Mastering Acute Joint Dislocations and Ligamentous Reconstruction
Key Takeaway
Acute joint dislocations require immediate, evidence-based intervention to restore biomechanical stability and prevent long-term sequelae such as post-traumatic osteoarthritis or avascular necrosis. This guide details the operative management of complex dislocations—including the patella, knee, hip, and acromioclavicular joints—while providing a step-by-step masterclass on the Liebolt technique for distal radioulnar joint (DRUJ) stabilization.
Introduction to Acute Joint Dislocations
The management of acute joint dislocations represents a critical pillar of operative orthopaedics. From the foundational principles established by Böhler and Watson-Jones to modern arthroscopic and MRI-guided interventions, the primary objective remains unchanged: achieve concentric, stable reduction while minimizing iatrogenic soft-tissue trauma. Failure to recognize subtle instability patterns or associated osteochondral shear injuries inevitably leads to chronic instability, post-traumatic arthrosis, and profound functional impairment.
This comprehensive masterclass synthesizes decades of peer-reviewed literature to provide a definitive guide on the management of complex joint dislocations. We will explore the biomechanics, surgical indications, and operative techniques for the distal radioulnar joint (DRUJ), ankle, patellofemoral joint, knee, proximal tibiofibular joint, hip, and acromioclavicular (AC) joint.
Distal Radioulnar Joint (DRUJ) Instability: The Liebolt Technique
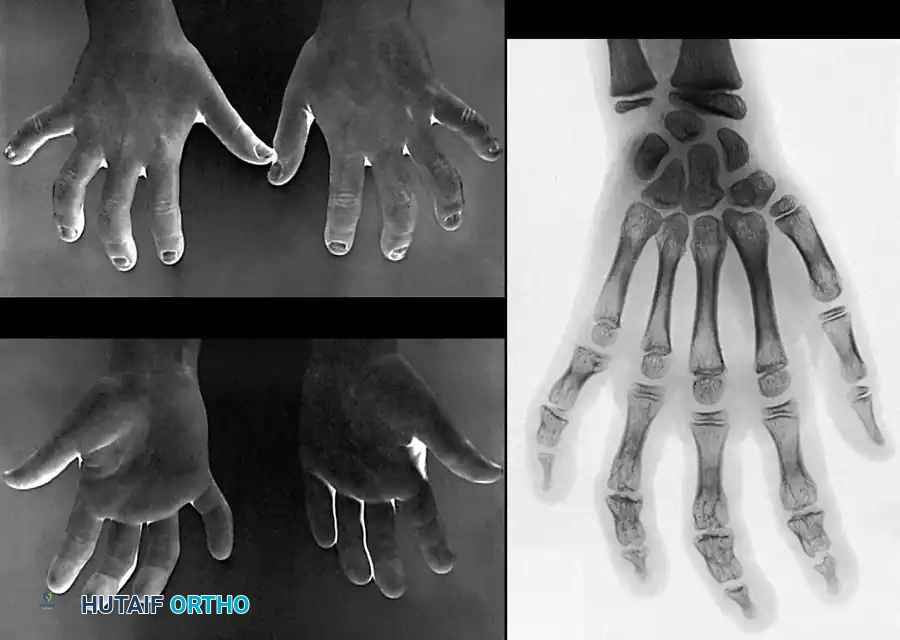
The DRUJ is a highly complex diarthrodial joint that relies heavily on the intrinsic stability provided by the triangular fibrocartilage complex (TFCC) and the extrinsic support of the extensor carpi ulnaris (ECU) subsheath. Chronic or acute-on-chronic DRUJ instability following trauma requires robust ligamentous reconstruction when direct TFCC repair is not viable.
The Liebolt technique remains a historically significant and biomechanically sound method for stabilizing the DRUJ using a tendon graft to recreate the volar and dorsal radioulnar ligaments.
Indications and Preoperative Planning
- Indications: Chronic DRUJ instability with a non-reconstructable TFCC, symptomatic volar or dorsal subluxation of the ulnar head, and failed conservative management.
- Contraindications: Advanced DRUJ arthrosis (requires salvage procedures such as the Darrach or Sauvé-Kapandji procedures), active infection, or fixed carpal malalignment.
- Graft Selection: A free palmaris longus autograft or a split strip of the ECU tendon is typically utilized.
Surgical Technique: Step-by-Step
- Positioning and Approach: The patient is placed supine with the arm on a hand table. A dorsal longitudinal incision is made over the DRUJ, centered over the fifth extensor compartment. The extensor retinaculum is incised, and the ECU is retracted to expose the distal ulna and radius.
- Preparation of the Osseous Tunnels:
Careful fluoroscopic guidance is required to avoid violating the radiocarpal joint. Drill holes are created in the distal radius and the distal ulna to anatomically mimic the origins and insertions of the radioulnar ligaments. - Graft Passage and Fixation:
The harvested tendon graft is passed through the osseous tunnels. The graft must be tensioned with the forearm in neutral rotation to prevent capturing the joint in supination or pronation.
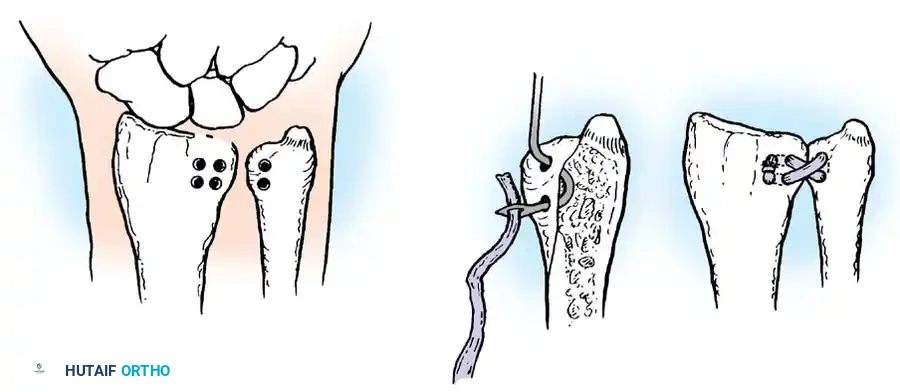
Fig. 57-24 Liebolt technique to stabilize distal radioulnar joint. A, Location of holes drilled in radius and ulna. B, Method of passing tendon. C, Appearance after joint has been stabilized.
Surgical Pearl: When drilling the ulnar tunnel (Fig. 57-24 A), ensure the entry point is at the fovea (the anatomic isometric point of the DRUJ) to allow for physiologic rotation without graft laxity or over-tensioning.
- Closure: The graft is sutured to itself or secured with interference screws (Fig. 57-24 C). The extensor retinaculum is repaired over the ECU to prevent subluxation, and the skin is closed in layers.
Postoperative Protocol
The forearm is immobilized in a long-arm cast or Munster splint in neutral rotation for 4 to 6 weeks. Following immobilization, progressive active and active-assisted range of motion (ROM) exercises are initiated. Strengthening begins at 8 to 10 weeks, with a return to heavy lifting delayed until 4 to 6 months.
Acute Patellar Dislocation
Acute lateral patellar dislocations predominantly affect young, active individuals. The primary pathoanatomic lesion is the rupture of the medial patellofemoral ligament (MPFL), which occurs in over 90% of cases (Sallay et al., 1996).
Biomechanics and Pathoanatomy
The MPFL is the primary restraint to lateral patellar translation from 0 to 30 degrees of knee flexion. Ruptures typically occur at the femoral origin (Schöttle's point) or the patellar insertion. Associated injuries frequently include osteochondral fractures of the medial patellar facet or the lateral femoral condyle, which occur as the patella relocates forcefully.
Indications for Surgery
While primary dislocations without osteochondral fragments are often managed conservatively (Larsen & Lauridsen, 1982), surgical intervention is strictly indicated for:
* Presence of an intra-articular osteochondral loose body (Nietosvaara et al., 1994).
* Massive disruption of the medial stabilizers with a grossly unstable patella in extension.
* Recurrent dislocations failing non-operative rehabilitation.
* Arthroscopic identification of a patellar "Bankart" lesion (Satterfield & Johnson, 2005).
Surgical Approach: MPFL Reconstruction
- Diagnostic Arthroscopy: Evaluate and address any chondral shear injuries. Remove loose bodies or perform internal fixation if the fragment is large and viable.
- Graft Harvest: A gracilis or semitendinosus autograft is harvested.
- Femoral Attachment: Using fluoroscopy, Schöttle's point is identified (anterior to the posterior femoral cortex line, proximal to the Blumensaat line, and distal to the medial epicondyle). A guide pin is placed, and a socket is reamed.
- Patellar Attachment: Two small transverse tunnels or suture anchors are placed in the proximal two-thirds of the medial patellar border.
- Tensioning: The graft is fixed to the patella, passed between the capsule and the vastus medialis obliquus (VMO), and docked into the femur.
Surgical Warning: Over-tensioning the MPFL graft is the most common cause of failure, leading to medial patellofemoral overload, severe pain, and rapid chondrolysis. The graft should be tensioned at 30 degrees of flexion with only enough force to restore a normal lateral glide (1-2 quadrants).
Knee and Proximal Tibiofibular Joint Dislocations
The Dislocated Knee: A Vascular Emergency
A true tibiofemoral dislocation is a devastating, high-energy multi-ligamentous knee injury (MLKI). The paramount concern is the integrity of the popliteal artery, which is tethered proximally at the adductor hiatus and distally at the soleus arch.
- Initial Management: Immediate closed reduction under conscious sedation. Post-reduction, an Ankle-Brachial Index (ABI) must be measured. An ABI < 0.9 mandates an immediate CT angiogram or formal vascular surgery consultation (Welling et al., 1981).
- Irreducible Dislocations: A posterolateral dislocation can become irreducible if the medial femoral condyle "buttonholes" through the medial capsule (Quinlan, 1966). This presents clinically with a transverse medial joint line skin furrow (the "dimple sign") and requires emergent open reduction.
- Surgical Timing: Once vascularly stable, MRI is obtained (Twaddle et al., 1996). Ligamentous reconstruction (ACL, PCL, PLC, MCL) is typically performed in a staged manner or as a single-stage procedure at 2 to 3 weeks post-injury to allow capsular healing and decrease the risk of arthrofibrosis.
Proximal Tibiofibular Joint Dislocation
Often missed in the polytrauma setting, proximal tibiofibular dislocations (Ogden, 1974) usually result from a twisting injury with the knee flexed.
* Classification: Anterolateral (most common), Posteromedial, and Superior.
* Treatment: Closed reduction is attempted by flexing the knee to 90 degrees (relaxing the biceps femoris and LCL) and applying direct pressure to the fibular head. If unstable, temporary open reduction and internal fixation (ORIF) with a single syndesmotic screw from the fibula to the tibia is performed, followed by screw removal at 8 to 12 weeks.
Traumatic Hip Dislocation
Traumatic hip dislocations are high-energy injuries, classically occurring as "dashboard injuries" in motor vehicle collisions. Posterior dislocations account for 90% of cases, while anterior dislocations occur in 10% (Epstein, 1973).
Pathomechanics and Complications
- Avascular Necrosis (AVN): The risk of AVN of the femoral head increases exponentially if the hip remains dislocated for more than 6 hours (Hougaard & Thomsen, 1986).
- Neurologic Injury: The sciatic nerve (specifically the peroneal division) is injured in 10-20% of posterior dislocations (Cornwall & Radomisli, 2000).
- Associated Fractures: Acetabular posterior wall fractures or femoral head impaction fractures (Pipkin lesions) are highly prevalent.
Reduction Maneuvers
Immediate closed reduction is mandatory.
* Allis Maneuver: The patient is supine. The surgeon applies in-line traction to the flexed knee while an assistant applies downward counter-traction on the pelvis.
* Captain Morgan Technique: The surgeon places their knee under the patient's flexed knee to act as a fulcrum, applying an upward traction force.
Pitfall: Repeated, forceful attempts at closed reduction in an inadequately sedated patient can cause iatrogenic femoral neck fractures. If two attempts fail, emergent open reduction in the operating room is required.
Post-Reduction Protocol
Following successful reduction, an immediate post-reduction CT scan is mandatory to evaluate for concentric reduction, incarcerated intra-articular osteochondral fragments, and occult acetabular or femoral head fractures (Hougaard et al., 1987). Non-concentric reduction or retained fragments dictate urgent arthroscopic or open surgical debridement.
Acromioclavicular (AC) Joint Dislocations
AC joint injuries are common athletic injuries resulting from a direct blow to the point of the shoulder, driving the acromion inferiorly while the clavicle remains stabilized by the sternocleidomastoid.
Classification and Decision Making
The Rockwood classification (expanded from Bannister et al., 1992) dictates management:
* Types I & II: Sprains or partial tears of the AC/CC ligaments. Treated non-operatively with a sling and early ROM.
* Type III: Complete rupture of AC and CC ligaments with 100% superior displacement of the clavicle. Management is highly controversial. Current evidence suggests non-operative treatment for most patients, reserving surgery for elite overhead athletes or manual laborers (Bradley & Elkousy, 2003).
* Types IV, V, & VI: Severe displacements (posterior, >100% superior, or inferior, respectively). These require operative intervention due to severe biomechanical dysfunction and skin tenting.
Surgical Reconstruction
Acute operative management (within 3 weeks) allows for primary repair and augmentation.
* Technique: The classic Weaver-Dunn procedure (transfer of the coracoacromial ligament to the distal clavicle) has largely been superseded by anatomic coracoclavicular (CC) ligament reconstruction.
* Modern Approach: Utilizing heavy non-absorbable sutures or suspensory cortical button devices, the clavicle is reduced to the coracoid. A free tendon graft (semitendinosus) is often passed under the coracoid and through osseous tunnels in the clavicle in a figure-of-eight fashion to anatomically recreate the conoid and trapezoid ligaments (Copeland & Kessel, 1980; Dumontier et al., 1995).
Postoperative Care
The shoulder is immobilized in a sling for 6 weeks. Passive ROM is permitted up to 90 degrees of forward elevation. Active ROM and strengthening are delayed until 6 to 8 weeks to allow for biologic healing of the reconstructed ligaments.
Conclusion
The operative management of acute joint dislocations demands a profound understanding of joint kinematics, ligamentous anatomy, and evidence-based surgical indications. Whether executing a precise Liebolt reconstruction for the DRUJ, navigating the vascular perils of a dislocated knee, or performing an anatomic MPFL reconstruction, the orthopaedic surgeon must prioritize concentric reduction and stable fixation. Adherence to these rigorous, textbook-level principles ensures the mitigation of catastrophic complications and the restoration of optimal patient function.
You Might Also Like