Mastering Plate Osteosynthesis for Humeral Shaft Fractures
Key Takeaway
Plate osteosynthesis remains the gold standard for operative fixation of humeral shaft fractures. Offering superior rotational stability and direct anatomical reduction, plating yields union rates exceeding 96%. This comprehensive guide details evidence-based indications, implant selection, surgical approaches, and postoperative protocols to optimize clinical outcomes and minimize complications such as iatrogenic radial nerve palsy.
INTRODUCTION TO PLATE OSTEOSYNTHESIS
Plate osteosynthesis remains the unequivocal “gold standard” for the operative fixation of humeral shaft fractures. While conservative management via functional bracing is highly successful for many isolated injuries, surgical intervention is mandated for specific fracture patterns, polytraumatized patients, and cases with associated neurovascular compromise. Plating provides robust biomechanical stability, allowing for early upper extremity weight-bearing—a critical factor in the rehabilitation of patients with multiple injuries.
Extensive literature supports the efficacy of this technique. Five large series (Foster et al., McKee et al., Vander Griend et al., Bell et al., and Tingstad et al.) encompassing 361 fractures demonstrated an exceptional average union rate of 96.7%. Furthermore, plating produces minimal shoulder or elbow morbidity compared to alternative fixation methods.
Plating vs. Intramedullary Nailing
The debate between plate osteosynthesis and intramedullary (IM) nailing has been extensively studied. Prospective, randomized comparisons reveal no significant differences in overall union rates or elbow function; however, critical distinctions exist regarding shoulder morbidity.
Clinical Pearl: Shoulder impingement and rotator cuff morbidity occur significantly more often with antegrade intramedullary nailing than with plate fixation. Furthermore, reoperation rates are statistically higher in patients treated with IM nails.
While patients may experience slightly more immediate postoperative shoulder pain following IM nailing, long-term shoulder flexion is demonstrably better in patients treated with compression plating. Updated meta-analyses, such as those by Heineman et al., suggest that while neither technique is universally superior for all fracture types, plating remains the preferred choice to avoid rotator cuff pathology and achieve direct anatomical reduction.
INDICATIONS FOR OPERATIVE TREATMENT
The decision to proceed with operative treatment depends on a complex interplay of fracture morphology, associated injuries, and patient-specific factors. McKee elegantly divided these indications into three distinct categories. While some indications are absolute (e.g., vascular injury), others remain relative and require astute clinical judgment.
Fracture-Specific Indications
- Failure of Closed Reduction: Inability to obtain or maintain acceptable alignment in a functional brace. Acceptable parameters include:
- Shortening < 3 cm
- Angulation < 20 degrees
- Rotation < 30 degrees
- Segmental Fractures: Prone to nonunion and difficult to control with bracing.
- Pathological Fractures: Require rigid stabilization and often tumor resection/augmentation.
- Intra-articular Extension: Fractures extending into the shoulder or elbow joints necessitate anatomical reduction.
Associated Injuries
- Open Fractures: Require aggressive debridement and stable fixation to protect soft tissues.
- Vascular Injury: Rigid skeletal stabilization is required prior to or immediately following vascular repair.
- Brachial Plexus Injury: Fixation aids in nerve exploration and rehabilitation.
- Ipsilateral Fractures: "Floating elbow" (ipsilateral forearm fracture) or ipsilateral shoulder/elbow fractures.
- Bilateral Humeral Fractures: Precludes the use of functional bracing and severely limits patient independence.
- Lower Extremity Fractures: Requires the upper extremities to be weight-bearing for crutch or walker use.
- High-Velocity Gunshot Injuries & Burns: Soft tissue compromise precludes bracing.
Patient-Specific Indications
- Polytrauma: Early mobilization is critical to prevent pulmonary complications (ARDS) and deep vein thrombosis.
- Severe Head Injury: Patients with a Glasgow Coma Scale (GCS) score ≤ 8 often exhibit spasticity, making brace management impossible.
- Poor Compliance or Tolerance: Patients unable to adhere to the strict protocols of functional bracing.
- Unfavorable Body Habitus: Morbid obesity or large breasts can mechanically displace a functional brace, leading to varus malunion.
PREOPERATIVE PLANNING AND IMPLANT SELECTION
Implant selection is dictated by bone quality, fracture pattern, and the anatomical location of the injury. The primary goal is to achieve absolute stability for simple fracture patterns or relative stability for complex, comminuted patterns.
Standard Diaphyseal Plating
The most commonly utilized implant for diaphyseal humeral shaft fractures is the broad, 4.5-mm limited-contact dynamic compression plate (LC-DCP).

For patients with smaller skeletal anatomy, a narrow 3.5-mm or 4.5-mm LC-DCP may be appropriate. The limited-contact design minimizes periosteal vascular disruption, thereby optimizing the biological environment for fracture healing.
Metaphyseal-Diaphyseal Transition Zones
Fractures located at the distal metaphyseal-diaphyseal junction present a unique biomechanical challenge due to the flaring of the bone and the limited distal footprint for screw purchase. These injuries often require dual 3.5-mm LC-DCPs or anatomically pre-contoured extra-articular distal humerus plates.

Construct Biomechanics Based on Fracture Pattern
- Transverse Fractures: Ideally suited for compression plating. Axial compression generates absolute stability, promoting primary bone healing.
- Spiral or Oblique Fractures: The optimal construct utilizes a lag screw for interfragmentary compression, protected by a neutralization plate.
Surgical Technique Pearl (The Eglseder Technique): Attaining provisional reduction of a spiral/oblique fracture can be challenging. Utilizing a mini-fragment plate (e.g., 2.0 or 2.4 mm) or independent lag screws allows for direct observation of the anatomical reduction. This simplifies the application of the definitive neutralization plate and significantly limits the periosteal stripping caused by large reduction clamps.

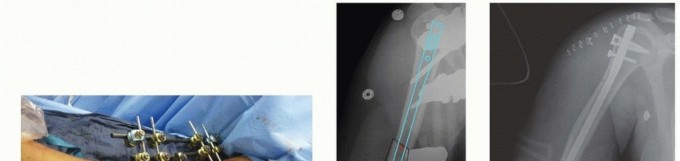
Figure 57-37 A: Displaced humeral shaft fracture.

Figure 57-37 B: After fixation with mini-fragment plate (Eglseder technique) and definitive compression plating.
- Comminuted Fractures: Require a bridge plating technique. Anatomical reduction of every intermediate fragment is unnecessary and biologically detrimental. The surgeon must focus on restoring correct alignment, rotation, and length while preserving the soft tissue envelope attached to the comminuted fragments.
Osteoporotic Bone and Complex Segmental Fractures
In patients with poor bone quality or long segmental defects, standard fixation may fail. To improve construct stability, longer implants must be utilized to increase the working length.

Figure 57-38 A: Segmental shaft fracture with extension into the proximal humerus.

Figure 57-38 B: Long plate utilized to obtain secure fixation across the segmental defect.

Figure 57-38 C: Lateral radiographic view demonstrating secure fixation with a long plate.
Biomechanical Rules for Poor Bone Quality:
1. Cortical Purchase: A minimum of eight cortices (four screws) above and below the fracture zone is strictly necessary to prevent screw pullout.
2. Plate Length: The length of the plate is just as critical as the number of screws. A longer plate increases the lever arm and distributes stress over a larger area of the diaphysis.
3. Locking Technology: Locking screws should be reserved for osteoporotic bone, short periarticular segments, or when screw augmentation with methyl methacrylate is required.
SURGICAL ANATOMY AND APPROACHES
The humerus can be approached from multiple angles, but the choice of approach is dictated by the fracture location and the planned plate position.
The Anterolateral Approach (Brachialis-Splitting)
This approach is the workhorse for fractures involving the proximal and middle thirds of the humeral shaft.
* Positioning: Supine or beach-chair position with the arm draped free.
* Internervous Plane: Proximally between the deltoid (axillary nerve) and pectoralis major (medial/lateral pectoral nerves). Distally, the brachialis muscle is split longitudinally. The medial half of the brachialis is innervated by the musculocutaneous nerve, while the lateral half is innervated by the radial nerve, making this a true internervous split.
* Radial Nerve Considerations: The radial nerve pierces the lateral intermuscular septum to enter the anterior compartment at the junction of the middle and distal thirds of the humerus. It must be meticulously identified and protected. When applying the plate, the surgeon must ensure the nerve is not trapped beneath the implant.
The Posterior Approach (Triceps-Splitting or Modified)
The posterior approach is ideal for midshaft fractures and those extending into the distal third of the humerus.
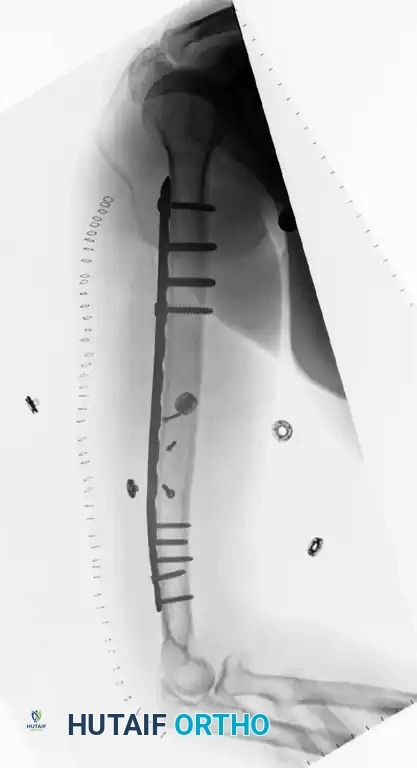
Figure 57-39 A: Fracture of the distal third of the humeral shaft.

Figure 57-39 B: Postoperative radiograph after plate fixation through a posterior triceps-splitting approach.
- Positioning: Lateral decubitus or prone position.
- Standard Triceps-Splitting: The triceps fascia is incised, and the muscle belly is split bluntly in the midline to expose the posterior humerus.
- Modified Posterior Approach (Gerwin, Hotchkiss, Weiland): Instead of splitting the triceps, the entire triceps muscle is reflected medially off the lateral intermuscular septum. This advanced technique exposes an average of 10 cm more of the humeral shaft compared to the standard split and provides unparalleled visualization of the radial nerve.
Minimally Invasive Plate Osteosynthesis (MIPO)
While MIPO has revolutionized the treatment of lower extremity fractures, its application in the humerus remains controversial due to the profound risk of iatrogenic radial nerve injury. Cadaveric studies demonstrate that during anterior MIPO, the plate sits an average of only 3.2 mm (range 2 to 4.9 mm) from the radial nerve.
Surgical Warning: Pronation of the forearm moves the radial nerve 3 mm closer to the anterior plate. Due to the proximity of the nerve and the lack of large-scale clinical validation, MIPO for the humeral shaft should be approached with extreme caution and is generally reserved for highly specialized centers.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The primary advantage of plate osteosynthesis is the ability to initiate early, aggressive rehabilitation.
- Range of Motion (ROM): Active and active-assisted ROM of the shoulder and elbow should begin within the first week postoperatively.
- Weight-Bearing: If absolute stability is achieved, early upper extremity weight-bearing is permitted, which is vital for polytrauma patients requiring crutches.
- Biomechanical Limitations: Surgeons must be aware of implant limitations. Biomechanical studies indicate that during bilateral crutch weight-bearing:
- A large construct (4.5-mm plate) will not fail with loads of 90 kg (~200 lbs) or less.
- A small fragment construct (3.5-mm plate) will experience plastic deformation and predicted failure in patients weighing 70 kg (~150 lbs) or more.
COMPLICATIONS AND MANAGEMENT
While plate osteosynthesis is highly successful, complications can occur and must be managed promptly.
Radial Nerve Palsy
Radial nerve palsy is the most frequently reported complication.
* Iatrogenic Injury: Often caused by excessive traction, entrapment under the plate during an anterolateral approach, or inadequate soft tissue release during a posterior approach.
* Management: If a patient awakens with a new-onset radial nerve palsy after plating, immediate surgical exploration is mandatory to ensure the nerve is not trapped beneath the plate or severed by a drill bit. If the nerve was visualized and protected during surgery, a period of observation with supportive splinting is appropriate.
Infection
Surgical site infections occur in approximately 1% to 2% of closed humeral fractures and up to 5% of open fractures. Treatment requires aggressive surgical debridement, targeted intravenous antibiotics, and retention of the hardware if the fixation remains absolutely stable. If the hardware is loose, it must be removed, and the fracture stabilized with an external fixator.
Nonunion and Refracture
Nonunion of the humeral shaft after plating is infrequent but can occur due to inadequate fixation (e.g., insufficient working length) or biological failure (e.g., excessive periosteal stripping). Refractures occur in approximately 1% of patients, typically after premature hardware removal. Routine removal of humeral plates is strongly discouraged unless symptomatic.
📚 Medical References
- plate osteosynthesis of distal fractures of the tibia, Injury 28:42, 1997.
- Helfet DL, Sorkin AT, Levine DS, et al: Minimally invasive plate osteosynthesis of distal tibial fractures, Tech Orthop 14:191, 1999.
- Herscovici D, Sanders RW, Infante A: Böhler incision: an extensile anterolateral approach to the foot and ankle, J Orthop Trauma 13:586, 1999.
- Hirvensalo E: Fracture fi xation with biodegradable rods: fortyone cases of severe ankle fractures, Acta Orthop Scand 60:601, 1989.
- Hovis WD, Bucholz RW: Polyglycolide bioabsorbable screws in the treatment of ankle fractures, Foot Ankle Int 18:128, 1997.
- Hovis WD, Kaiser BW, Watson JT, et al: Treatment of syndesmotic disruptions of the ankle with bioabsorbable screw fi xation, J Bone Joint Surg 84A:26, 2002.
- Hughes JL, Weber H, Willenegger H, et al: Evaluation of ankle fractures: nonoperative and operative treatment, Clin Orthop Relat Res 138:111, 1979.
- Johnson DP, Hill J: Fracture-dislocation of the ankle with rupture of the deltoid ligament, Injury 19:59, 1988.
- Johnson EE, Davlin LB: Open ankle fractures: the indications for immediate open reduction and internal fi xation, Clin Orthop 292:118, 1993.
- Joy G, Patzakis MJ, Harvey JP Jr: Precise evaluation of the reduction of severe ankle fractures: technique and correlation with end results, J Bone Joint Surg 56A:979, 1974.
- Kao KF, Huang PJ, Chen YW, et al: Postero-medio-anterior approach of the ankle for the pilon fracture, Injury 31:71, 2000.
- Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw, Foot Ankle 9:290, 1989.
- Kellam JF, Waddell JP: Fractures of the distal tibial metaphysis with intraarticular extension—the distal tibial explosion fracture, J Trauma 19:593, 1979.
- Ketenjian AY, Shelton ML: Primary internal fi xation of open fractures: a retrospective study of the use of metallic internal fi xation in fresh open fractures, J Trauma 12:756, 1972.
- Kim SK, Oh JK: One or two lag screws for fi xation of Danis-Weber type B fractures of the ankle, J Trauma 46:1039, 1999.
- Konrath GA, Hopkins G II: Posterolateral approach for tibial pilon fractures: a report of two cases, J Orthop Trauma 13:586, 1999.
- Konvath G, Karges D, Watson JT, et al: Early versus delayed treatment of severe ankle fracture: a comparison of results, J Orthop Trauma 9:377, 1995.
- Koval KJ, Petraco DM, Kummer FJ, et al: A new technique for complex fi bula fracture fi xation in the elderly: a clinical and biomechanical evaluation, J Orthop Trauma 11:28, 1997.
- Kristensen KD, Hansen T: Closed treatment of ankle fractures: stage II supination-eversion fractures followed for 20 years, Acta Orthop Scand 56:107, 1985.
- Laskin RS: Steinmann pin fi xation in the treatment of unstable fractures of the ankle, J Bone Joint Surg 56A:549, 1974.
- Lauge-Hansen N: Fractures of the ankle, II: combined experimental-surgical and experimental-roentgenologic investigations, Arch Surg 60:957, 1950.
- Lauge-Hansen N: Fractures of the ankle, V: pronationdorsifl exion fracture, Arch Surg 67:813, 1953.
- Leach RE: Ankle fractures: internal fi xation, III: fractures of the tibial plafond, Instr Course Lect 28:88, 1979.
- Lee HG, Horan TB: Internal fi xation in injuries of the ankle, Surg Gynecol Obstet 76:593, 1943.
- Loren GJ, Ferkel RD: Arthroscopic assessment of occult intraarticular injury in acute ankle fractures, Arthroscopy 18:412, 2002.
- Lynn MD: The triplane distal tibial epiphyseal fracture, Clin Orthop Relat Res 86:187, 1972.
- Maale G, Seligson D: Fractures through the weight-bearing surface of the distal tibia, Orthopedics 3:517, 1980.
- Makwana NK, Bhowal B, Harper WM, et al: Conservative versus operative treatment for displaced ankle fracture in patients over 55 years of age: a prospective, randomized study, J Bone Joint Surg 83B:525, 2001.
- Marmor L: An unusual fracture of the tibial epiphysis, Clin Orthop 73:132, 1970.
- Marsh JL: Current controversies in orthopaedic trauma: external fi xation is the treatment of choice for fractures of the tibial plafond, J Orthop Trauma 13:583, 1999.
- Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fi xator for fractures of the tibial plafond, J Bone Joint Surg 77A:1498, 1995.
- Marsh JL, Muehling V, Dirschl D, et al: Tibial plafond fractures treated by articulated external fi xation: a randomized trial of postoperative motion versus nonmotion, J Orthop Trauma 20:536, 2006.
- Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: how do these ankles function over time? J Bone Joint Surg 85A:287, 2003.
- Mast J: Reduction techniques in fractures of the distal tibial articular surface, Tech Orthop 2:29, 1987.
- Mast JW, Spiegel PG, Pappas JN: Fractures of the tibial pilon, Clin Orthop Relat Res 230:68, 1988.
- McCormack RG, Leith JM: Ankle fractures in diabetics: complications of surgical management, J Bone Joint Surg 80B:689, 1998.
- McDade WC: Diagnosis and treatment of ankle injuries, Instr Course Lect 24:251, 1975.
- McLennan JG, Ungersma J: Evaluation of the treatment of ankle fractures with the Inyo nail, J Orthop Trauma 2:272, 1989.
- Meyers MH: Fracture about the ankle joint with fi xed displacement of the proximal fragment of the fi bula behind the tibia, Clin Orthop Relat Res 42:67, 1965.
- Michelson JD: Current concepts review: fractures about the ankle, J Bone Joint Surg 77A:142, 1995.
- Michelson JD, Helgemo SL, Ahn UM: Dynamic biomechanics of the normal and fractured ankle, Trans Orthop Res Soc 40:253, 1994.
- Molinari M, Bertoldi L, De March L: Fracture dislocation of the ankle with the fi bula trapped behind the tibia: a case report, Acta Orthop Scand 61:471, 1990.
- Müller ME, Allgöwer M, Schneider R, et al: Manual of internal fi xation: techniques recommended by the AO group, 2nd ed, New York, 1979, Springer-Verlag. Myerson MS, Edwards WHB: Management of neuropathic fractures in the foot and ankle, J Am Acad Orthop Surg 7:8, 1999.
- Namba RS, Kabo JM, Dorey FJ, et al: Continuous passive motion versus immobilization: the effect on posttraumatic joint stiffness, Clin Orthop Relat Res 267:218, 1991.
- Needleman RL, Skrade DA, Stiehl JB: Effect of the syndesmotic screw on ankle motion, Foot Ankle 10:17, 1989.
- Ngcelwane MV: Management of open fractures of the ankle joint, Injury 21:93, 1990.
- Nielsen JO, Dons-Jensen H, Sorensen HT: Lauge-Hansen classifi cation of malleolar fractures: an assessment of the reproducibility in 118 cases, Acta Orthop Scand 61:385, 1990.
- Okcu G, Aktuglu K: Intra-articular fractures of the tibial plafond: a comparison of the results using articulated and ring external fi xators, J Bone Joint Surg 86B:868, 2004.
- O’Leary C, Ward FJ: A unique closed abduction-external rotation ankle fracture, J Trauma 29:119, 1989.
- Olerud S, Johansson H: The lateral malleolus, Ann Dig Foreign Orthop Lit 3rd qtr:29, 1970.
- Orava S, Karpakka J, Taimela S, et al: Stress fracture of medial malleolus, J Bone Joint Surg 77A:362, 1995.
- Ostrum RF: Posterior plating of displaced Weber B fi bula fractures, J Orthop Trauma 10:199, 1996.
- Ovadia DN, Beals RK: Fractures of the tibial plafond, J Bone Joint Surg 68A:543, 1986.
- Pankovich AM: Fractures of the fi bula at the distal tibiofi bular syndesmosis, Clin Orthop Relat Res 143:138, 1979.
- Pankovich AM, Shivaram MS: Anatomical basis of variability in injuries of the medial malleolus and the deltoid ligament, I: anatomical studies; II: clinical studies, Acta Orthop Scand 50:217, 1979.
- Park JW, Kim SK, Hong JS, et al: Anterior tibiofi bular ligament avulsion fracture in Weber type B lateral malleolar fracture, J Trauma 52:655, 2002.
- Park SS, Kubiak EN, Egol KA, et al: Stress radiographs after ankle fracture: the effect of ankle position and deltoid ligament status on medial clear space measurements, J Orthop Trauma 20:11, 2006.
- Parrish TF: Fracture dislocation of the ankle—an unusual cause of failure of reduction: a case report, J Bone Joint Surg 41A:749, 1959.
- Patterson MJ, Cole JD: Two-staged delayed open reduction and internal fi xation of severe pilon fractures, J Orthop Trauma 13:85, 1999.
- Peter RE, Harrington RM, Henley MB, et al: Biomechanical effects of internal fi xation of the distal tibiofi bular syndesmotic joint: comparison of two fi xation techniques, J Orthop Trauma 8:215, 1994.
- Petrisor BA, Poolman R, Koval K, et al: Management of displaced ankle fractures, J Orthop Trauma 20:515, 2006.
- Pettrone FA, Gail M, Pee D, et al: Quantitative criteria for prediction of the results after displaced fracture of the ankle, J Bone Joint Surg 65A:66, 1983.
- Phillips WA, Schwartz HS, Keller CS, et al: A prospective, randomized study of the management of severe ankle fractures, J Bone Joint Surg 67A:67, 1985.
- Phillips WA, Spiegel PG: Evaluation of ankle fractures: nonoperative vs operative, Clin Orthop Relat Res 138:17, 1979 (editorial). Pierce RO Jr, Heinrich JH: Comminuted intraarticular fractures of the distal tibia, J Trauma 19:828, 1979.
- Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures, J Bone Joint Surg 85A:1893, 2003.
- Pugh KJ, Wolinsky PR, McAndrew MP, et al: Tibial pilon fractures: a comparison of treatment methods, J Trauma 47:937, 1999.
- Ramsey PL, Hamilton W: Changes in tibiotalar area of contact caused by lateral talar shift, J Bone Joint Surg 58A:356, 1976.
- Roberts RS: Surgical treatment of displaced ankle fractures, Clin Orthop Relat Res 172:164, 1983.
- Rokkanen PU, Böstman O, Hirvensalo E, et al: Bioabsorbable fi xation in orthopaedic surgery and traumatology, Biomaterials 21:2607, 2000.
- Rüedi T: Fractures of the lower end of the tibia into the ankle joint: results 9 years after open reduction and internal fi xation, Injury 5:130, 1973.
- Rüedi T, Allgöwer M: Fractures of the lower end of the tibia into the ankle joint, Injury 1:92, 1969.
- Rüedi T, Allgöwer M: Fractures of the lower end of the tibia into the ankle joint: results 9 years after open reduction and internal fi xation, Injury 5:130, 1973.
- Rüedi TP, Allgöwer M: The operative treatment of intraarticular fractures of the lower end of the tibia, Clin Orthop Relat Res 138:105, 1979.
- Salter RB: Injuries of the ankle in children, Orthop Clin North Am 5:147, 1974.
- Salter RB, Simmonds DF, Malcolm BW, et al: The biological effect of continuous passive motion on the healing of full-thickness defects in articular cartilage: an experimental investigation in the rabbit, J Bone Joint Surg 62A:1232, 1980.
- Sarkisian JS, Cody SW: Closed treatment of ankle fractures: a new criterion for evaluation: a review of 250 cases, J Trauma 16:323, 1976.
- Segal D: Ankle fractures: internal fi xation, II: displaced ankle fractures treated surgically and postoperative management, Instr Course Lect 28:79, 1979.
- Shelbourne KD, Fisher DA, Rettig AC, et al: Stress fractures of the medial malleolus, Am J Sports Med 16:60, 1988.
- Sirkin M, Sanders R: The treatment of pilon fractures, Orthop Clin North Am 32:91, 2001.
- Sirkin M, Sanders R, DiPasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures, J Orthop Trauma 13:78, 1999.
- Stiehl JB: Ankle fractures with diastasis, Instr Course Lect 39:95, 1990.
- Stiehl JB: Complex ankle fracture dislocations with syndesmotic diastasis, Orthop Rev 19:499, 1990.
- Stiehl JB: Open fractures of the ankle joint, Instr Course Lect 39:113, 1990.
- Svend-Hansen H, Bremerskov V, Baekgaard N: Ankle fractures treated by fi xation of the medial malleolus alone: late results in 29 patients, Acta Orthop Scand 49:211, 1978.
- Teeny SM, Wiss DA: Open reduction and internal fi xation of tibial plafond fractures, Clin Orthop Relat Res 292:108, 1993.
- Thompson MC, Gesink D, Hamson K: Biomechanical evaluation of syndesmosis fi xation with 3.5and 4.5-millimeter stainless steel screws. Paper presented at the annual meeting of the Orthopaedic Trauma Association, Charlotte, NC, Oct 23, 1999.
- Tile ON: Fractures of the ankle. In Schatzker J, Tile ON, eds: The rationale of operative fracture care, New York, 1987, Springer-Verlag. Topliss CJ, Jackson M, Atkins RM: Anatomy of pilon fractures of the distal tibia, J Bone Joint Surg 87B:692, 2005.
- Torg JS, Ruggiero RA: Comminuted epiphyseal fracture of the distal tibia: a case report and review of the literature, Clin Orthop Relat Res 110:215, 1975.
- Tornetta P, Gorup J: Axial computed tomography of pilon fractures, Clin Orthop Relat Res 232:273, 1996.
- Tornetta P, Nguyen S, Scott C: Lag screw fi xation of the lateral malleolus. Paper presented at the annual meeting of the Orthopaedic Trauma Association, Vancouver, British Columbia, Oct 8, 1998.
- Tornetta P, Reynolds F, Spoo J, et al: Overtightening of the syndesmosis: is it really possible? Paper presented at the annual meeting of the Orthopaedic Trauma Association, Charlotte, NC, Oct 23, 1999.
- Vander Griend R, Michelson JD, Bone LB: Fractures of the ankle and the distal part of the tibia, J Bone Joint Surg 78A:1772, 1996.
- Vives MJ, Abidi NA, Ishikawa SN, et al:
You Might Also Like