteotomy (digastric osteotomy) is performed. The osteotomy is initiated at the posterior border of the greater trochanter, just anterior to the insertion of the piriformis tendon. It exits distally at the vastus ridge. The thickness of the trochanteric fragment is typically 1.5 centimeters. The gluteus medius and minimus remain attached proximally, and the vastus lateralis remains attached distally. The osteotomized trochanter is then mobilized anteriorly, exposing the superior and anterior hip capsule.
Capsulotomy and Surgical Dislocation
A Z shaped capsulotomy is meticulously performed. The longitudinal limb of the capsulotomy is placed along the anterosuperior axis of the femoral neck. The proximal transverse limb runs parallel to the acetabular rim, and the distal transverse limb runs parallel to the intertrochanteric line. This specific configuration protects the main branches of the medial femoral circumflex artery, which course posterosuperiorly.
Following the capsulotomy, the hip is surgically dislocated by applying flexion, adduction, and external rotation to the leg. The ligamentum teres is sharply transected using specialized curved scissors. Dislocation allows for a complete 360 degree inspection of the femoral head and the acetabulum. The intraarticular hematoma is evacuated, and any labral pathology can be addressed at this stage.

Development of the Extended Retinacular Flap
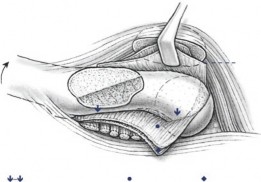
This is the most critical and technically demanding step of the procedure. The goal is to separate the posterior periosteum and the retinaculum (containing the medial femoral circumflex artery) from the femoral neck, allowing the epiphysis to be mobilized independently of the metaphysis without placing tension on the vascular pedicle.
The external rotators (piriformis, obturator internus, and gemelli) are identified. The piriformis is released from its insertion. The obturator internus and gemelli are released, taking care to protect the underlying deep branch of the medial femoral circumflex artery. An incision is made in the periosteum along the anterior intertrochanteric line. Using a combination of sharp dissection and specialized curved periosteal elevators, the periosteum is elevated off the anterior, inferior, and posterior aspects of the femoral neck. The dissection proceeds proximally toward the physis. The flap must be elevated in a full thickness manner to ensure the delicate retinacular vessels are not disrupted. The posterior flap, containing the critical blood supply, is carefully protected.
Metaphyseal Debridement and Subcapital Osteotomy
Once the extended retinacular flap has been fully mobilized, attention is directed to the physis. In an unstable slip, the epiphysis is often grossly mobile. The remaining physeal tissue on both the epiphyseal and metaphyseal sides is meticulously debrided using curettes.
The prominent anterior and superior metaphyseal bone, which constitutes the cam lesion, is resected using a high speed burr or osteotomes. This bone removal is essential for two reasons. First, it shortens the femoral neck, which is necessary to allow for the reduction of the epiphysis without placing tension on the shortened posterior retinacular vessels. Second, it eliminates the mechanical source of anterior impingement. The metaphyseal bed is contoured to match the concavity of the epiphyseal base.
Anatomical Reduction and Fixation
With the metaphysis appropriately shortened and contoured, the epiphysis is reduced onto the femoral neck. The reduction is achieved by gently manipulating the epiphysis while the leg is held in neutral rotation and slight traction. The extended retinacular flap must remain lax throughout the reduction maneuver. Any tension on the flap indicates insufficient metaphyseal shortening and requires further bone resection.
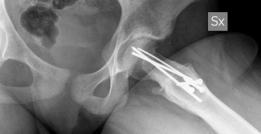
Once anatomical reduction is confirmed visually and fluoroscopically, temporary fixation is achieved with smooth Kirschner wires. Definitive fixation is typically accomplished using two or three fully threaded cannulated screws or specialized physeal implants. Fully threaded screws are preferred as they prevent compression across the osteotomy site, which could inadvertently tension the retinacular vessels. The screws must not penetrate the articular surface.
Closure
The hip is reduced back into the acetabulum. The capsulotomy is loosely closed to prevent postoperative joint tamponade, which could compromise epiphyseal perfusion. The trochanteric flip osteotomy is reduced and fixed using two or three cortical screws or a specialized trochanteric cable plate system. The fascial layers, subcutaneous tissue, and skin are closed in a standard layered fashion.
Complications and Management
The subcapital realignment procedure is associated with a distinct profile of potential complications. Vigorous preoperative counseling and meticulous surgical technique are required to minimize these risks.
Avascular Necrosis
Avascular necrosis of the femoral head is the most devastating complication following the treatment of unstable Slipped Capital Femoral Epiphysis. While the extended retinacular flap technique is designed specifically to preserve blood supply, iatrogenic injury to the medial femoral circumflex artery can occur during flap elevation, or the vessels may be tensioned if the metaphysis is inadequately shortened. Furthermore, the vascular insult may have occurred at the time of the initial slip, rendering the surgical technique moot. Management of avascular necrosis depends on the extent of head involvement and the age of the patient, ranging from core decompression and bisphosphonate therapy in early stages to total hip arthroplasty in cases of severe collapse.
Chondrolysis
Chondrolysis, the rapid and progressive loss of articular cartilage, is another severe complication. It is characterized by severe joint stiffness, pain, and joint space narrowing on radiographs. The etiology is multifactorial, potentially related to unrecognized intraarticular hardware penetration, autoimmune responses, or prolonged joint tamponade. Management includes aggressive physical therapy, nonsteroidal anti inflammatory drugs, and hardware removal if penetration is suspected. Severe cases often result in spontaneous ankylosis or require arthrodesis or arthroplasty.
Trochanteric Non Union and Hardware Failure
Non union or migration of the greater trochanter following the digastric osteotomy can lead to persistent abductor weakness and a Trendelenburg gait. This is often related to inadequate fixation or premature weight bearing. Treatment requires revision internal fixation, often supplemented with bone grafting. Loss of epiphyseal reduction or hardware failure at the subcapital osteotomy site is rare with modern fully threaded implants but necessitates immediate revision surgery.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategies |
|---|---|---|---|
| Avascular Necrosis | 5% to 15% | Vascular injury at injury or iatrogenic tension | Core decompression, osteotomy, THA |
| Chondrolysis | 2% to 7% | Unrecognized hardware penetration, autoimmune | Hardware removal, aggressive ROM, THA |
| Trochanteric Non Union | 3% to 5% | Inadequate fixation, early weight bearing | Revision ORIF with bone grafting |
| Heterotopic Ossification | 10% to 20% | Extensive surgical dissection | Indomethacin prophylaxis, surgical excision |
| Infection | < 2% | Standard surgical risks | I&D, appropriate intravenous antibiotics |

Post Operative Rehabilitation Protocols
The postoperative rehabilitation following a modified Dunn procedure must strike a delicate balance between protecting the osteotomy sites and promoting joint mobility to prevent stiffness and chondrolysis.
Immediate Post Operative Phase (Weeks 0 to 6)
Strict adherence to weight bearing restrictions is mandatory. Patients are typically restricted to toe touch weight bearing or non weight bearing on the operative extremity for a minimum of six to eight weeks. This protects both the subcapital epiphyseal fixation and the trochanteric osteotomy.
Continuous Passive Motion machines are frequently utilized immediately postoperatively to encourage synovial fluid circulation and prevent intraarticular adhesions. Active assisted range of motion exercises are initiated early, focusing on flexion, extension, and gentle abduction. Active abduction is strictly prohibited to prevent displacement of the trochanteric osteotomy.
Intermediate Phase (Weeks 6 to 12)
At the six to eight week mark, clinical and radiographic evaluation is performed. If there is evidence of early consolidation at the trochanteric osteotomy site and maintenance of the epiphyseal reduction, weight bearing is gradually progressed. Patients transition from crutches to a cane and eventually to unassisted ambulation.
Physical therapy during this phase focuses on restoring abductor strength, normalizing gait mechanics, and maximizing active range of motion. Aquatic therapy can be highly beneficial during this transition period.
Late Phase and Return to Activity (Months 3 to 12)
Full weight bearing and progressive resistance training are implemented. Return to high impact sports or vigorous physical activity is generally delayed until complete radiographic union of both the physis and the trochanteric osteotomy is confirmed, typically around six to nine months postoperatively.
Routine hardware removal is not universally recommended. However, if the patient experiences symptomatic hardware prominence over the greater trochanter, or if there is a desire to remove the subcapital screws to facilitate future imaging or interventions, removal can be considered after complete physeal fusion has occurred.
Summary of Key Literature and Guidelines
The evolution of the surgical management of unstable Slipped Capital Femoral Epiphysis is heavily documented in recent orthopedic literature. The shift from in situ pinning to open anatomical reduction was catalyzed by the pioneering work of Ganz and colleagues.
In 2001, Ganz et al. published the landmark paper describing the technique of surgical hip dislocation, demonstrating that the hip could be safely dislocated without compromising the medial femoral circumflex artery if the vascular anatomy was strictly respected. This foundational work paved the way for the application of this approach to complex intraarticular pathology.
Subsequently, Leunig et al. (2007) detailed the modified Dunn procedure utilizing the extended retinacular flap specifically for severe Slipped Capital Femoral Epiphysis. Their initial cohort demonstrated excellent clinical outcomes, restoration of normal hip anatomy, and a remarkably low rate of avascular necrosis compared to historical controls treated with closed reduction or in situ pinning.
More recent multicenter studies, such as those conducted by Sankar and the ANCHOR (Academic Network of Conservational Hip Outcomes Research) group, have critically evaluated the reproducibility of the modified Dunn procedure. These studies have confirmed that while the technique offers superior anatomical restoration and eliminates cam impingement, the risk of avascular necrosis remains non zero and is highly dependent on surgical volume and expertise. The literature consistently emphasizes the steep learning curve associated with the extended retinacular flap technique.
Current academic consensus suggests that for unstable Slipped Capital Femoral Epiphysis, anatomical reduction via a surgical dislocation approach represents the gold standard for preserving the long term viability and function of the hip joint, provided the procedure is performed by a surgeon with specialized training in advanced hip preservation techniques. In the absence of such expertise, stabilization in situ or transfer to a tertiary care center remains the most prudent course of action to avoid catastrophic iatrogenic complications.