Anterior Approach to the Clavicle: Comprehensive Surgical Anatomy & Techniques
Key Takeaway
The anterior approach to the clavicle offers extensive exposure for treating fractures, reconstructing SCJ/ACJ dislocations, excising tumors, or correcting nonunions. Critical considerations involve meticulous understanding of the S-shaped bone's biomechanics, muscle attachments, and proximity to vital neurovascular structures like the subclavian vessels and brachial plexus, essential for safe and effective surgical outcomes.
Mastering the Anterior Approach to the Clavicle: A Surgical Guide
Introduction & Epidemiology
The clavicle, a critical bony strut connecting the axial skeleton to the upper extremity, plays an essential role in shoulder girdle mechanics, providing support for the scapula, facilitating range of motion, and protecting underlying neurovascular structures. Fractures of the clavicle are among the most common orthopedic injuries, accounting for approximately 2.6% of all fractures and up to 45% of all shoulder girdle fractures. The vast majority (80%) occur in the midshaft, with lateral (15%) and medial (5%) clavicle fractures being less common. Common mechanisms include direct trauma, falls onto the outstretched hand, or a direct blow to the shoulder. While many clavicle fractures can be managed non-operatively, a significant subset benefits from surgical intervention.
The anterior approach to the clavicle provides comprehensive exposure of the entire bone, facilitating various surgical procedures. This versatile approach is fundamental for:
- Open reduction and internal fixation of fractures, particularly those with significant displacement, shortening, comminution, or neurovascular compromise.
- Reconstruction of the sternoclavicular (SCJ) and acromioclavicular (ACJ) joints in cases of dislocation or subluxation, especially higher-grade injuries or instability.
- Drainage of sepsis originating from the clavicle or adjacent soft tissues.
- Biopsy and excision of tumors affecting the clavicle.
- Osteotomy for the correction of malunion or the treatment of symptomatic nonunion.
Beyond these primary indications, the anterior approach, when combined with a clavicular osteotomy, can offer a gateway to deeper structures such as the brachial plexus and subclavian vessels. Meticulous control of superficial bleeding, particularly from subcutaneous vessels and branches of the platysma muscle, is paramount for adequate visualization, given the proximity of vital neurovascular structures immediately posterior and inferior to the clavicle.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy and biomechanics is critical for safe and effective surgery via the anterior clavicular approach.
Clavicular Morphology and Articulations
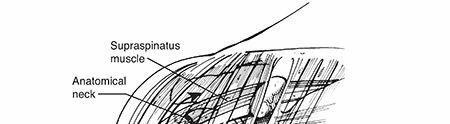
The clavicle is an S-shaped long bone, with a medially convex and laterally concave curvature. Its medial two-thirds are roughly cylindrical, while the lateral third is flattened. The bone serves as a bony strut, maintaining the scapula at a constant distance from the thorax and acting as a pivot for upper extremity motion.
- Sternal End: Articulates with the manubrium to form the sternoclavicular joint (SCJ), a saddle-type synovial joint stabilized by a strong capsule, the articular disc, and robust extrinsic ligaments: the anterior and posterior sternoclavicular ligaments, the interclavicular ligament, and the costoclavicular ligament (rhomboid ligament). The posterior SCJ ligament is particularly significant as it separates the joint from major mediastinal structures.
- Acromial End: Articulates with the acromion to form the acromioclavicular joint (ACJ), a plane synovial joint. This joint is stabilized by its capsule and ligaments, primarily the superior and inferior AC ligaments, and crucially, by the coracoclavicular (CC) ligaments (conoid and trapezoid ligaments). The conoid ligament, more medial and conical, resists posterior translation and superior displacement. The trapezoid ligament, more lateral and flat, resists horizontal displacement.
- Shaft: The thinnest and most common site of fracture, typically at the junction of the middle and lateral thirds. The superior surface is relatively smooth, while the inferior surface features the subclavian groove for the subclavius muscle and the attachment points for the costoclavicular and coracoclavicular ligaments.
Muscular Attachments
The clavicle provides origin or insertion for several muscles, whose actions contribute to fracture displacement patterns:
- Superior: Trapezius (lateral third) and Sternocleidomastoid (SCM, medial third). The SCM tends to pull the medial fragment superiorly.
- Inferior/Anterior: Pectoralis Major (medial half of anterior surface) and Deltoid (lateral third of anterior surface). The pectoralis major pulls the medial fragment inferiorly, while the deltoid pulls the lateral fragment inferiorly and anteriorly.
- Inferior: Subclavius muscle (subclavian groove).
Neurovascular Structures
The proximity of vital neurovascular structures is the most significant concern during the anterior approach. Meticulous surgical technique is paramount to avoid iatrogenic injury.
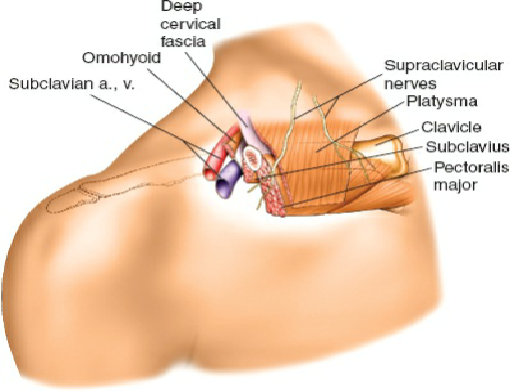
- Superior: The supraclavicular nerves (branches of the cervical plexus) cross superficial to the clavicle, providing sensation to the skin over the shoulder and upper chest. They are often encountered and may be sacrificed or retracted during the approach, potentially leading to a localized area of paresthesia or anesthesia postoperatively. The platysma muscle lies immediately deep to the skin and subcutaneous fat.
-
Posterior and Inferior:
This region harbors the most critical structures:
- Subclavian Artery and Vein: The subclavian vein lies anterior and inferior to the artery. Both pass posterior to the clavicle and subclavius muscle.
- Brachial Plexus: The trunks and divisions of the brachial plexus pass posterior to the subclavian artery.
- Pleura and Apex of the Lung: Especially relevant for medial clavicle pathology, as the apex of the lung can extend superiorly to the level of the clavicle, increasing the risk of pneumothorax.
- Internal Jugular Vein: Lies medial and posterior to the sternal head of the SCM.
- Vagus Nerve and Phrenic Nerve: The phrenic nerve lies on the anterior surface of the anterior scalene muscle, deep to the clavicle.
- Thyrocervical Trunk and its branches (e.g., suprascapular artery): May be encountered.
- Medial: The great vessels of the neck and mediastinum are in close proximity to the SCJ, particularly with posterior SCJ dislocations.
Biomechanics
The clavicle functions as a compression strut, transmitting forces from the upper extremity to the axial skeleton. Its S-shape provides elasticity and resistance to bending forces. Fractures disrupt this strut function, leading to shoulder dysfunction, pain, and potential neurovascular compromise. The forces acting on fracture fragments (muscle pull, gravity, limb weight) dictate the displacement patterns seen clinically and necessitate robust fixation to restore anatomical alignment and function. Nonunion, particularly of midshaft fractures, is often attributed to inadequate stability, biological factors, or excessive stripping of periosteal blood supply.
Indications & Contraindications
Operative Indications
The decision for operative intervention is based on fracture characteristics, patient factors, and functional demands. The anterior approach is the workhorse for most operative indications involving the clavicle.
-
Midshaft Clavicle Fractures:
- Significant shortening (>1.5-2 cm)
- Significant displacement (>100% cortical apposition, particularly superiorly displaced)
- Severe comminution (Z-type fractures, butterfly fragments)
- Open fractures (Gustilo-Anderson classification)
- Neurovascular compromise (rare, but absolute indication)
- Impending skin compromise (tenting)
- Associated injuries: Ipsilateral floating shoulder (scapula neck/glenoid fracture), polytrauma, ipsilateral upper extremity injuries requiring early mobilization.
- Symptomatic nonunion or malunion.
- Patient demand for early return to high-demand activities (e.g., athletes) where non-operative outcomes may be inferior.
-
Lateral Clavicle Fractures (Neer Type II, III, V):
- Neer Type II: Displaced fractures medial to the coracoclavicular ligaments.
- Neer Type III: Acromioclavicular joint involvement with significant displacement.
- Neer Type V: Comminution of the inferior cortex with displaced superior fragment.
- Symptomatic nonunion or malunion.
-
Medial Clavicle Fractures/Dislocations:
- Posterior sternoclavicular joint dislocations (urgent reduction due to mediastinal compression risk).
- Displaced intra-articular fractures.
- Symptomatic anterior sternoclavicular joint instability.
- Open fractures.
-
Other Indications:
- Clavicular tumors (biopsy, excision).
- Infection (drainage, debridement).
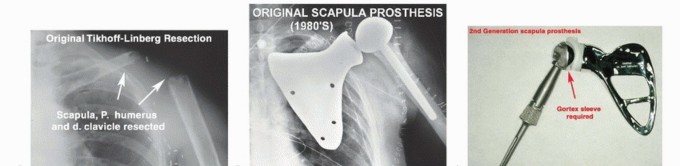
- Access to deep structures (e.g., brachial plexus decompression, subclavian vessel repair) via planned clavicular osteotomy, as mentioned in the seed content: "The brachial plexus and subacromial vessels can also be approached via this surgical approach. To do this an osteotomy of the clavicle is required." This is a highly specialized indication and typically involves temporary or permanent clavicular resection.
Relative and Absolute Contraindications
-
Absolute Contraindications:
- Active infection in the surgical field (unless the surgery is for infection control).
- Severe soft tissue compromise (e.g., devitalized skin, severe burns, impending skin necrosis) precluding safe wound closure.
- Patient deemed medically unfit for surgery (e.g., unstable polytrauma, severe comorbidities).
-
Relative Contraindications:
- Non-displaced or minimally displaced fractures without significant shortening.
- Patient non-compliance with post-operative rehabilitation.
- Severe osteoporosis where hardware fixation may be tenuous (consider alternative fixation or non-operative management if possible).
- Young, skeletally immature patients (consider non-operative management first due to excellent remodeling potential).
Operative vs. Non-Operative Indications Summary
| Indication Type | Operative | Non-Operative |
|---|---|---|
| Midshaft Fractures | Shortening >1.5-2 cm, >100% displacement, comminution, open fracture, neurovascular compromise, impending skin compromise, floating shoulder, symptomatic nonunion/malunion, patient demand for early function. | Minimally displaced fractures (<100%), shortening <1.5 cm, stable pattern, non-smoker, elderly low-demand patient without other operative indications, pediatric fractures (excellent remodeling potential). |
| Lateral Fractures | Neer Type II, III (displaced/unstable), Type V (comminuted inferior cortex), symptomatic nonunion/malunion. | Neer Type I (stable, nondisplaced), Type III (stable, non-displaced, minimal symptoms, often controversial and based on patient factors). |
| Medial Fractures | Posterior SCJ dislocation (urgent), displaced intra-articular fracture, symptomatic anterior SCJ instability, open fracture, neurovascular compromise. | Anterior SCJ subluxation/dislocation (often stable), minimally displaced fractures, conservative trial for asymptomatic instability. |
| Other Clavicle Pathologies | Clavicular tumors (biopsy, excision), infection (drainage, debridement), severe pain from malunion, specialized access to deep structures (with osteotomy). | Asymptomatic malunion, stable post-traumatic arthritis without significant functional deficit, self-limiting inflammatory conditions. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical to ensure a safe and efficient surgical procedure.
Pre-Operative Evaluation
- History: Detailed account of the mechanism of injury, associated symptoms (pain, paresthesia, weakness), handedness, prior medical history, comorbidities (diabetes, smoking, osteoporosis), and medications (anticoagulants).
-
Physical Examination:
- Inspection: Skin integrity (open wounds, tenting, ecchymosis), swelling, deformity.
- Palpation: Tenderness, crepitus, evaluation of SCJ and ACJ.
- Neurovascular Assessment: Meticulous evaluation of brachial plexus function (motor and sensory), radial, ulnar, and median nerve integrity. Palpation of distal pulses (radial, ulnar, brachial), capillary refill, and comparison to the contralateral limb. Any deficit warrants immediate investigation.
- Associated Injuries: Evaluate for ipsilateral scapula, rib, cervical spine, or lung injuries.
-
Imaging:
- Standard Radiographs: AP view of the clavicle, 30-degree cephalic tilt view (serendipity view) to assess superior/inferior displacement, and possibly a 30-degree caudal tilt view for anteroposterior displacement. For SCJ injuries, a bilateral serendipity view is essential for comparison.
- Computed Tomography (CT) Scan: Indicated for comminuted fractures, intra-articular extension (SCJ or ACJ), precise measurement of shortening or displacement, and especially crucial for evaluating posterior SCJ dislocations and their relationship to mediastinal structures.
- Magnetic Resonance Imaging (MRI): Useful for assessing associated soft tissue injuries (ligamentous damage in ACJ/SCJ injuries), evaluating nonunion with underlying biology, or characterizing soft tissue tumors.
- Angiography: If vascular injury is suspected.
Pre-operative Planning Steps
- Determine Surgical Strategy: Select appropriate plate type (superior vs. anteroinferior, locking vs. non-locking, contour), plate length, and screw types based on fracture morphology and bone quality.
- Contour Plates: Pre-contouring plates using contralateral radiographs or anatomical models can save significant intraoperative time and improve fit, especially for highly contoured plates like those for the lateral clavicle.
- Anesthesia: General anesthesia is standard. Regional anesthesia (e.g., interscalene block) can be a valuable adjunct for post-operative pain control, but care must be taken to avoid masking subtle neurovascular changes post-operatively.
- Antibiotics: Prophylactic antibiotics (e.g., Cefazolin) administered pre-incision.
Patient Positioning
The patient's position is critical for optimal exposure and safe execution of the anterior approach.
- Supine Position: The patient is placed supine on the operating table.
-
Shoulder Elevation:
The original seed content describes, "Break the table and elevate the head end, so as to elevate the shoulder area. Place a sandbag between the medial border of the scapula and the spine. This will allow the shoulder to drop back and often this maneuver reduces fractu-"
- Completing this thought: This maneuver accomplishes several key objectives: it effectively elevates the surgical field, allowing the shoulder to fall posteriorly and inferiorly, which often indirectly reduces fracture displacement, particularly shortening. This also places the neurovascular structures further away from the posterior aspect of the clavicle, increasing the working space and safety margin.
- Alternatively, a small rolled towel or commercially available shoulder bump can be placed longitudinally between the scapulae.
- Arm Draping: The ipsilateral arm should be draped free or across the chest to allow for intraoperative manipulation for reduction maneuvers and assessment of range of motion.
- C-arm Access: Ensure unrestricted access for intraoperative fluoroscopy, typically a C-arm, to confirm reduction and hardware placement. The C-arm monitor should be positioned in the surgeon's direct line of sight.
- Preparation and Draping: The surgical field should be prepped widely, extending from the base of the neck, across the shoulder, and down to the nipple line, to allow for extension of the incision if necessary and to facilitate draping. Sterile draping is performed to isolate the surgical area.
- Tourniquet: Generally not used for clavicle surgery due to the lack of sufficient soft tissue to apply a tourniquet and the risk of neurovascular compression in the neck/shoulder region. Meticulous hemostasis is achieved with electrocautery and ligatures.
Detailed Surgical Approach / Technique
The anterior approach to the clavicle requires meticulous dissection and a structured approach to minimize complications and optimize outcomes.
Incision
The choice of incision depends on the fracture location, extent of pathology, and surgeon preference.
-
Midshaft Fractures:
- Transverse/Oblique (Langer's lines): This is generally preferred for cosmetic reasons. An incision approximately 1-2 cm inferior to and parallel to the clavicle, centered over the fracture site, can be utilized. This provides good exposure while minimizing tension on the wound.
- Direct Longitudinal: For extensive exposure (e.g., comminuted fractures, nonunion requiring extensive debridement and grafting, or tumor excision), a direct longitudinal incision along the superior border of the clavicle may be necessary. While less cosmetic, it offers maximal access.
-
Lateral Clavicle Fractures/ACJ Injuries:
- A slightly oblique incision extending from the anterior aspect of the clavicle laterally over the ACJ.
-
Medial Clavicle Fractures/SCJ Injuries:
- A transverse incision over the medial clavicle and SCJ. Careful curvilinear extension along the SCM border may be needed for broader exposure, always respecting the great vessels.
The length of the incision should be adequate to allow for full visualization of the fracture fragments and insertion of fixation devices without excessive retraction, which can devitalize soft tissues.
Dissection
-
Skin and Subcutaneous Tissue:
Incise the skin and subcutaneous tissue. Identify and coagulate or ligate any superficial bleeders.
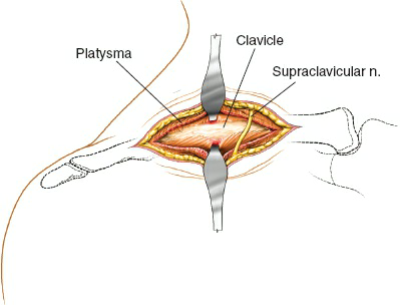
- As highlighted in the seed content: "Bleeding from subcutaneous vessels and vessels in the platysma muscle is very common. Because of the proximity of great vessels, such superficial bleeding must be controlled to ensure adequate visualization of the structures (see Fig. 1-1)."
-
 - Take care to identify and protect the supraclavicular nerves, which typically cross superficial to the clavicle. While often unavoidable, careful retraction or sharp dissection can minimize nerve damage.
- Platysma Muscle: The platysma muscle, if present in the region, is encountered deep to the subcutaneous fat. It should be sharply incised in line with the skin incision or retracted. Meticulous hemostasis is maintained.
- Deep Fascia: Incise the deep fascia overlying the clavicle.
-
Subperiosteal Dissection:
This is a crucial step.
- Anterior and Superior: Elevate the periosteum and muscle attachments (deltoid, pectoralis major, SCM, trapezius) just enough to expose the fracture fragments. The goal is to preserve as much periosteal blood supply as possible, especially on the inferior aspect.
- Inferior: Extreme caution is mandatory. Limit inferior periosteal stripping as much as possible to protect the underlying subclavian artery, vein, and brachial plexus. A small Hohmann retractor can be carefully placed subperiosteally along the inferior border of the clavicle to protect these vital structures during drilling and screw insertion. This retractor should always hug the bone and never be inserted blindly or excessively deep.
- In cases of nonunion or severe comminution, scar tissue may be encountered. This should be carefully debrided to expose viable bone ends.
Fracture Reduction
The goal is to restore anatomical length, alignment, and rotation of the clavicle.
- Visualization: Directly visualize the fracture fragments. Debride any hematoma or interposed soft tissue.
-
Reduction Maneuvers:
- Manual Traction: Longitudinal traction on the arm, often combined with manipulation of the shoulder, can help restore length.
- Reduction Forceps: Pointed reduction clamps (e.g., Weber, Verbrugge, mini-fragment clamps) are invaluable for holding fragments in reduction. Joystick techniques with K-wires inserted into fragments can aid in manipulation.
- Bone Hooks/Periosteal Elevators: Can be used to lever fragments into position.
- Restore Length: Key for function. Ensure the reduction is stable enough to allow for plate application.
- Rotation: Important, especially for midshaft fractures. Compare the orientation of the ends of the fracture fragments to the intact contralateral clavicle, or ensure the superior surface maintains its normal gentle curve.
- Coracoclavicular Ligament Repair/Reconstruction: For lateral clavicle fractures (Neer Type II, III, V) or ACJ dislocations, concomitant repair or reconstruction of the CC ligaments (e.g., with suture button devices or allograft/autograft) may be necessary to maintain reduction and stability.
Fixation
Plate and screw fixation is the most common and biomechanically stable method for clavicle fractures.
-
Plate Selection:
- Anatomical Contoured Locking Plates: Modern low-profile, pre-contoured locking plates are generally preferred. These provide angular stability and minimize hardware prominence.
-
Location:
- Superior Plating: Biomechanically strong, resisting bending forces effectively. However, it can be associated with higher rates of hardware prominence and irritation due to thinner soft tissue coverage.
- Anterosuperior/Anteroinferior Plating: Anteroinferior placement may be less prominent but typically biomechanically weaker for resisting bending forces unless a robust plate is used.
- Plate Length: Should allow for at least three bicortical screws (or 6 cortices) on each side of the fracture, ideally more for comminuted patterns.
- Dual Plating: For severely comminuted or highly unstable fractures, dual plating (e.g., superior and anteroinferior) may be considered to enhance construct stability.
-
Plate Application:
- After achieving provisional reduction with clamps or K-wires, apply the chosen plate.
- Secure the plate to the main fragments with screws. Start with a non-locking screw through an oval hole to draw the plate to the bone and achieve compression (lag screw principle across the fracture if possible).
- Insert subsequent locking screws according to the plate design, ensuring adequate purchase in both cortices.
- For lateral clavicle fractures, plates are often extended laterally with screws engaging the acromion, or specific lateral clavicle plates may have intramedullary prongs for distal fixation. Suture buttons are often used in conjunction with plates or as stand-alone constructs to reconstruct the coracoclavicular ligaments.
- For medial clavicle fractures or SCJ dislocations, specialized plates or K-wires (removed early to prevent migration) may be used. Ligamentous reconstruction often augments stability.
-
 - Confirm reduction and hardware placement with intraoperative fluoroscopy in multiple planes (AP, 30-degree cephalic tilt).
-
Screw Insertion (Critical Safety Point):
- During drilling, measuring, and screw insertion, the inferior aspect of the clavicle must be protected. A malleable retractor or a small Hohmann retractor under the clavicle and hugging the posterior cortex is essential to shield the subclavian vessels and brachial plexus. This retractor should be observed during drilling to ensure it remains in position.
- Avoid over-drilling or over-penetrating the posterior cortex.
- Ensure all screws achieve bicortical purchase for maximal stability unless specifically contraindicated (e.g., very short lateral fragment where unicortical locking screws may be considered if no other option).
Wound Closure
- Irrigation: Copiously irrigate the wound with sterile saline.
- Periosteal Repair: If sufficient periosteum remains, close it over the plate to provide an additional soft tissue envelope and potentially enhance healing, though this is often not possible or necessary.
- Platysma and Subcutaneous Tissue: Close the platysma muscle layer (if significant) and the subcutaneous tissue with absorbable sutures to reduce dead space and provide a strong layer for skin approximation.
- Skin Closure: Close the skin with subcuticular sutures for optimal cosmesis, followed by sterile strips or skin glue.
- Dressing: Apply a sterile, compressive dressing.
Complications & Management
Despite careful technique, complications can occur with the anterior approach to the clavicle. Awareness of potential complications and their management is crucial.
Intraoperative Complications
-
Neurovascular Injury (Brachial Plexus, Subclavian Artery/Vein, Internal Jugular Vein):
- Incidence: Rare but devastating. Estimated <1%.
- Prevention: Meticulous dissection, limited inferior periosteal stripping, constant use of a bone-hugging retractor protecting the inferior and posterior aspects of the clavicle during drilling/screw insertion. Avoid excessive depth with instruments. For medial clavicle procedures, awareness of the dome of the pleura is paramount.
- Management: Immediate recognition is key. Direct repair by the orthopedic surgeon or a vascular/thoracic surgery consult as needed. Secure hemostasis, repair vessel, or nerve.
-
Pneumothorax:
- Incidence: Rare, more common with medial clavicle fractures or deep dissection.
- Prevention: Careful dissection, especially medially. Avoid deep penetration with instruments.
- Management: Immediate chest tube insertion.
-
Excessive Bleeding:
- Incidence: Common from superficial vessels (platysma, supraclavicular arteries/veins). Major vessel injury is rare.
- Prevention: Meticulous hemostasis with electrocautery and ligatures.
- Management: Direct pressure, cautery, ligation. If from major vessels, follow neurovascular injury protocol.
-
Inadequate Reduction/Fixation:
- Incidence: Variable, depends on fracture complexity and surgeon experience.
- Prevention: Proper pre-operative planning, intraoperative fluoroscopy, appropriate choice of hardware, careful reduction maneuvers.
- Management: Intraoperative revision of reduction and/or fixation.
Early Postoperative Complications
-
Infection (Superficial or Deep):
- Incidence: 1-5%. Higher in open fractures, immunocompromised patients, or prolonged surgery.
- Prevention: Prophylactic antibiotics, meticulous aseptic technique, proper wound care.
-
Management:
- Superficial: Oral antibiotics, local wound care.
- Deep: Surgical irrigation and debridement, intravenous antibiotics, possible hardware removal if persistent or chronic, often combined with re-fixation if nonunion occurs.
-
Hematoma/Seroma:
- Incidence: Common.
- Prevention: Meticulous hemostasis, wound closure in layers.
- Management: Aspiration (sterile), compression dressing. Surgical drainage if large or symptomatic.
-
Wound Dehiscence/Necrosis:
- Incidence: Rare, but increased with excessive tension on skin, poor tissue handling, or compromised vascularity.
- Prevention: Careful skin incision planning (Langer's lines), gentle tissue handling, layered closure without tension.
- Management: Local wound care, débridement, potential need for plastic surgery consultation for flap coverage.
Late Postoperative Complications
-
Nonunion:
- Incidence: 5-15% for operatively treated fractures, but can be higher for certain fracture patterns or with specific risk factors (smoking, severe comminution, initial displacement, infection, inadequate fixation).
- Management: Revision ORIF with bone grafting (autograft from iliac crest or distal radius, or allograft), plate augmentation, or electrical stimulation. Goal is to achieve stability and promote osteogenesis.
-
Malunion:
- Incidence: Variable, many are asymptomatic. Symptomatic malunions (e.g., shortening causing impingement, pain, neurovascular symptoms) are less common but debilitating.
- Management: Corrective osteotomy and internal fixation, often with bone grafting.
-
Hardware Prominence/Irritation:
- Incidence: Very common, up to 30-50%, due to thin soft tissue coverage.
- Prevention: Use of low-profile, anatomically contoured plates.
- Management: Hardware removal, typically after radiographic and clinical evidence of complete fracture union (usually 6-12 months post-op).
-
Persistent Pain/Stiffness:
- Incidence: Can result from nerve irritation, post-traumatic arthritis, or inadequate rehabilitation.
- Management: Physical therapy, pain management, diagnostic injections, hardware removal, or rarely, arthrodesis for severe joint instability.
-
Refracture:
- Incidence: Rare after union, but can occur with severe re-trauma or premature hardware removal.
- Management: Re-operation with stronger fixation, possibly bone grafting.
-
Post-traumatic Arthritis (ACJ/SCJ):
- Incidence: Can occur following intra-articular fractures or dislocations.
- Management: Conservative management (NSAIDs, injections, PT) initially. Surgical options include distal clavicle excision (Mumford procedure) for ACJ arthritis or partial sternoclavicular joint resection for SCJ arthritis.
Complications and Management Table
| Complication | Incidence (Approximate Range) | Salvage/Management Strategies |
|---|---|---|
| Neurovascular Injury | <1% | Immediate recognition and surgical repair by orthopedic/vascular/thoracic surgeon. Hemostasis. Post-op neurological monitoring. |
| Pneumothorax | <1% | Chest tube insertion. Monitor respiratory status. |
| Infection | 1-5% | Superficial: Oral antibiotics, wound care. Deep: Surgical irrigation & débridement, IV antibiotics, consider hardware removal (with re-fixation/grafting if nonunion). |
| Nonunion | 5-15% | Revision ORIF with bone grafting (autograft/allograft), plate augmentation, electrical stimulation. Address contributing factors (smoking cessation). |
| Malunion | Variable | Asymptomatic: Observation. Symptomatic: Corrective osteotomy and internal fixation, often with bone grafting. |
| Hardware Prominence/Irritation | 30-50% | Hardware removal (after radiographic union, typically 6-12 months post-op). |
| Persistent Pain/Stiffness | Variable | Physical therapy, pain management modalities, diagnostic injections. Consider hardware removal. Address underlying causes (e.g., nerve irritation, post-traumatic arthritis). |
| Refracture | Rare | Re-operation with more robust fixation (e.g., longer plate, dual plating), consider bone grafting. Ensure complete union before considering hardware removal. |
| Wound Dehiscence/Necrosis | Rare | Local wound care, débridement. May require plastic surgery consultation for flap coverage. |
| Hematoma/Seroma | Common | Aspiration (sterile), compression. Surgical drainage if large, tense, or infected. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring function, preventing stiffness, and ensuring optimal outcomes following clavicle fixation. Protocols are typically progressive and individualized based on fracture stability, fixation strength, and patient factors.
Phase I: Protection and Early Motion (Weeks 0-6)
- Immobilization: Sling use for comfort and protection. Duration typically 2-6 weeks depending on the stability of fixation, fracture type, and surgeon preference. Patients are generally advised to keep the arm in the sling except for hygiene and specific exercises.
- Pain Management: Opioids, NSAIDs, and muscle relaxants as needed. Regional anesthesia (interscalene block) can be beneficial for the first 24-48 hours.
-
Early Active Range of Motion (ROM):
- Hand, wrist, and elbow ROM exercises encouraged immediately to prevent stiffness and promote circulation.
- Gentle pendulum exercises (Codman's) for the shoulder, allowing gravity to assist motion without active muscle contraction.
- Scapular stabilization exercises (e.g., gentle scapular retraction/protraction) within pain limits.
-
Restrictions:
- No active shoulder abduction or flexion beyond 45-60 degrees.
- No lifting, pushing, or pulling with the affected arm.
- Avoid external rotation beyond neutral.
- No weight-bearing on the affected arm.
- No overhead activities.
- Wound Care: Maintain a clean, dry dressing. Monitor for signs of infection. Suture removal (if non-absorbable) at 10-14 days.
Phase II: Progressive Range of Motion and Light Strengthening (Weeks 6-12)
- Radiographic Assessment: Obtain follow-up radiographs to assess early callus formation and stability of fixation. Once initial healing is evident, progression can be more aggressive.
- Discontinue Sling: Typically around 6 weeks, or as pain dictates and radiographic union progresses.
-
Active-Assisted and Active ROM:
- Gradually increase active and active-assisted shoulder ROM in all planes (flexion, abduction, internal/external rotation).
- Focus on achieving full elevation and external rotation.
- Wall slides, pulley exercises, and cane exercises.
-
Light Strengthening:
- Begin with isometric exercises for the rotator cuff and periscapular muscles (subscapularis, supraspinatus, infraspinatus, teres minor, rhomboids, serratus anterior, trapezius).
- Light resistance with elastic bands, gradually progressing as tolerated.
-
Restrictions:
- Continue to avoid heavy lifting or high-impact activities.
- No sudden movements or unprotected falls.
Phase III: Advanced Strengthening and Functional Return (Weeks 12-24+)
- Radiographic Assessment: Confirm solid radiographic union before advancing to full-strength activities.
-
Progressive Strengthening:
- Continue progressive resistance exercises for all shoulder girdle muscles.
- Incorporate eccentric exercises and proprioceptive training.
- Begin closed-chain exercises (e.g., push-ups against a wall, progressing to floor).
-
Functional Training:
- Sport-specific or occupation-specific training and drills.
- Gradual return to overhead activities.
-
Return to Activity:
- Return to light, non-contact activities typically at 3-4 months.
- Return to heavy labor or contact sports usually at 4-6 months, provided there is full ROM, strength, and solid radiographic union without pain.
- The decision for return to sport should be individualized, with objective criteria including pain-free ROM, full strength (ideally confirmed with isokinetic testing), and psychological readiness.
Key Principles of Rehabilitation
- Pain-Limited: Exercises should be performed within the patient's pain tolerance.
- Gradual Progression: Avoid sudden increases in load or range of motion.
- Individualization: Protocols must be tailored to the patient's specific fracture pattern, fixation type, bone quality, activity level, and goals.
- Patient Education: Emphasize adherence to restrictions and the importance of consistent exercise.
- Scar Management: Begin scar massage once the wound is well-healed to prevent adhesions.
Summary of Key Literature / Guidelines
The management of clavicle fractures, particularly midshaft fractures, has evolved significantly based on accumulating evidence. The anterior approach is the cornerstone of operative management, and its indications have broadened.
-
Midshaft Clavicle Fractures:
- The landmark Canadian Orthopaedic Trauma Society (COTS) study (2007) provided strong evidence supporting operative fixation for completely displaced midshaft clavicle fractures. This randomized controlled trial demonstrated significantly improved functional outcomes (Constant and DASH scores) and lower rates of symptomatic malunion and nonunion in the operative group compared to conservative management.
- Subsequent meta-analyses and systematic reviews have generally supported these findings, advocating for operative fixation in displaced or shortened midshaft clavicle fractures. While some studies suggest no significant difference in overall functional outcome long-term for minimally displaced fractures, operative treatment offers faster return to function and lower rates of nonunion in displaced fractures.
- The choice between superior and anteroinferior plating remains a topic of debate. Biomechanical studies suggest superior plating offers greater stiffness and strength in bending and torsion. However, anteroinferior plating may reduce hardware prominence. Low-profile, anatomically contoured locking plates have become the standard for both positions, aiming to mitigate issues of prominence while providing stable fixation.
-
Lateral Clavicle Fractures:
- Operative management is generally indicated for Neer Type II and V fractures due to the disruption of the coracoclavicular ligaments, leading to instability and a high risk of nonunion with conservative management.
- Various techniques exist, including plate fixation with or without coracoclavicular ligament reconstruction (e.g., using suture button devices, allograft, or autograft). The addition of coracoclavicular stabilization to lateral clavicle plating has shown superior results in some studies, particularly for preventing loss of reduction.
- Neer Type III fractures (ACJ involvement without CC ligament disruption) remain controversial, with many treated non-operatively, especially in low-demand patients. However, operative fixation may be considered for symptomatic patients, particularly athletes or manual laborers, to restore anatomy and prevent chronic pain or dysfunction.
-
Medial Clavicle Fractures and SCJ Injuries:
- Posterior sternoclavicular dislocations are considered orthopedic emergencies due to potential compression of mediastinal structures (trachea, esophagus, great vessels). Urgent reduction, often open, is indicated.
- Surgical intervention for unstable or significantly displaced medial clavicle fractures and symptomatic anterior SCJ instability is generally recommended, often involving plate fixation or ligamentous reconstruction. Caution regarding the underlying mediastinal structures is paramount.
-
Nonunion and Malunion:
- Symptomatic nonunion of the clavicle often requires revision surgery with plate fixation and bone grafting (autograft or allograft) to achieve union. Success rates are generally high with appropriate surgical technique and grafting.
- Symptomatic malunion (e.g., significant shortening, neurovascular impingement, cosmetic deformity) may warrant corrective osteotomy and fixation.
General Guidelines and Future Directions:
Current guidelines from orthopedic societies emphasize shared decision-making with patients, considering their functional demands, comorbidities, and preferences. The trend is towards increased operative intervention for displaced clavicle fractures to minimize nonunion and improve functional outcomes. Ongoing research continues to refine plate design, optimal fixation strategies (e.g., dual plating for comminuted fractures), and the role of biological augmentation. Emphasis remains on minimizing soft tissue stripping, achieving anatomical reduction, and providing stable internal fixation while respecting the delicate neurovascular anatomy of the region.
You Might Also Like