Operative Management of Morel-Lavallée Lesions and Severe Soft Tissue Trauma
Key Takeaway
The percutaneous drainage of a Morel-Lavallée lesion is a minimally invasive technique designed to evacuate hemolymphatic fluid and debride necrotic fat following closed degloving injuries. Utilizing strategic 2-cm incisions, mechanical brushing, and low-pressure lavage, surgeons can effectively obliterate the dead space. This approach, combined with prolonged closed suction drainage and targeted antibiotic therapy, significantly reduces infection rates and promotes optimal soft-tissue adherence in severe orthopaedic trauma.
INTRODUCTION TO SEVERE SOFT TISSUE TRAUMA
The management of severe soft tissue trauma remains one of the most challenging aspects of orthopaedic surgery. Whether presenting as a closed degloving injury—classically described as a Morel-Lavallée lesion—or as a high-energy open fracture, the fundamental principles of management remain consistent: meticulous debridement of necrotic tissue, reduction of bacterial bioburden through copious irrigation, obliteration of dead space, and strategic wound closure.
This comprehensive guide details the evidence-based surgical techniques for the percutaneous drainage of Morel-Lavallée lesions, as pioneered by Tseng and Tornetta, and expands upon the critical principles of open fracture debridement, irrigation fluid dynamics, and advanced wound management strategies.
PART I: PERCUTANEOUS DRAINAGE OF A MOREL-LAVALLÉE LESION
Pathoanatomy and Biomechanics
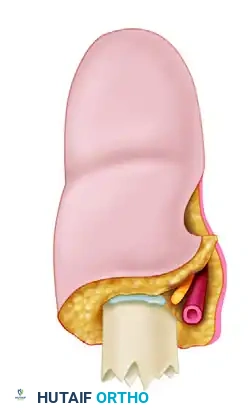
A Morel-Lavallée lesion (MLL) is a post-traumatic, closed degloving injury resulting from severe shearing forces. These forces cause the skin and subcutaneous adipose tissue to abruptly separate from the underlying rigid fascial plane. This traumatic separation disrupts the trans-fascial perforating blood vessels and lymphatic channels, leading to the rapid accumulation of a hemolymphatic fluid collection within the newly created potential space.
Over time, the peripheral margins of this collection undergo an inflammatory cascade, forming a pseudocapsule. If left untreated, the avascular subcutaneous fat undergoes liquefactive necrosis, serving as a rich nidus for bacterial colonization and predisposing the overlying skin to full-thickness necrosis due to compromised microcirculation.
Clinical Pearl: The presence of a fluctuant, compressible mass with overlying skin hypermobility following high-energy blunt trauma (especially over the greater trochanter, flank, or lumbosacral region) is highly suspicious for a Morel-Lavallée lesion. Early intervention is critical to prevent pseudocapsule formation and secondary infection.
Preoperative Planning and Positioning
Optimal patient positioning is dictated by the anatomic location of the lesion, which most commonly involves the lateral thigh and trochanteric region.
* Positioning: Place the patient in a lateral decubitus or supine position with a bump under the ipsilateral hip to allow unhindered, 360-degree access to the involved area.
* Preparation: The entire limb and hemipelvis should be prepped and draped widely to allow for the extension of incisions if the percutaneous approach must be converted to an open debridement.
Surgical Technique: The Tseng and Tornetta Approach
The percutaneous approach described by Tseng and Tornetta offers a minimally invasive method to evacuate the hematoma, debride necrotic fat, and obliterate the dead space without subjecting the compromised overlying skin to large, ischemic surgical incisions.
Step 1: Strategic Incision Placement
* Make a 2-cm longitudinal incision over the most distal, dependent aspect of the fluctuant lesion.
* Make a second 2-cm incision at the superior and posterior extent of the injury. This establishes a dual-portal system for inflow and outflow during lavage.
* Note: Additional 2-cm incisions may be required depending on the geometric complexity and overall surface area of the lesion.
Step 2: Lesion Mapping and Fluid Sampling
* Introduce a rigid suction tip (e.g., Yankauer) through the distal incision. Gently sweep the instrument subcutaneously to determine the true anatomic extent of the cavity and to break up early loculations.
* Aspirate the hemolymphatic fluid and immediately send samples for aerobic, anaerobic, and mycobacterial culture and sensitivity.
Step 3: Mechanical Debridement of Necrotic Fat
* Evacuate the primary hematoma using high-wall suction.
* Introduce a sterile plastic intramedullary brush (commonly utilized for femoral canal preparation in total joint arthroplasty) through the incisions.
* Vigorously but carefully scrub the undersurface of the subcutaneous tissue and the superficial surface of the fascia. This mechanical brushing is critical for dislodging adherent, necrotic fat lobules and disrupting the early pseudocapsule.
Surgical Warning: Do not use aggressive sharp curettage on the undersurface of the skin flap, as this may further damage the already tenuous subdermal vascular plexus, leading to iatrogenic full-thickness skin necrosis.
Step 4: High-Volume Lavage
* Perform a pulsed lavage through the superior incision while allowing outflow through the dependent distal incision.
* Continue the lavage until the effluent fluid is entirely clear and devoid of any yellow fat globules or dark hematoma debris.
Step 5: Drain Placement and Closure
* Pass a medium-sized closed suction drain (e.g., 10-French or 15-French Blake or Jackson-Pratt) through the cavity, ensuring the fenestrated portion traverses the entire length of the dead space.
* Close the 2-cm incisions tightly using deep dermal interrupted sutures and non-absorbable monofilament for the skin to prevent air leaks, which would compromise the suction seal.
Postoperative Protocol
- Suction Dynamics: Attach the drain to continuous wall suction. High negative pressure is required to physically appose the subcutaneous tissue to the fascia, promoting adherence and obliterating the dead space.
- Drain Removal Criteria: The drain must remain in place until the output is strictly less than 30 mL in a 24-hour period. Premature removal is the leading cause of MLL recurrence. This process frequently requires 8 to 14 days.
- Antibiotic Prophylaxis: Maintain the patient on intravenous cephalosporins (or culture-specific antibiotics) for 24 hours following the removal of the drain to mitigate the risk of ascending infection.
PART II: PRINCIPLES OF OPEN FRACTURE DEBRIDEMENT AND IRRIGATION
While Morel-Lavallée lesions represent severe closed soft-tissue trauma, open fractures present an immediate threat of deep infection and osteomyelitis due to direct environmental contamination. The transition from closed degloving management to open fracture care relies on the same foundational principle: aggressive, meticulous debridement.
The Timing of Debridement: Deconstructing the "6-Hour Rule"
Historically, the empirical standard for open fracture management was the "6-hour rule," which mandated operative debridement within six hours of injury to prevent bacterial logarithmic growth. However, modern extensive clinical studies have heavily scrutinized this dogma.
Current evidence-based consensus indicates that while thorough operative debridement should be performed as soon as safely possible, delaying surgery up to 24 hours in stable patients receiving immediate broad-spectrum intravenous antibiotics does not significantly increase infection rates. The standard of care remains urgent, meticulous debridement, prioritizing the quality of the surgical excision over an arbitrary time threshold.
Assessment of Tissue Viability
The cornerstone of open fracture management is the radical excision of all devitalized tissue. Muscle viability must be assessed using the classic "4 C's":
1. Color: Healthy muscle should be a vibrant, normal red. Dark brown, grey, or purple muscle indicates ischemia and necrosis.
2. Consistency: Viable muscle is firm and resilient. Friable or mushy muscle must be excised.
3. Contractility: Healthy muscle fibers will visibly contract when stimulated by electrocautery or mechanical pinching with forceps.
4. Capacity to Bleed: Good microcirculation should be visible within the bleeding edges of the cut muscle.
Irrigation Dynamics: Volume, Pressure, and Pulsation
Following the excision of dead and contaminated tissue, copious irrigation is required to mechanically wash away residual planktonic bacteria and microscopic debris.
1. Irrigation Volume
Animal models and clinical studies demonstrate a dose-dependent relationship between irrigation volume and bacterial clearance, though this effect plateaus. The widely accepted volumetric guidelines based on the Gustilo-Anderson classification are:
* Grade I Fractures: Minimum of 3 Liters.
* Grade II Fractures: Minimum of 6 Liters.
* Grade III Fractures: Minimum of 9 Liters.
2. Irrigation Pressure
The debate between high-pressure and low-pressure lavage has been largely settled by recent in vitro and in vivo studies (e.g., Draeger and Dhaners).
* High-Pressure Lavage: While effective at removing surface bacteria, high-pressure pulsatile lavage causes significant microstructural damage to soft tissues and bone architecture. Furthermore, it has been shown to drive particulate contaminants and bacteria deeper into the intramedullary canal and surrounding fascial planes (up to 4 cm away from the wound). It also impairs early osteogenesis and delays fracture healing.
* Low-Pressure Lavage: The current orthopaedic consensus strongly favors high-volume, low-pressure lavage (e.g., gravity flow or bulb-syringe). This method effectively clears debris without causing iatrogenic tissue trauma or propagating contamination.
The Role of Irrigation Additives
The use of additives in irrigation fluid remains highly controversial. Additives are generally categorized into three classes: antiseptics, antibiotics, and surfactants.
- Antiseptics (Povidone-iodine, Chlorhexidine, Hydrogen Peroxide): While possessing broad-spectrum bactericidal properties, these agents are highly cytotoxic to host osteoblasts, fibroblasts, and macrophages. They impair local immune function and delay wound healing. Their routine use in open fracture irrigation is generally discouraged.
- Antibiotics (Bacitracin, Polymyxin, Neomycin): The addition of topical antibiotics to irrigation fluid has not demonstrated clinical efficacy in preventing deep infections. Furthermore, it carries risks of systemic toxicity, allergic reactions, and the promotion of antimicrobial resistance.
- Surfactants (Castile Soap, Benzalkonium Chloride): Surfactants act by lowering the surface tension of the fluid, emulsifying lipid-based debris, and interfering with bacterial adhesion to bone and hardware. In a landmark prospective, randomized controlled trial by Anglen, nonsterile castile soap was compared to bacitracin solution in 398 lower extremity open fractures. The study found no significant difference in infection rates or bone healing, but wound healing complications were significantly higher in the bacitracin group. Consequently, low-pressure lavage with a surfactant is considered a highly effective, low-toxicity option for heavily contaminated wounds.
Pitfall: Relying on irrigation to compensate for inadequate surgical debridement is a critical error. No volume or type of irrigant can sterilize necrotic tissue. The scalpel remains the surgeon's most effective tool against infection.
PART III: WOUND MANAGEMENT AND CLOSURE STRATEGIES
Principles of Wound Closure
The historical paradigm of universally leaving open fracture wounds open has evolved. With the advent of modern aggressive debridement protocols and potent systemic antibiotics, early loose closure is now advocated for select wounds.
Criteria for Closure:
* The wound must be surgically clean following debridement.
* Closure must be absolutely tension-free. A reliable clinical test is that the wound edges should be easily approximated using a 2-0 nylon suture without the suture breaking or blanching the skin edges.
* If tension exists, the wound must be left open to prevent secondary skin necrosis, ischemia, and compartment syndrome.
Local Antibiotic Delivery: The Bead Pouch Technique
For wounds that cannot be closed primarily, or in cases of severe contamination (Gustilo IIIB/IIIC), local antibiotic delivery is highly efficacious. Polymethyl methacrylate (PMMA) bone cement is mixed with heat-stable, powdered antibiotics (commonly Vancomycin and Tobramycin). The cement is rolled into small beads, strung on a non-absorbable surgical wire, and placed directly into the wound bed.
The wound is then covered with a semi-permeable occlusive dressing (the "bead pouch"). This technique provides massive local concentrations of antibiotics—often 100 to 1000 times the minimum inhibitory concentration (MIC)—without systemic toxicity, while simultaneously preventing tissue desiccation.
Soft Tissue Coverage and Flaps
Early soft tissue coverage (ideally within 5 to 7 days) significantly decreases the incidence of deep infection, malunion, and nonunion. The reconstructive ladder dictates the method of coverage, ranging from split-thickness skin grafting to local rotational flaps (e.g., gastrocnemius or soleus flaps) and free tissue transfer.
Clinical Pearl: In severe tibial fractures requiring flap coverage (ASIF/OTA Class C injuries), careful selection of the flap is paramount. Multicenter data indicates that utilizing a local rotational flap in the zone of injury for a Class C fracture makes the patient 4.3 times more likely to experience a wound complication requiring reoperation compared to utilizing a healthy, well-vascularized free flap from outside the zone of injury.
Negative Pressure Wound Therapy (NPWT)
Negative Pressure Wound Therapy (e.g., VAC therapy) has revolutionized the interim management of open orthopaedic wounds. Applied at the conclusion of an irrigation and debridement, NPWT utilizes subatmospheric pressure to achieve several critical physiologic benefits:
1. Macro-deformation: Draws wound edges together, reducing the overall surface area of the defect.
2. Micro-deformation: Stretches individual cells, stimulating cellular proliferation and angiogenesis.
3. Fluid Evacuation: Actively removes interstitial edema and inflammatory exudate, improving local microvascular blood flow.
4. Granulation: Rapidly promotes the formation of a robust granulation tissue bed, preparing the wound for delayed primary closure or skin grafting.
NPWT devices are typically set to -125 mmHg continuous pressure and are exchanged every 48 to 72 hours in the operating room during sequential debridements until the wound bed is optimized for definitive closure.
CONCLUSION
The successful management of severe soft tissue trauma—from the percutaneous obliteration of a Morel-Lavallée lesion to the complex reconstruction of a Gustilo IIIB open fracture—requires a profound understanding of tissue biomechanics, fluid dynamics, and host biology. By adhering to strict protocols of mechanical debridement, high-volume/low-pressure lavage, and strategic dead-space management, the orthopaedic surgeon can reliably mitigate infection, preserve limb function, and optimize patient outcomes.
📚 Medical References
- Morel-Lavallée lesion, J Trauma 42:1046, 1997.
- Heckman MM, Whitesides TE, Grewe SR, et al: Histologic determination of the ischemic threshold of muscle in the canine compartment syndrome, J Orthop Trauma 7:199, 1993.
- Herscovici D Jr, Sanders RW, Scaduto JM, et al: Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy
You Might Also Like