Hemiarthroplasty for Proximal Humerus: What You Need to Know
Key Takeaway
Learn more about Hemiarthroplasty for Proximal Humerus: What You Need to Know and how to manage it. Hemiarthroplasty for proximal humerus is a surgical option for complex or severely displaced proximal humerus fractures, which account for 4-5% of all fractures. This procedure replaces the damaged articular segment of the humerus with a prosthetic implant, while preserving the shoulder's socket. It's often chosen when poor bone quality or compromised blood supply increases osteonecrosis risk, particularly in older patients.
DEFINITION
Proximal humerus fractures involve isolated or combined injuries to the greater tuberosity, lesser tuberosity, articular segment, and proximal humeral shaft. Overall, proximal humerus fractures account for 4% to 5% of all fractures. 2, 8, 11, 13 ## ANATOMY The proximal humerus consists of four segments: the greater tuberosity, lesser tuberosity, articular segment, and humeral shaft ( FIG 1). The most cephalad surface of the articular segment is, on average, 8 mm above the greater tuberosity. 18 Humeral version averages 29.8 degrees (range, 10 to 55 degrees).18, 23 The intertubercular groove lies between the tuberosities and forms the passageway for the long head of the biceps as it traverses from the intra-articular origin into the distal arm. The tuberosities attach to the articular segment at the anatomic neck. The greater tuberosity has three facets for the corresponding insertions of the supraspinatus, infraspinatus, and teres minor tendons; the lesser tuberosity has a single facet for the subscapularis. The deltoid, pectoralis major, and latissimus dorsi all insert on the humerus distal to the surgical neck. These soft tissue attachments contribute to the deforming forces sustained with proximal humerus fractures.
 ---
---
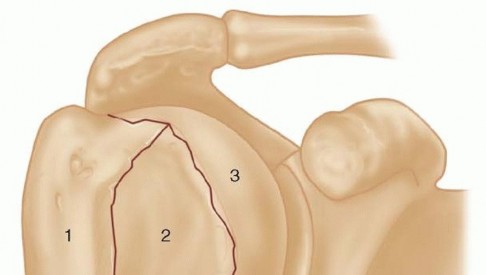
 ### FIG 1 • Neer classification of proximal humerus fractures:
1
, greater tuberosity;
2
, lesser tuberosity;
3
, articular surface;
4
, shaft. The humeral head receives its blood supply from the anterolateral branch of the anterior humeral circumflex artery (the arcuate artery of Laing) and the posterior humeral circumflex artery. The artery of Laing courses parallel to the lateral aspect of the long head of the biceps and enters the humeral head at the interface between the intertubercular groove and the greater tuberosity. 20 More recent studies have indicated that the posterior branch may play a larger role in perfusion of the fractured humeral head, reducing the risk of osteonecrosis.10, 15, 16 ## PATHOGENESIS The incidence of proximal humerus fractures is increasing with an aging population and associated osteoporosis. The mechanism of injury may be indirect or direct and secondary to high-energy collisions in younger patients (eg, motor vehicle accidents, athletic injuries) or falls from standing height in elderly patients. Pathologic fractures from primary or metastatic disease should be included in the differential diagnosis. Risk factors for the development of proximal humerus fractures in the elderly patient population include low bone density, lack of hormone replacement therapy, previous fracture history, three or more chronic illnesses,
and smoking. 17
## NATURAL HISTORY Neer's classic study in 1970 compared the results of nonoperative treatment with hemiarthroplasty for three-and fourpart displaced proximal humerus fractures. No satisfactory results were found in the nonoperative group owing to inadequate reduction, nonunion, malunion, and humeral head osteonecrosis with collapse. 22 Stableforth 28 reaffirmed this in a study in which patients were randomized to nonoperative management or prosthetic replacement. The patients with displaced fractures treated nonoperatively had worse overall results for pain, range of motion, and activities of daily living. Olerud et al 25 most recently demonstrated significantly improved quality of life with a trend toward pain scores with four-part fractures treated with hemiarthroplasty versus observation. ## PATIENT HISTORY AND PHYSICAL FINDINGS A thorough history and complete physical examination should be performed. History should include mechanism of injury, premorbid level of function, occupation, hand dominance, history of malignancy, and ability to participate in a structured rehabilitation program. 14 202
### FIG 1 • Neer classification of proximal humerus fractures:
1
, greater tuberosity;
2
, lesser tuberosity;
3
, articular surface;
4
, shaft. The humeral head receives its blood supply from the anterolateral branch of the anterior humeral circumflex artery (the arcuate artery of Laing) and the posterior humeral circumflex artery. The artery of Laing courses parallel to the lateral aspect of the long head of the biceps and enters the humeral head at the interface between the intertubercular groove and the greater tuberosity. 20 More recent studies have indicated that the posterior branch may play a larger role in perfusion of the fractured humeral head, reducing the risk of osteonecrosis.10, 15, 16 ## PATHOGENESIS The incidence of proximal humerus fractures is increasing with an aging population and associated osteoporosis. The mechanism of injury may be indirect or direct and secondary to high-energy collisions in younger patients (eg, motor vehicle accidents, athletic injuries) or falls from standing height in elderly patients. Pathologic fractures from primary or metastatic disease should be included in the differential diagnosis. Risk factors for the development of proximal humerus fractures in the elderly patient population include low bone density, lack of hormone replacement therapy, previous fracture history, three or more chronic illnesses,
and smoking. 17
## NATURAL HISTORY Neer's classic study in 1970 compared the results of nonoperative treatment with hemiarthroplasty for three-and fourpart displaced proximal humerus fractures. No satisfactory results were found in the nonoperative group owing to inadequate reduction, nonunion, malunion, and humeral head osteonecrosis with collapse. 22 Stableforth 28 reaffirmed this in a study in which patients were randomized to nonoperative management or prosthetic replacement. The patients with displaced fractures treated nonoperatively had worse overall results for pain, range of motion, and activities of daily living. Olerud et al 25 most recently demonstrated significantly improved quality of life with a trend toward pain scores with four-part fractures treated with hemiarthroplasty versus observation. ## PATIENT HISTORY AND PHYSICAL FINDINGS A thorough history and complete physical examination should be performed. History should include mechanism of injury, premorbid level of function, occupation, hand dominance, history of malignancy, and ability to participate in a structured rehabilitation program. 14 202
 ---
---
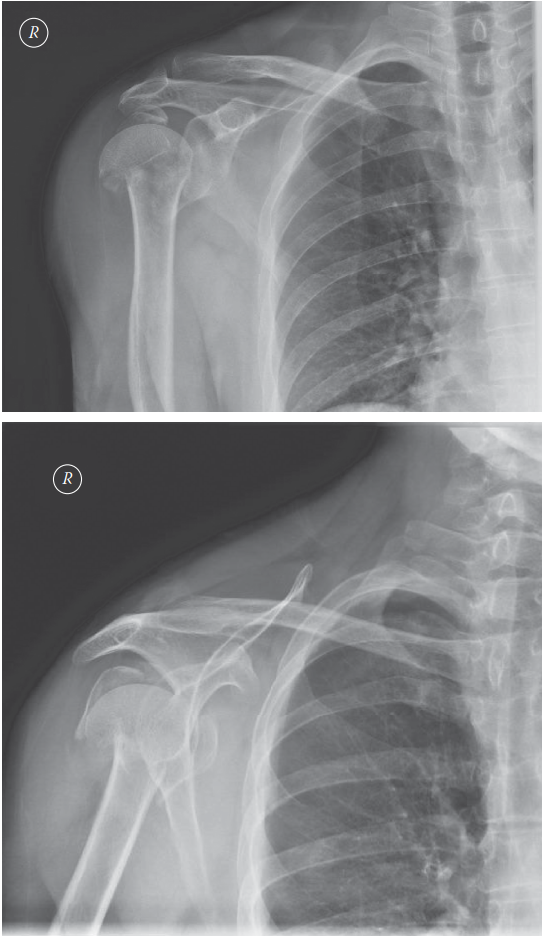
FIG 2 • A. Anteroposterior (AP) and (B) scapular “Y” views of a displaced four-part proximal humerus fracture without evidence of concomitant dislocation. (Copyright Kamal I. Bohsali, MD.) A review of systems should involve queries regarding loss of consciousness, paresthesias, and ipsilateral elbow or wrist pain. On physical examination, the orthopaedic surgeon should look for swelling, soft tissue injuries, ecchymosis, and deformity. Posterior fracture-dislocations will demonstrate flattening of the anterior aspect of the shoulder with an associated posterior prominence. Anterior fracture-dislocations present with opposite findings. 14 ## IMAGING AND OTHER DIAGNOSTIC STUDIES Appropriate radiographs include biplanar views of the shoulder 14 ( FIG 2). If the axillary view cannot be obtained because of patient discomfort, alternate views such as the Velpeau trauma axillary view can be used to evaluate and classify the glenohumeral articulation. 2 The Neer classification is based on the four anatomic segments of the proximal humerus: the humeral head, the greater and lesser tuberosities, and the humeral shaft (see FIG 1).11 Number of parts is based on 45 degrees of angulation or 1 cm of displacement from neighboring segments. The AO/ASIF/OTA Comprehensive Long Bone Classification system distinguishes the valgus impacted fourpart proximal humerus fracture from other four-part fractures with partial preservation of the vascular inflow to the articular segment through an intact medial capsule. 8, 19, 26 The current fracture classification systems have fair interobserver reliability, even with the addition of computed tomography (CT) scans. Despite the limitations of these systems, they remain clinically useful when deciding on nonoperative versus operative treatment. 2, 11 CT scans may be helpful in evaluating tuberosity displacement and articular surface involvement. 12, 14 ## DIFFERENTIAL DIAGNOSIS Acute hemorrhagic bursitis Traumatic rotator cuff tear Simple dislocation Acromioclavicular separation Calcific tendinitis 2 ## NONOPERATIVE MANAGEMENT Nonoperative treatment usually is reserved for minimally displaced fractures of the proximal humerus, which account for nearly 80% of these injuries. The characteristics of the fracture (ie, bone quality, fracture orientation, concurrent soft tissue injuries), the personality of the patient (eg, compliant, realistic expectations, mental status), and surgeon experience all affect the decision to proceed with operative intervention. Moribund individuals and patients unable to cooperate with a postoperative rehabilitation program (eg, closed head injury) are not appropriate candidates for operative intervention. In general, nonoperative management of complex, displaced proximal humerus fractures has not proven as successful. Initial immobilization with a sling and axillary pad may be helpful. Gentle range-of-motion exercises may be started by 7 to 10 days after the fracture event when pain has decreased and the patient is less apprehensive. 2 Intermittent biplanar radiographs are essential to determine additional displacement and the interval stage of healing. 2 Active and active-assisted range-of-motion exercises are initiated with evidence of radiographic union. Inform the patient that he or she may never attain symmetric range of motion or strength when comparing the affected versus the uninjured side. ## SURGICAL MANAGEMENT The goal of surgery is to anatomically reconstruct the glenohumeral joint with restoration of humeral height, replication of appropriate prosthetic retroversion, and establishment of secure tuberosity fixation. Prosthetic replacement is the preferred treatment of most four-part fractures, three-part fractures and dislocations in elderly patients with osteoporotic bone, head-splitting articular segment fractures, and chronic anterior or posterior humeral head dislocations with more than 40% of the articular surface involvement. 1, 2, 23 Several studies have indicated that the outcome of primary hemiarthroplasty for acute proximal humerus fractures is superior to that from late reconstruction. 6, 24 There are commercially available fracture-specific stems that allow for improved bone grafting and tuberosity placement, some with bone windows with reduced proximal stem diameter and others with a suture collar with potential conversion to a reverse shoulder prosthesis ( FIG 3A,B). ## Preoperative Planning Although some studies have suggested urgent intervention (ie, within <48 hours), most authors recommend preoperative planning with a careful neurovascular assessment of the injured shoulder, medical optimization of the patient, and preoperative templating with standard radiographs of the contralateral uninjured shoulder. 12 A CT scan may provide improved characterization of the fracture pattern such as intra-articular involvement and degree of tuberosity comminution for surgical planning.2 An interscalene block (regional anesthesia) may be used to supplement general anesthesia. 203
 ---
---

 ### FIG 3 • A,B. Fracture-specific stem with commercially available fracture jig allows for intraoperative trial reduction. (A: Courtesy of Depuy-Synthes, Warsaw, IN; B: Copyright Kamal I. Bohsali, MD.) Endotracheal intubation is recommended to allow for intraoperative muscle relaxation, but laryngeal mask intubation may be used. 12, 14 ## Positioning The patient is placed on an operating table in the beachchair position with the arm positioned in a sterile articulating arm holder or draped free if an appropriate number of assistants are available ( FIG 4). Intraoperative C-arm fluoroscopy is recommended and will assist the surgeon in implant placement and tuberosity positioning.
### FIG 3 • A,B. Fracture-specific stem with commercially available fracture jig allows for intraoperative trial reduction. (A: Courtesy of Depuy-Synthes, Warsaw, IN; B: Copyright Kamal I. Bohsali, MD.) Endotracheal intubation is recommended to allow for intraoperative muscle relaxation, but laryngeal mask intubation may be used. 12, 14 ## Positioning The patient is placed on an operating table in the beachchair position with the arm positioned in a sterile articulating arm holder or draped free if an appropriate number of assistants are available ( FIG 4). Intraoperative C-arm fluoroscopy is recommended and will assist the surgeon in implant placement and tuberosity positioning.
 ---
---
 ### FIG 4 • A,B. The patient is placed on an operating table in the beach-chair position, with the arm positioned in a sterile articulating arm holder or draped free with use of a padded Mayo stand. (Copyright Kamal I. Bohsali, MD.)
*
### FIG 4 • A,B. The patient is placed on an operating table in the beach-chair position, with the arm positioned in a sterile articulating arm holder or draped free with use of a padded Mayo stand. (Copyright Kamal I. Bohsali, MD.)
*
Approach The surgical prep site should include the entire upper extremity and shoulder region, including the scapular and pectoral regions. Appropriate prophylactic intravenous antibiotics are given to the patient before skin incision. A standard deltopectoral incision is used. Care is taken to minimize injury (eg, surgical detachment, contusion secondary to retractors) to the deltoid conjoint muscle. The musculocutaneous and axillary nerves are identified and protected during the procedure. ## TECHNIQUES
-
** Deltopectoral Approach The incision begins superior and medial to the coracoid process and extends toward the anterior aspect of the deltoid insertion ( TECH FIG 1A). The cephalic vein is identified, preserved, and retracted laterally with the deltoid muscle. The pectoralis major is mobilized medially. If additional exposure is necessary, the proximal 1 cm of the pectoralis major insertion is released ( TECH FIG 1B). Fracture hematoma usually is encountered once the clavipectoral fascia is incised. At this time, fracture fragments and the rotator cuff musculature become evident. The axillary and musculocutaneous nerves can be identified through digital palpation of the anteroinferior aspect of the subscapularis muscle and the posterior aspect of the coracoid muscles respectively. External rotation of the humerus results in reduced tension on the axillary nerve. 204
 ---
---
 TECH FIG 1 • Skin incision and deltopectoral approach. A. The skin incision is centered over the anterior deltoid. The deltopectoral interval is developed with lateral retraction of the cephalic vein. B. For more exposure, the superior 1 cm of the pectoralis major tendon may be incised. (ˆ, pectoralis major; #, deltoid; *,
cephalic vein.)
1. ##
Tuberosity Mobilization **The tendon of the long head of the biceps is identified as it courses in the bicipital groove toward the rotator interval. The tendon serves as a key landmark when reestablishing the anatomic relationship between the greater and lesser tuberosities. The rotator cuff interval and coracohumeral ligament are both released to allow for mobilization of the tuberosities ( TECH FIG 2A,B). If the fracture does not involve the bicipital groove, an osteotome or saw may be used to create a cleavage plane for tuberosity mobilization. Preservation of the coracoacromial ligament is advisable to maintain the coracoacromial arch. Heavy, nonabsorbable traction sutures (eg, 1-mm cottony Dacron) are placed through the rotator cuff insertions on the tuberosities. Two or three sutures should be placed through the subscapularis tendon and three or four sutures through the supraspinatus. When using a suture collar system, definitive sutures may be placed after implantation of the humeral stem.
TECH FIG 1 • Skin incision and deltopectoral approach. A. The skin incision is centered over the anterior deltoid. The deltopectoral interval is developed with lateral retraction of the cephalic vein. B. For more exposure, the superior 1 cm of the pectoralis major tendon may be incised. (ˆ, pectoralis major; #, deltoid; *,
cephalic vein.)
1. ##
Tuberosity Mobilization **The tendon of the long head of the biceps is identified as it courses in the bicipital groove toward the rotator interval. The tendon serves as a key landmark when reestablishing the anatomic relationship between the greater and lesser tuberosities. The rotator cuff interval and coracohumeral ligament are both released to allow for mobilization of the tuberosities ( TECH FIG 2A,B). If the fracture does not involve the bicipital groove, an osteotome or saw may be used to create a cleavage plane for tuberosity mobilization. Preservation of the coracoacromial ligament is advisable to maintain the coracoacromial arch. Heavy, nonabsorbable traction sutures (eg, 1-mm cottony Dacron) are placed through the rotator cuff insertions on the tuberosities. Two or three sutures should be placed through the subscapularis tendon and three or four sutures through the supraspinatus. When using a suture collar system, definitive sutures may be placed after implantation of the humeral stem.
 ---
---
 ### TECH FIG 2 • A. The long head of the biceps is identified and traced superiorly to the rotator interval. The tendon serves as a key landmark when reestablishing the anatomic relation between the greater and lesser tuberosities. B. The axillary nerve is identified at the anteroinferior border of the subscapularis.
(continued)
Tuberosity fragments vary in size and may require trimming for reduction and repair ( TECH FIG 2C,D). With the tuberosities retracted on their muscular insertions, the humeral head and shaft fragments are removed. In four-part fractures, the humeral head articular surface will be devoid of soft tissue attachments. The native articular surface is removed and sized with a template for trial humeral head replacement ( TECH FIG 2E). Obtain cancellous bone from the extracted humeral head for later bone grafting. The glenoid must be examined for concomitant pathology. Hematoma and cartilaginous or bony fragments are removed with sterile saline irrigation. Glenoid fractures should be stabilized with internal fixation. If the glenoid exhibits significant degenerative wear or irreparable damage, a glenoid component may be necessary. 205
### TECH FIG 2 • A. The long head of the biceps is identified and traced superiorly to the rotator interval. The tendon serves as a key landmark when reestablishing the anatomic relation between the greater and lesser tuberosities. B. The axillary nerve is identified at the anteroinferior border of the subscapularis.
(continued)
Tuberosity fragments vary in size and may require trimming for reduction and repair ( TECH FIG 2C,D). With the tuberosities retracted on their muscular insertions, the humeral head and shaft fragments are removed. In four-part fractures, the humeral head articular surface will be devoid of soft tissue attachments. The native articular surface is removed and sized with a template for trial humeral head replacement ( TECH FIG 2E). Obtain cancellous bone from the extracted humeral head for later bone grafting. The glenoid must be examined for concomitant pathology. Hematoma and cartilaginous or bony fragments are removed with sterile saline irrigation. Glenoid fractures should be stabilized with internal fixation. If the glenoid exhibits significant degenerative wear or irreparable damage, a glenoid component may be necessary. 205
 ---
---
 ### TECH FIG 2 •
(continued)
C. Nonabsorbable sutures are placed at the junction of the tendon-tuberosity interface and not through the tuberosities. D. Once the native humeral head is removed, the tuberosities with their respective rotator cuff attachments are mobilized for humeral canal preparation and later repair. E. Humeral head sizing. The extracted native humeral head is sized with the use of a commercially available template guide. (Copyright Steven B. Lippitt, MD.)
### TECH FIG 2 •
(continued)
C. Nonabsorbable sutures are placed at the junction of the tendon-tuberosity interface and not through the tuberosities. D. Once the native humeral head is removed, the tuberosities with their respective rotator cuff attachments are mobilized for humeral canal preparation and later repair. E. Humeral head sizing. The extracted native humeral head is sized with the use of a commercially available template guide. (Copyright Steven B. Lippitt, MD.)
-
** Humeral Shaft Preparation The proximal end of the humeral shaft is delivered into the incisional wound. Loose endosteal bone fragments and hematoma are removed from the canal of the humeral shaft. Axial reamers in 1-mm increments are used without power to prepare the humeral shaft for trial implantation.
 ---
---
 ### TECH FIG 3 • A,B. A commercially available fracture jig stably situates the implant at appropriate height and retroversion. (Courtesy of DePuy-Synthes Orthopaedics, Warsaw, IN.) In systems without a suture collar, we recommend placing the trial humeral implant with the lateral fin slightly posterior to the bicipital groove and with the medial aspect of the trial head at least at the height of the medial calcar. We currently use a commercially available fracture jig that can maintain the height and retroversion of the trial component through a functional range of motion during the provisional reduction ( TECH FIG 3).12, 14
206
3. ##
Determination of Humeral Retroversion
Correct humeral retroversion is critical when recreating the glenohumeral articulation. Most techniques suggest 30 degrees as a guide during reconstruction, although native retroversion may vary from 10 to 50 degrees. 18, 27
Several methods are employed to gauge this angle: **External rotation of the humerus to 30 degrees from the sagittal plane of the body with the humeral head component facing straight medially An imaginary line from the distal humeral epicondylar axis that bisects the axis of the prosthesis Positioning of the lateral fin of the prosthesis about 8 mm posterior to the biceps groove ( TECH FIG 4)
### TECH FIG 3 • A,B. A commercially available fracture jig stably situates the implant at appropriate height and retroversion. (Courtesy of DePuy-Synthes Orthopaedics, Warsaw, IN.) In systems without a suture collar, we recommend placing the trial humeral implant with the lateral fin slightly posterior to the bicipital groove and with the medial aspect of the trial head at least at the height of the medial calcar. We currently use a commercially available fracture jig that can maintain the height and retroversion of the trial component through a functional range of motion during the provisional reduction ( TECH FIG 3).12, 14
206
3. ##
Determination of Humeral Retroversion
Correct humeral retroversion is critical when recreating the glenohumeral articulation. Most techniques suggest 30 degrees as a guide during reconstruction, although native retroversion may vary from 10 to 50 degrees. 18, 27
Several methods are employed to gauge this angle: **External rotation of the humerus to 30 degrees from the sagittal plane of the body with the humeral head component facing straight medially An imaginary line from the distal humeral epicondylar axis that bisects the axis of the prosthesis Positioning of the lateral fin of the prosthesis about 8 mm posterior to the biceps groove ( TECH FIG 4)
 ---
---
- TECH FIG 4 • Retroversion assessment. The anterior fin of the prosthesis is aligned with the forearm in neutral rotation, and the lateral fin is positioned about 8 mm posterior to the biceps groove, establishing a retroversion angle of about 30 degrees. (Copyright Steven B. Lippitt, MD.)
-
Determination of Prosthetic Height The prosthetic height also is critical in reestablishing appropriate muscle tension and shoulder mechanics. Preoperative templating such as x-rays of the contralateral unaffected shoulder may assist in the goal of anatomic reconstruction.
 ---
---

 ### TECH FIG 5 • Height adjustment. A commercially available fracture jig permits intraoperative height adjustment. Similarly, a sponge may be placed holding the trial stem at a determined level, allowing for intraoperative assessment. (Copyright Steven B. Lippitt, MD.) Intraoperative examination of soft tissue tension, including the deltoid, rotator cuff, and the long head of the biceps, combined with fluoroscopic imaging aids in prosthetic height placement. Common errors involve placing the prosthesis too low, resulting in poor deltoid muscle tension and no room for the tuberosities ( TECH FIG 5). 5. ## Trial Reduction Two to four drill holes are placed in the proximal humerus medial and lateral to the bicipital groove, with no. 2 nonabsorbable sutures subsequently passed for fixation of the tuberosity to the shaft. With the suture collar technique, drill holes are made through the anterolateral and posterolateral aspects of the proximal humerus, approximately 2 cm below the fracture line ( TECH FIG 6A). A trial reduction is then performed with the mobilized tuberosities fitted below the head of the modular prosthetic head or suture collar. A towel clip or specially designed tuberosity clamp may be used to hold the tuberosities for fluoroscopic examination and assessment of glenohumeral stability. Intraoperative fluoroscopy is helpful in confirming appropriate implant height and glenohumeral stability ( TECH FIG 6B,C). To ensure adequate deltoid tensioning, the humeral head should not subluxate more than 25% to 30% of the glenoid height inferiorly. 207
### TECH FIG 5 • Height adjustment. A commercially available fracture jig permits intraoperative height adjustment. Similarly, a sponge may be placed holding the trial stem at a determined level, allowing for intraoperative assessment. (Copyright Steven B. Lippitt, MD.) Intraoperative examination of soft tissue tension, including the deltoid, rotator cuff, and the long head of the biceps, combined with fluoroscopic imaging aids in prosthetic height placement. Common errors involve placing the prosthesis too low, resulting in poor deltoid muscle tension and no room for the tuberosities ( TECH FIG 5). 5. ## Trial Reduction Two to four drill holes are placed in the proximal humerus medial and lateral to the bicipital groove, with no. 2 nonabsorbable sutures subsequently passed for fixation of the tuberosity to the shaft. With the suture collar technique, drill holes are made through the anterolateral and posterolateral aspects of the proximal humerus, approximately 2 cm below the fracture line ( TECH FIG 6A). A trial reduction is then performed with the mobilized tuberosities fitted below the head of the modular prosthetic head or suture collar. A towel clip or specially designed tuberosity clamp may be used to hold the tuberosities for fluoroscopic examination and assessment of glenohumeral stability. Intraoperative fluoroscopy is helpful in confirming appropriate implant height and glenohumeral stability ( TECH FIG 6B,C). To ensure adequate deltoid tensioning, the humeral head should not subluxate more than 25% to 30% of the glenoid height inferiorly. 207
 ---
---

 ### TECH FIG 6 • A. Humeral shaft preparation. Drill holes are placed in the proximal humerus medial and lateral to the bicipital groove with 1-mm cottony Dacron or no. 2 nonabsorbable sutures. B. Trial reduction. A trial reduction may be performed with the fracture jig in place, allowing assessment of the functional range of motion. C. An intraoperative fluoroscopic image confirms prosthetic height and tuberosity reduction prior to implantation of the final implant. (A,B: Copyright Steven B. Lippitt, MD; C: Copyright Kamal I. Bohsali, MD.)
### TECH FIG 6 • A. Humeral shaft preparation. Drill holes are placed in the proximal humerus medial and lateral to the bicipital groove with 1-mm cottony Dacron or no. 2 nonabsorbable sutures. B. Trial reduction. A trial reduction may be performed with the fracture jig in place, allowing assessment of the functional range of motion. C. An intraoperative fluoroscopic image confirms prosthetic height and tuberosity reduction prior to implantation of the final implant. (A,B: Copyright Steven B. Lippitt, MD; C: Copyright Kamal I. Bohsali, MD.)
-
Final Implant Placement The final humeral component should be cemented in patients with osteoporotic bone and/or poor diaphyseal fixation. More recent implant designs allow for press-fit placement of the humeral component. A cement restrictor is placed to prevent cement extravasation distally. Pulsatile lavage and retrograde injection of cement with suction pressurization also is used ( TECH FIG 7A). Excess cement is removed during the curing phase. Spaces between the tuberosities, prosthesis, and shaft are packed with autogenous cancellous bone graft from the resected humeral head ( TECH FIG 7B). A second reduction may be performed with the trial head after cement or press-fit fixation of the humeral stem. The final head may be impacted before stem implantation or after the repeat trial reduction. When using a suture collar, suture passage may be more facile without the final humeral head in position. A cerclage suture is placed circumferentially around the greater tuberosity and through the supraspinatus insertion, and then medial or through the prosthesis and subscapularis insertion (lesser tuberosity). Several authors have indicated superior fixation with the cerclage suture when compared to tuberosity-totuberosity and tuberosity-to-fin fixation alone. 9, 23 Overreduction of the tuberosities should be avoided to prevent limitations in external (lesser tuberosity) and internal (greater tuberosity) rotation. The order and configuration of suture tying may vary due to surgeon preference and implant-specific instructions. In general, sutures are tied, beginning with tuberosity-to-shaft reapproximation followed by tuberosity-to-tuberosity closure using the previously placed suture limbs ( TECH FIG 7C). The lateral portion of the rotator interval is closed with the arm in approximately 30 degrees of external rotation with no. 2 nonabsorbable sutures as needed ( TECH FIG 7D). 208
 ---
---


 ### TECH FIG 7 • A. If using cement, a restrictor is placed to prevent extravasation distally. Pulsatile lavage and retrograde injection of cement with suction pressurization are also used. B. Morselized cancellous bone graft is placed between the tuberosities and shaft. C. Tuberosity fixation. Previously placed suture limbs through the tuberosities and shaft are reapproximated. D. A medial cerclage suture is placed circumferentially around the greater tuberosity and through the supraspinatus insertion and then medial to or through the medial hole of the prosthesis and through the subscapularis insertion (lesser tuberosity) and tied. E. The rotator interval is closed with no. 2 nonabsorbable suture with the arm in about 30 degrees of external rotation. ( A,C,E: Copyright Steven B. Lippitt, MD; B: Courtesy of DePuy-Synthes Orthopaedics, Warsaw, IN.) 1. ## Surgical Wound Closure The deltopectoral interval usually is not closed. Drain suction is recommended in both acute and chronic injuries to prevent hematoma formation. A commercially available pain pump may be used to augment postoperative analgesia and to reduce narcotic medication use. The subcutaneous tissues are reapproximated with 2-0 absorbable suture. Subcuticular closure is performed with 2-0 monofilament suture. The patient is then placed in a sling or shoulder immobilizer with 45 degrees of abduction for comfort.
209
## PEARLS AND PITFALLS Indications ▪ A complete history and physical examination should be performed, with particular attention paid to the neurovascular status. Imaging studies 1. Appropriate plain radiographs with possible CT scan supplementation aid in the surgical decision making. C-arm fluoroscopy is useful for intraoperative implant and tuberosity positioning. Tuberosity identification 1. Use the long head of the biceps to define the tuberosities for mobilization. 2.
Tag this for later tenodesis before wound closure. Implant placement
1.
Know the specifics of the implant system including its limitations.
2. Place the implant in appropriate retroversion (approximately 20-30 degrees). 3. Check the height of the trial stem before performing cement fixation using a fracture jig or sponge for provisional fixation. 4. Intraoperative fluoroscopy can be used to assess appropriate implant height. Tuberosity fixation 5. Avoid loss of external rotation or internal rotation with overreduction of the lesser and greater tuberosities, respectively. Postoperative rehabilitation 1. On postoperative day 1, initiate gentle pendulum exercises, with passive forward flexion and external rotation (at 0 degrees of abduction). Always modify rehabilitation protocol based on intraoperative assessment of soft tissue compromise and patient neurologic status. ## POSTOPERATIVE CARE Physician-directed therapy is initiated on postoperative day 1 with gentle, gravity-assisted pendulum exercises, as well as passive pulley-and-stick exercises to maintain forward flexion and external rotation (motion limits placed by surgeon based on intraoperative stability). After discharge, the patient's wound is reexamined and sutures removed at 10 to 14 days. Gentle range-of-motion exercises are continued. At 6 weeks, repeat radiographs are obtained to evaluate tuberosity healing. When tuberosity healing is evident, phase 2 exercises are initiated with isometric rotator cuff exercises and active-assisted elevation with the pulley. At 3 months, strength training with graduated rubber bands (phase 3) is implemented. Maximal motion and function are obtained at about 12 months from date of surgery. ## OUTCOMES About 90% of patients treated with hemiarthroplasty demonstrate minimal pain, despite a wide range of function, motion, and strength. Factors that portend a poor outcome after hemiarthroplasty for fractures include tuberosity malposition, superior migration of the humeral prosthesis, stiffness, persistent pain, poor initial positioning of the implant (excessive retroversion, decreased height), and age older than 75 years in women. 4, 5, 27 When comparing acute intervention versus late reconstruction, most authors report poorer outcomes with delayed surgical intervention (more than 2 weeks), particularly with functional results. 22, 29 ## COMPLICATIONS Complications include delays in wound healing, infection, nerve injury, humeral fracture, component malposition, instability, nonunion of the tuberosities, rotator cuff tearing, regional pain syndrome, periarticular fibrosis, heterotopic bone formation, component loosening, and glenoid arthritis. 3, 7, 21 The most common problems in acute fracture treatment involve stiffness, nonunion, malunion, or resorption of the tuberosities. 7, 21 In patients with chronic fractures treated with hemiarthroplasty, the most common problems encountered were instability, heterotopic ossification, tuberosity malunion or nonunion, and rotator cuff tears. 21 ##
### TECH FIG 7 • A. If using cement, a restrictor is placed to prevent extravasation distally. Pulsatile lavage and retrograde injection of cement with suction pressurization are also used. B. Morselized cancellous bone graft is placed between the tuberosities and shaft. C. Tuberosity fixation. Previously placed suture limbs through the tuberosities and shaft are reapproximated. D. A medial cerclage suture is placed circumferentially around the greater tuberosity and through the supraspinatus insertion and then medial to or through the medial hole of the prosthesis and through the subscapularis insertion (lesser tuberosity) and tied. E. The rotator interval is closed with no. 2 nonabsorbable suture with the arm in about 30 degrees of external rotation. ( A,C,E: Copyright Steven B. Lippitt, MD; B: Courtesy of DePuy-Synthes Orthopaedics, Warsaw, IN.) 1. ## Surgical Wound Closure The deltopectoral interval usually is not closed. Drain suction is recommended in both acute and chronic injuries to prevent hematoma formation. A commercially available pain pump may be used to augment postoperative analgesia and to reduce narcotic medication use. The subcutaneous tissues are reapproximated with 2-0 absorbable suture. Subcuticular closure is performed with 2-0 monofilament suture. The patient is then placed in a sling or shoulder immobilizer with 45 degrees of abduction for comfort.
209
## PEARLS AND PITFALLS Indications ▪ A complete history and physical examination should be performed, with particular attention paid to the neurovascular status. Imaging studies 1. Appropriate plain radiographs with possible CT scan supplementation aid in the surgical decision making. C-arm fluoroscopy is useful for intraoperative implant and tuberosity positioning. Tuberosity identification 1. Use the long head of the biceps to define the tuberosities for mobilization. 2.
Tag this for later tenodesis before wound closure. Implant placement
1.
Know the specifics of the implant system including its limitations.
2. Place the implant in appropriate retroversion (approximately 20-30 degrees). 3. Check the height of the trial stem before performing cement fixation using a fracture jig or sponge for provisional fixation. 4. Intraoperative fluoroscopy can be used to assess appropriate implant height. Tuberosity fixation 5. Avoid loss of external rotation or internal rotation with overreduction of the lesser and greater tuberosities, respectively. Postoperative rehabilitation 1. On postoperative day 1, initiate gentle pendulum exercises, with passive forward flexion and external rotation (at 0 degrees of abduction). Always modify rehabilitation protocol based on intraoperative assessment of soft tissue compromise and patient neurologic status. ## POSTOPERATIVE CARE Physician-directed therapy is initiated on postoperative day 1 with gentle, gravity-assisted pendulum exercises, as well as passive pulley-and-stick exercises to maintain forward flexion and external rotation (motion limits placed by surgeon based on intraoperative stability). After discharge, the patient's wound is reexamined and sutures removed at 10 to 14 days. Gentle range-of-motion exercises are continued. At 6 weeks, repeat radiographs are obtained to evaluate tuberosity healing. When tuberosity healing is evident, phase 2 exercises are initiated with isometric rotator cuff exercises and active-assisted elevation with the pulley. At 3 months, strength training with graduated rubber bands (phase 3) is implemented. Maximal motion and function are obtained at about 12 months from date of surgery. ## OUTCOMES About 90% of patients treated with hemiarthroplasty demonstrate minimal pain, despite a wide range of function, motion, and strength. Factors that portend a poor outcome after hemiarthroplasty for fractures include tuberosity malposition, superior migration of the humeral prosthesis, stiffness, persistent pain, poor initial positioning of the implant (excessive retroversion, decreased height), and age older than 75 years in women. 4, 5, 27 When comparing acute intervention versus late reconstruction, most authors report poorer outcomes with delayed surgical intervention (more than 2 weeks), particularly with functional results. 22, 29 ## COMPLICATIONS Complications include delays in wound healing, infection, nerve injury, humeral fracture, component malposition, instability, nonunion of the tuberosities, rotator cuff tearing, regional pain syndrome, periarticular fibrosis, heterotopic bone formation, component loosening, and glenoid arthritis. 3, 7, 21 The most common problems in acute fracture treatment involve stiffness, nonunion, malunion, or resorption of the tuberosities. 7, 21 In patients with chronic fractures treated with hemiarthroplasty, the most common problems encountered were instability, heterotopic ossification, tuberosity malunion or nonunion, and rotator cuff tears. 21 ##
Scientific References
- 1. Beredjiklian PK, Iannotti JP, Norris TR, et al. Operative treatment of malunion of a fracture of the proximal aspect of the humerus. J Bone Joint Surg Am 1998;80:1484-1497. 2. Bohsali KI, Wirth MA. Fractures of the proximal humerus. In: Rockwood CA Jr, Matsen FA III, Wirth MA, et al, eds. The Shoulder, ed 4. Philadelphia: Elsevier, 2009:295-332. 3. Bohsali KI, Wirth MA, Rockwood CA Jr. Current concepts review: complications of total shoulder arthroplasty. J Bone Joint Surg Am 2006;88A:2279-2292. 4. Boileau P, Krishnan SG, Tinsi L, et al. Tuberosity malposition and migration: reason for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412. 5. Boileau P, Walch G, Trojani C, et al. Surgical classification and limits of shoulder arthroplasty. In: Walch G, Boileau P, eds. Shoulder Arthroplasty. Berlin: Springer-Verlag, 1999:349-358. 6. Bosch U, Skutek M, Fremery RW, et al. Outcome after primary and secondary hemiarthroplasty in elderly patients with fractures of the proximal humerus. J Shoulder Elbow Surg 1998;7: 479-484. 7. Compito CA, Self EB, Bigliani LU. Arthroplasty and acute shoulder trauma. Clin Orthop Relat Res 1994;307:27-36. 8. DeFranco MJ, Brems JJ, Williams GR Jr, et al. Evaluation and management of valgus impacted four-part proximal humerus fractures. Clin Orthop Relat Res 2006;442:109-114. 9. Frankle MA, Ondrovic LE, Markee BA, et al. Stability of tuberosity attachment in proximal humeral arthroplasty. J Shoulder Elbow Surg 2002;11:413-420. 10. Gerber C, Schneeberger A, Vinh T. The arterial vascularization of the humeral head: an anatomical study. J Bone Joint Surg Am 1990;72:1486-1494. 11. Green A. Proximal humerus fractures. In: Norris T, ed. Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL: AAOS, 2002:209-217. 12. Green A, Lippitt SB, Wirth MA. Humeral head replacement arthroplasty. In: Wirth MA, ed. Proximal Humerus Fractures. Rosemont, IL: AAOS, 2005:39-48. 13. Green A, Norris T. Proximal humerus fractures and fracture-dislocations. In: Jupiter J, ed. Skeletal Trauma, ed 3. Philadelphia: WB Saunders, 2003:1532-1624. **210** 14. Hartsock LA, Estes WJ, Murray CA, et al. Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29(3): 467-475. 15. Hertel R, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg 2004;13:427-433. 16. Hettrich CM, Boraiah S, Dyke JP, et al. Quantitative assessment of the vascularity of the proximal part of the humerus. J Bone Joint Surg Am 2010;92(4):943-948. 17. Huopio J, Kroger H, Honkanen R, et al. Risk factors for perimenopausal fractures: a prospective study. Osteoporos Int 2000;11: 219-227. 18. Iannotti JP, Gabriel JP, Schneck SL, et al. The normal glenohumeral relationships: an anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992;74A:491-500. 19. Jakob R, Miniaci A, Anson P, et al. Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73B: 295-298. 20. Laing The arterial supply of the adult humerus. J Bone Joint Surg Am 1956;38A:1105-1116. 21. Muldoon MP, Cofield RH. Complications of humeral head replacement for proximal humerus fractures. Instr Course Lect 1997:46: 15-24. 22. Neer CS. Displaced proximal humeral fractures. Part II: treatment of 3-part and 4-part displacement. J Bone Joint Surg Am 1970;52A: 1090-1103. 23. Nho SJ, Brophy RH, Barker JU, et al. Innovations in the management of proximal humerus fractures. J Am Acad Orthop Surg 2007;15:12-26. 24. Norris TR, Green A, McGuigan FX. Late prosthetic shoulder arthroplasty for displaced proximal humerus fractures. J Shoulder Elbow Surg 1995;4:271-280. 25. Olerud P, Ahrengart L, Ponzer S, et al. Hemiarthroplasty versus nonoperative treatment of displaced 4-part proximal humeral fractures in elderly patients: a randomized controlled trial. J Shoulder Elbow Surg 2011;20:1025-1033. 26. Orthopaedic Trauma Association Committee for Coding and Classification: fracture and dislocation compendium. J Orthop Trauma 1996;10(suppl):1-155. 27. Pearl ML, Volk AG. Retroversion of the proximal humerus in relationship to the prosthetic replacement arthroplasty. J Shoulder Elbow Surg1995;4:286-289. 28. Stableforth PG. Four part fractures of the neck of the humerus. J Bone Joint Surg Br 1984;66B:104-108. [View Source / PubMed]
- 29. Zuckerman JD, Cuomo F, Koval KJ. Proximal humeral replacement for complex fractures: indications and surgical technique. Instr Course Lect 1997;46:7-14. [View Source / PubMed]
You Might Also Like