Comprehensive Management of Humeral Shaft Fractures: An Evidence-Based Guide
Key Takeaway
Humeral shaft fractures account for approximately 3% of all skeletal injuries. While functional bracing remains the gold standard for isolated injuries, yielding high union rates, operative intervention is indicated for polytrauma, open fractures, or unacceptable alignment. This guide details the biomechanics, acceptable radiographic tolerances, step-by-step surgical approaches—including the anterolateral acromial approach—and evidence-based rehabilitation protocols essential for optimal patient outcomes.
INTRODUCTION AND EPIDEMIOLOGY
Fractures of the humeral shaft are frequently encountered in orthopedic trauma, accounting for approximately 3% of all skeletal fractures. They present with a bimodal distribution: high-energy trauma (such as motor vehicle collisions) predominantly affects young males, while low-energy falls are the primary mechanism in elderly females with osteoporotic bone.
The management of these fractures requires a nuanced understanding of upper extremity biomechanics, soft tissue envelopes, and patient-specific functional demands. As Sir John Charnley famously stated, the humerus is “perhaps the easiest of the major long bones to treat by conservative methods.” The extensive range of motion afforded by the shoulder and elbow joints, coupled with the upper extremity's tolerance for small amounts of shortening, allows for radiographic imperfections that cause minimal functional deficit and are exceedingly well tolerated by the patient.
However, the paradigm of treatment is not absolute. While nonoperative management remains the cornerstone for isolated injuries, modern orthopedic surgery has seen a refined indication for operative intervention to optimize alignment, facilitate early mobilization, and manage complex polytrauma.
BIOMECHANICS AND DEFORMING FORCES
Understanding the muscular anatomy of the arm is critical, as the fracture pattern and subsequent displacement are directly dictated by the muscular attachments relative to the fracture line.
- Proximal Third Fractures (Above Pectoralis Major): The proximal fragment is abducted and externally rotated by the rotator cuff, while the distal fragment is pulled medially by the pectoralis major.
- Middle Third Fractures (Between Pectoralis Major and Deltoid): The proximal fragment is pulled medially by the pectoralis major, latissimus dorsi, and teres major. The distal fragment is abducted by the deltoid and pulled proximally by the biceps and triceps, leading to shortening.
- Distal Third Fractures (Below the Deltoid): The proximal fragment is abducted by the deltoid, while the distal fragment is pulled proximally by the biceps and triceps, often resulting in varus angulation and shortening.
Acceptable Radiographic Tolerances
Because the upper extremity is not subjected to the same weight-bearing forces as the lower extremity, and due to the compensatory motion of the shoulder and elbow, the acceptable parameters for nonoperative alignment are generous:
* Varus/Valgus Angulation: Up to 30 degrees.
* Anterior/Posterior Bowing: Up to 20 degrees.
* Shortening: Up to 3 centimeters.
* Rotation: Up to 15 degrees of malrotation.
Clinical Pearl: While these tolerances are widely accepted, cosmetic deformity—particularly varus bowing in thin individuals—may be unacceptable to the patient even if functionally tolerated. Shared decision-making is paramount.
NONOPERATIVE MANAGEMENT: THE GOLD STANDARD
Historically, conservative treatment encompassed a variety of modalities including skeletal traction, abduction casting, Velpeau dressings, and hanging arm casts. Each of these historical methods carried distinct disadvantages, ranging from joint stiffness to patient noncompliance.
Today, functional bracing has essentially replaced all other conservative methods, establishing itself as the “gold standard” for nonoperative treatment. Initially popularized by Sarmiento in 1977, functional bracing relies on specific biomechanical principles rather than rigid immobilization.
Principles of Functional Bracing
- The Hydraulic Effect: The rigid brace compresses the soft tissues (biceps, triceps, brachialis) around the humerus. This creates a hydrostatic cylinder that stabilizes the fracture fragments.
- Active Muscle Contraction: Isometric contraction of the arm musculature within the brace further increases the hydrostatic pressure, promoting micro-motion at the fracture site which stimulates secondary bone healing (callus formation).
- Gravity: The dependent position of the arm utilizes gravity to restore length and correct angulation.
Step-by-Step Nonoperative Protocol
- Acute Phase (Days 0 to 10): Immediate application of a functional brace is often poorly tolerated due to acute swelling and pain. We currently utilize a coaptation splint (sugar-tong splint) or a hanging arm cast for the first 7 to 10 days. This allows the initial inflammatory phase to subside and pain to decrease.
- Conversion Phase: Once swelling has decreased, the splint is converted to a prefabricated, adjustable functional brace (Sarmiento brace).
- Mobilization: Pendulum exercises for the shoulder and active/active-assisted elbow range of motion are initiated immediately. Use of the extremity for light activities of daily living is encouraged as tolerated.
- Restrictions: Active shoulder abduction is strictly avoided in the early phases, as the deltoid contraction can displace the fracture.
- Sling Avoidance: The use of a sling is highly discouraged once the functional brace is applied. A sling negates the beneficial effect of gravity and frequently leads to varus and internal rotation deformities.
Surgical Warning: Skin maceration is a significant concern with functional bracing. Daily hygiene, the use of a cotton stockinette beneath the brace, and regular skin checks are mandatory. Furthermore, morbid obesity may increase the risk of varus deformities due to the inability of the brace to adequately compress the soft tissue envelope against the bone; however, these deformities are often masked by the adipose tissue and remain a cosmetic rather than functional issue.
Outcomes of Nonoperative Management
Union rates of 90% to 100% have been consistently reported with functional bracing. A landmark nonrandomized study by Jawa et al. compared outcomes in distal-third diaphyseal fractures treated with functional bracing versus plate-and-screw fixation.
* Operative Treatment: Resulted in more predictable alignment and faster radiographic healing but was associated with more severe complications, including iatrogenic nerve injury, loss of fixation, and deep infection.
* Functional Bracing: Associated with minor complications such as skin breakdown and malunion. Notably, two patients initially treated with bracing required conversion to plate fixation due to unacceptable alignment.
INDICATIONS FOR OPERATIVE INTERVENTION
While nonoperative management is highly successful, specific clinical scenarios necessitate surgical intervention. The primary goal of operative treatment is to reestablish length, alignment, and rotation with stable fixation that allows early motion and, ideally, early weight-bearing on the fractured extremity (crucial for polytrauma patients).
Absolute Indications:
* Open fractures (Gustilo-Anderson Grade II or III).
* Associated vascular injury requiring repair.
* Compartment syndrome.
* "Floating elbow" (ipsilateral humeral shaft and forearm fractures).
Relative Indications:
* Polytrauma (to facilitate mobilization and nursing care).
* Bilateral humeral shaft fractures.
* Pathologic fractures.
* Failure of conservative management (loss of reduction exceeding acceptable tolerances).
* Neurologic deficit occurring after closed reduction (suggesting nerve entrapment).
* Body habitus precluding effective bracing (e.g., morbid obesity).
OPERATIVE TECHNIQUES AND SURGICAL APPROACHES
Options for surgical fixation include plate osteosynthesis, intramedullary (IM) nailing, and external fixation. Plate osteosynthesis remains the gold standard for operative fixation, providing direct visualization, anatomic reduction, and absolute or relative stability depending on the fracture pattern.
1. Plate Osteosynthesis (ORIF)
Plating is typically performed using a 4.5mm broad or narrow dynamic compression plate (DCP) or locking compression plate (LCP). The choice of surgical approach depends on the location of the fracture.
The Anterolateral Acromial Approach (For Proximal and Mid-Shaft Fractures)
For fractures of the proximal humerus that extend into the diaphysis, an extended anterolateral approach is highly effective. This approach utilizes the internervous plane between the anterior and middle heads of the deltoid proximally, and splits the brachialis distally.
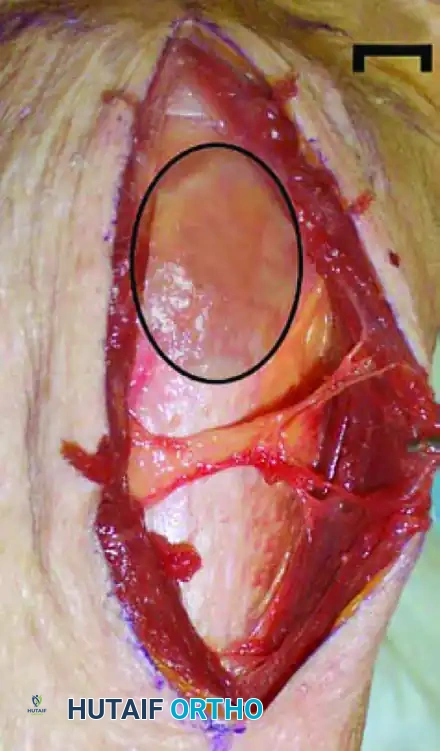
Step 1: Superficial Dissection and Deltoid Splitting
An incision is made from the anterolateral tip of the acromion extending distally. The raphe between the anterior and middle heads of the deltoid is identified. This avascular plane is carefully developed to expose the underlying proximal humerus.
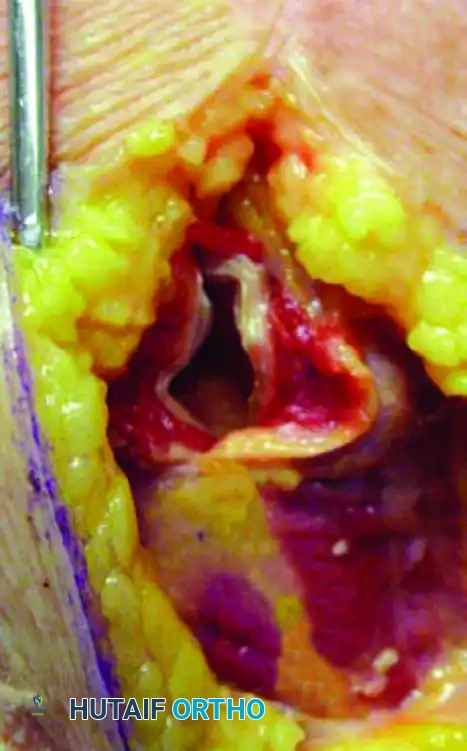
Step 2: Axillary Nerve Identification and Plate Insertion
The axillary nerve crosses the operative field approximately 5 to 7 cm distal to the lateral edge of the acromion. It must be meticulously identified and protected. When applying a locking plate for a proximal fracture with diaphyseal extension, the plate is slid deep to the axillary nerve to span the fracture site without placing tension on the neurovascular bundle.
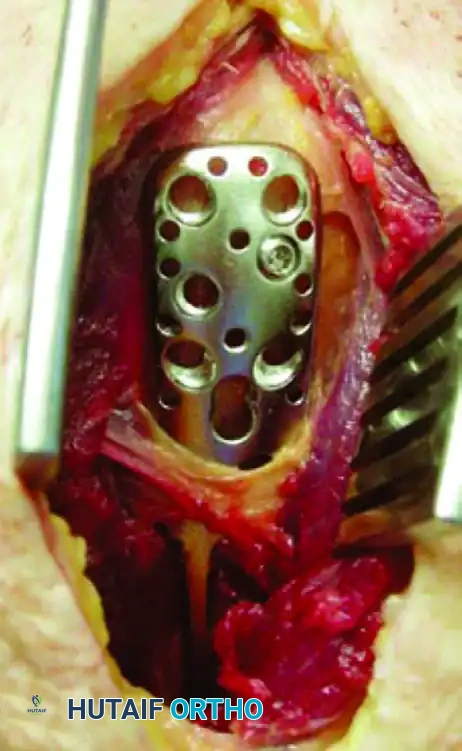
Step 3: Optimal Plate Positioning
To avoid iatrogenic injury to the ascending branch of the anterior circumflex humeral artery and the humeral head penetrating vessels, the plate must be positioned accurately. The ideal location is the "bare spot" on the lateral humerus, situated just posterior to the bicipital groove.
The Posterior Approach (For Distal-Third Fractures)
For mid-to-distal third shaft fractures, the posterior approach is preferred. It provides excellent exposure of the radial nerve and the posterior surface of the humerus, which is flat and ideal for plate application.
* The patient is positioned in the lateral decubitus or prone position.
* A midline posterior incision is made.
* The triceps can be split longitudinally (triceps-splitting) or the lateral and long heads can be separated to expose the medial head, which is then incised (triceps-sparing/Geraty approach).
* Crucial Step: The radial nerve and profunda brachii artery must be identified as they cross the posterior humerus from medial to lateral in the spiral groove. The nerve is mobilized and protected with vessel loops before plate application.
2. Intramedullary Nailing
Intramedullary (IM) nailing offers a load-sharing construct with minimal disruption of the fracture hematoma. It can be performed via an antegrade or retrograde approach.
* Advantages: Minimally invasive, preserves periosteal blood supply, excellent for pathologic fractures or segmental bone loss.
* Disadvantages: Antegrade nailing is associated with a higher incidence of shoulder pain and rotator cuff morbidity. Retrograde nailing carries a risk of iatrogenic supracondylar fracture and elbow stiffness. Furthermore, IM nailing of the humerus has historically shown higher rates of nonunion and radial nerve palsy compared to plating, though modern locked nail designs have improved outcomes.
3. External Fixation
External fixation is rarely used as a definitive treatment for humeral shaft fractures. It is generally reserved for damage-control orthopedics in polytrauma patients, high-energy gunshot wounds, fractures with massive soft tissue defects, or gross contamination.
Clinical Pearl: Suzuki et al. suggested that immediate external fixation with a planned conversion to plate fixation within 2 weeks is a safe and effective strategy for selected patients with severe soft tissue injuries that preclude early plating. However, surgeons must be vigilant: in their series, two out of 17 patients (both with open fractures) developed deep infections after conversion from external fixation to plating. Pin site care and timely conversion are critical to mitigating this risk.
COMPLICATIONS AND MANAGEMENT
Radial Nerve Palsy
The radial nerve is intimately associated with the posterior humerus, making it highly susceptible to injury. Radial nerve palsy occurs in approximately 11% to 18% of humeral shaft fractures, most commonly associated with middle-to-distal third junction fractures (Holstein-Lewis fracture).
* Primary Palsy: Present at the time of injury. The vast majority (over 85%) are neuropraxias that will spontaneously recover within 3 to 4 months. Expectant management with a wrist splint and physical therapy is indicated.
* Secondary Palsy: Occurs after closed reduction or bracing. This is a relative indication for surgical exploration, as the nerve may be entrapped in the fracture site.
* Exploration Indications: Open fractures with nerve palsy, penetrating trauma, or failure of clinical/EMG recovery by 4 to 6 months post-injury.
Nonunion
Nonunion occurs in up to 10% of humeral shaft fractures, with higher rates seen in proximal third fractures, open fractures, and patients with metabolic risk factors (smoking, diabetes).
* Atrophic Nonunion: Requires rigid internal fixation (usually a 4.5mm DCP) combined with autologous bone grafting (iliac crest) to provide osteoinductive and osteoconductive elements.
* Hypertrophic Nonunion: Primarily a mechanical failure. Rigid plate fixation alone is usually sufficient to achieve union.
Infection
Deep infection is a devastating complication, more common following operative intervention (particularly after external fixation conversion or open fractures). Management requires aggressive surgical debridement, removal of loose hardware, culture-specific intravenous antibiotics, and stabilization (often requiring revision to an external fixator or antibiotic-coated IM nail until the infection is cleared).
POSTOPERATIVE REHABILITATION PROTOCOL
Successful outcomes depend heavily on structured, phased rehabilitation.
- Phase I (0-2 Weeks): Focus on pain control, wound healing, and edema management. Immediate active and active-assisted range of motion of the fingers, wrist, and elbow. Pendulum exercises for the shoulder are initiated.
- Phase II (2-6 Weeks): Progression of shoulder range of motion. Passive and active-assisted forward elevation and external rotation. Avoid aggressive active abduction or internal rotation against resistance to protect the fixation.
- Phase III (6-12 Weeks): Once radiographic evidence of bridging callus is observed, active range of motion is advanced. Isotonic strengthening of the rotator cuff, deltoid, and periscapular stabilizers begins.
- Phase IV (12+ Weeks): Return to full functional activities and heavy lifting, contingent upon clinical and radiographic union.
CONCLUSION
Fractures of the humeral shaft present a unique biomechanical environment where nonoperative management via functional bracing remains the highly successful gold standard for isolated injuries. However, the modern orthopedic surgeon must be adept at recognizing the indications for operative intervention. When surgery is required, meticulous surgical technique—whether utilizing the anterolateral approach with careful axillary nerve protection or the posterior approach with radial nerve mobilization—is paramount to achieving anatomic restoration, minimizing complications, and ensuring a rapid return to function.
You Might Also Like

