Mastering the Surgical Management of Lower Extremity Nonunions: Tibia and Foot
Key Takeaway
Nonunions of the tibia and metatarsals present complex reconstructive challenges requiring meticulous preoperative planning. Successful management hinges on identifying the biologic and mechanical etiology of the nonunion. Treatment strategies range from partial fibulectomy and percutaneous bone marrow aspirate injection to complex posterolateral bone grafting and rigid internal fixation. This guide details the evidence-based surgical techniques, biomechanical principles, and postoperative protocols essential for achieving reliable osseous union in the lower extremity.
PRINCIPLES OF LOWER EXTREMITY NONUNION
The development of a nonunion in the lower extremity represents a profound failure of the normal fracture healing cascade, driven by either mechanical instability, biologic compromise, or a combination of both. Successful surgical intervention requires a comprehensive understanding of the host’s physiological status, the local soft-tissue envelope, and the biomechanical forces acting across the pseudarthrosis.
Clinical Pearl: Always classify the nonunion as hypertrophic (hypervascular, mechanically unstable), oligotrophic, or atrophic (avascular, biologically compromised) before selecting a surgical strategy. Hypertrophic nonunions require stability; atrophic nonunions require both stability and biologic augmentation (e.g., bone grafting).
NONUNION OF SPECIFIC BONES: THE FOOT
Metatarsals
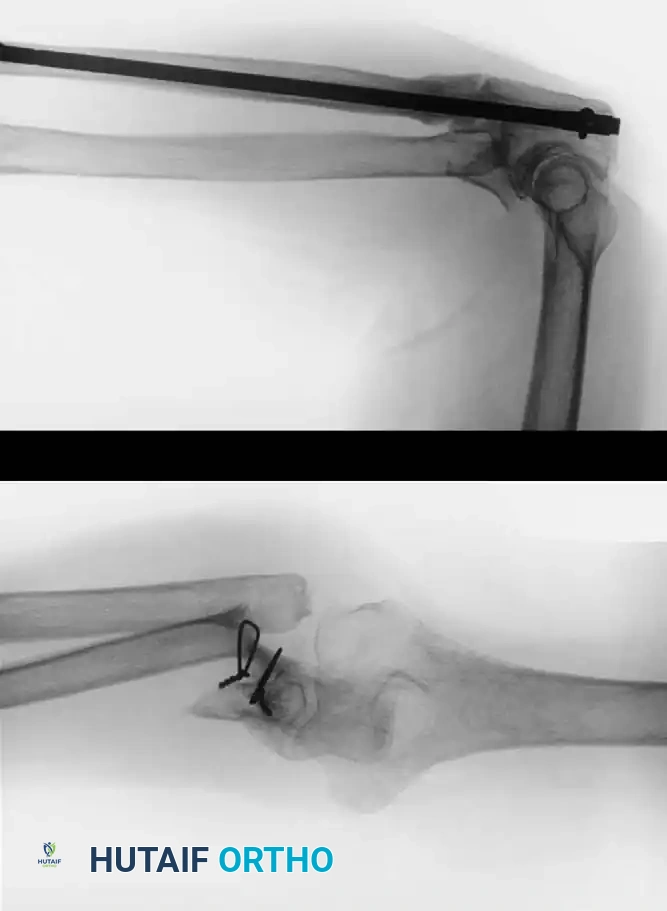
Nonunions of the metatarsals are relatively uncommon due to the robust vascular supply and the splinting effect of adjacent intact metatarsals and intrinsic musculature. When they do occur, they are almost exclusively the result of poor apposition of the fracture fragments, severe soft-tissue stripping during initial injury or surgery, or deep infection.
They occur most frequently in the distal third of the bone, particularly following highly comminuted crush injuries or displaced spiral fractures where soft tissue interposition prevents cortical contact.
Management Principles:
* Asymptomatic Nonunions: Often require no surgical intervention, provided the patient has a plantigrade, pain-free foot.
* Symptomatic Nonunions: Require surgical takedown. The fibrous pseudarthrosis must be excised back to bleeding, healthy bone.
* Fixation: Rigid internal fixation using low-profile mini-fragment plates (2.0 mm or 2.4 mm systems) is the gold standard. If a segmental defect is created after debridement, structural autograft (e.g., iliac crest) is required to maintain metatarsal length and prevent transfer metatarsalgia.
NONUNION OF THE TIBIA
Nonunions are estimated to occur after 2% to 15% of all tibial fractures, making the tibia the most common long bone to experience delayed union or nonunion. The subcutaneous nature of the anteromedial tibial face renders it highly susceptible to high-energy trauma, open fractures, and severe soft-tissue compromise.
The development of a tibial nonunion is multifactorial. It is closely related to the type and severity of the initial injury (e.g., Gustilo-Anderson classification for open fractures), but other critical factors play a significant role:
* Injury Factors: Degree of fracture comminution, high-energy mechanism, open fracture with periosteal stripping, and degree of soft-tissue injury.
* Host Factors: Medical comorbidities (diabetes mellitus, peripheral vascular disease), patient lifestyle (tobacco use is a massive risk factor, poor nutritional status), and the use of certain medications (NSAIDs, corticosteroids).
* Complications: Subsequent complications, such as deep infection or acute compartment syndrome, severely compromise the local vascularity and affect the healing of the fracture.
Medial Malleolus
A fracture of the medial malleolus occasionally fails to unite, especially after nonoperative (closed) treatment where periosteum or the deltoid ligament may interpose between the fracture fragments.
Surgery may be indicated for the few nonunions in which other serious complications of the fracture, such as advanced traumatic arthritis, are not seen on radiographs, and ideally if the injury is less than 2 years old. The standard surgical technique usually includes excision of the fibrous nonunion, application of autogenous bone grafts, and rigid internal fixation of the malleolar fragment.
When the nonunion is painful, it can be treated in one of three ways depending on the morphology of the fragment and the patient's functional demands:
- Conservative Management: When the ununited fragment is small and the patient’s lifestyle or work is sedentary, conservative treatment with an ankle corset, a scaphoid pad, a medial heel wedge, or a custom arch support may provide sufficient symptomatic relief.
- Fragment Resection: When the bone adjacent to the nonunion is highly sclerotic or has been resorbed, and the proximal part of the malleolus is large enough to preserve the ankle mortise and deltoid ligament competence, resecting the ununited distal fragment is preferable to attempting complex bone grafting.
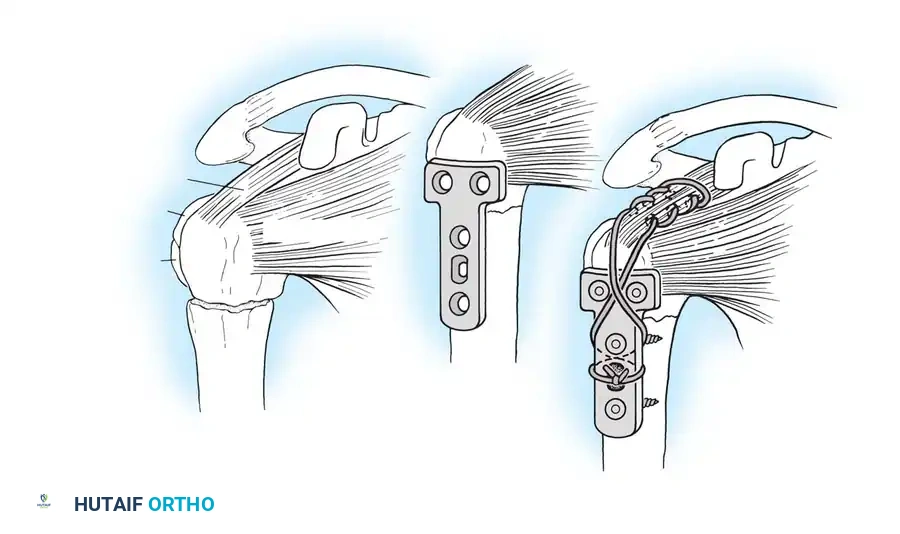
- Bone Grafting and Fixation: When neither of the two previous treatments seems applicable (e.g., large fragment, young active patient, unstable mortise), formal bone grafting and internal fixation are indicated.

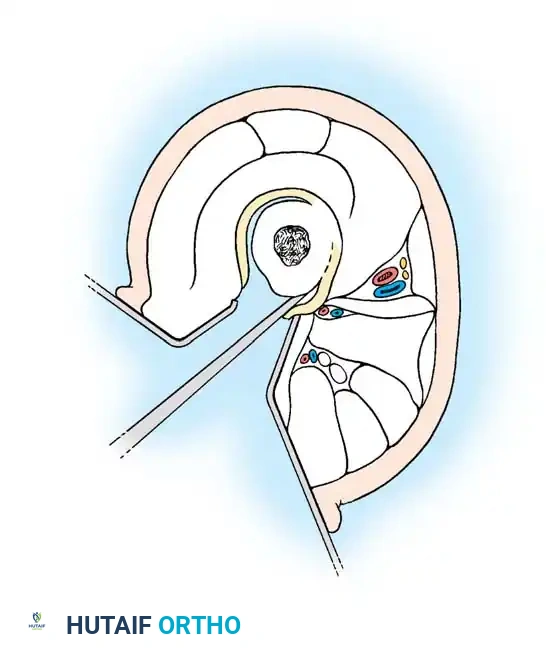
Fig. 56-16 Technique of corticotomy. A, One and one-half–cm skin incision and periosteal elevation. B, Osteotome is twisted transversely to cut groove in anterior cortex only. C, Anterior groove is cut to, but not through, medullary cavity. D, Periosteum is elevated laterally, and lateral cortex is cut with 5-mm osteotome to and through posterolateral corner. E, Anteromedial periosteum is elevated, and medial cortex is cut. F, Osteotome is twisted 90 degrees in posteromedial cortex to crack it and is inserted in posterolateral cortex and twisted. G, Osteoclasis is completed by gentle controlled external rotation of fixator rings.
Surgical Warning: When resecting a medial malleolar nonunion fragment, extreme care must be taken not to destabilize the ankle mortise. The deep fibers of the deltoid ligament must remain attached to the proximal stable segment, or valgus talar shift will inevitably occur.
Technique 56-6: Resection of the Distal Fragment of the Medial Malleolus
- Approach: Make a medial longitudinal incision 5 cm long centered over the medial malleolus. Divide the periosteum and superficial deltoid ligament fibers strictly in line with the skin incision.
- Dissection: By careful sharp and blunt subperiosteal dissection, isolate the ununited distal fragment.
- Resection: Remove the distal fragment of the malleolus. Crucial: Do not cut the periosteum in a transverse direction, and meticulously protect the posterior tibial tendon lying in the retromalleolar groove.
- Closure: Thoroughly irrigate the joint space to remove any loose bodies or debris, and close the wound in layers.
Postoperative Protocol: Weight-bearing in a rigid ankle corset or controlled ankle motion (CAM) boot can be started at 3 weeks, progressing to regular footwear as tolerated.

Technique 56-7: Sliding Graft for Medial Malleolus
- Exposure: Expose the nonunion through an anteromedial curved incision 10 cm long.
- Preparation: Reflect the periosteum anteriorly and posteriorly. Meticulously remove all interposed fibrous tissue from the nonunion site. Freshen the ends of the fragments using a curette or high-speed burr, but remove no bone from their deeper (articular) edges to avoid joint penetration. Carefully hollow out the distal fragment to receive the graft.
- Graft Harvest: Beginning at the nonunion and using an oscillating motor saw, harvest a cortical graft approximately 4 cm long and 1 cm wide from the proximal tibial fragment.
- Graft Placement: Displace (slide) the graft distally across the nonunion site and into the prepared trough in the distal fragment.
- Fixation: Hold the distal fragment in its precise anatomic position, restoring the mortise. Transfix the fragments and the sliding graft with a fully threaded or partially threaded 4.0 mm cancellous lag screw.
- Augmentation: Place cancellous bone chips (harvested from the proximal metaphysis) around the graft site to enhance osteoconduction.
- Closure: Confirm the position of the graft, the screw, and the joint space with intraoperative fluoroscopy. Close the wound in layers.

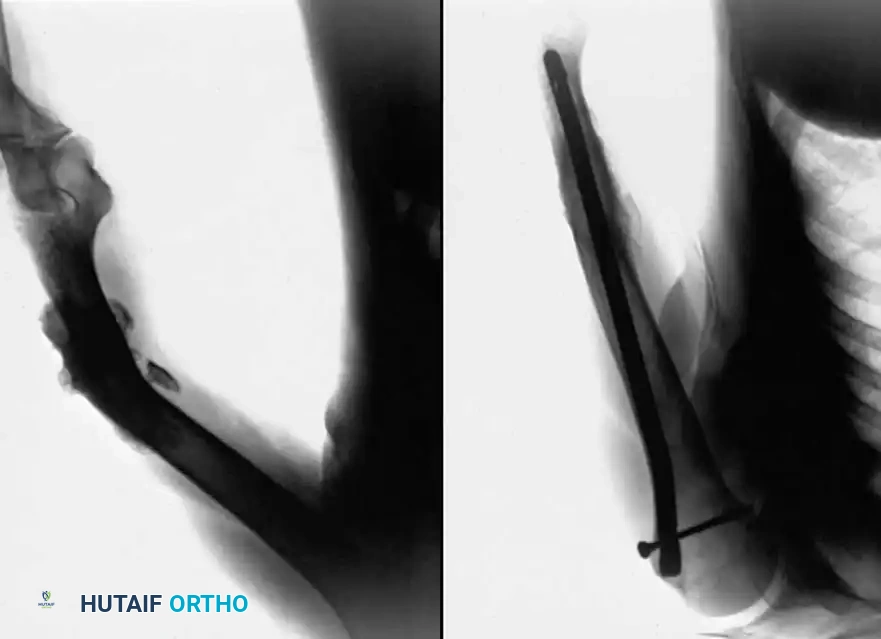
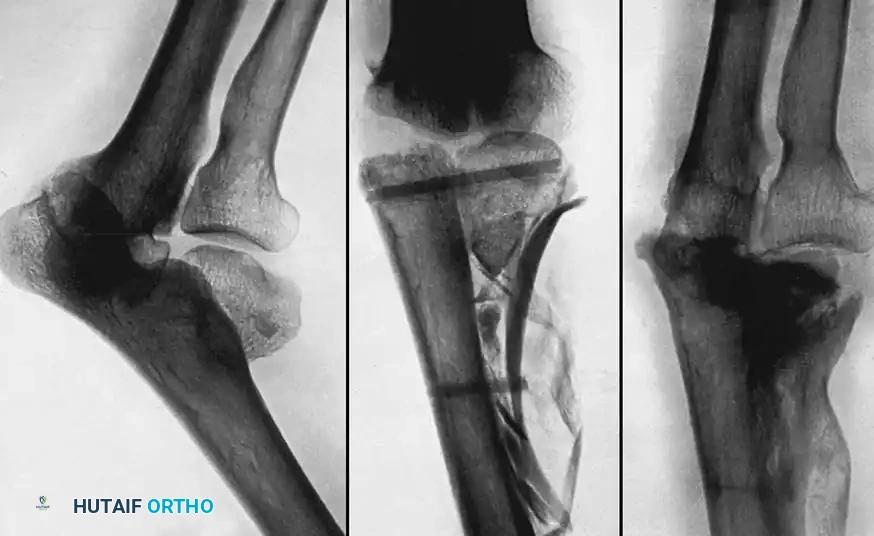
Fig. 56-18 Nonunion of medial malleolus treated by sliding graft.
Postoperative Protocol: A non-weight-bearing cast is applied from the toes to just distal to the knee. At 2 weeks, sutures are removed, and a walking cast or rigid boot is applied. Partial weight-bearing is allowed during the next 2 weeks, advancing to full weight-bearing thereafter. The immobilization is discarded when radiographs confirm osseous union, typically at 8 to 10 weeks.
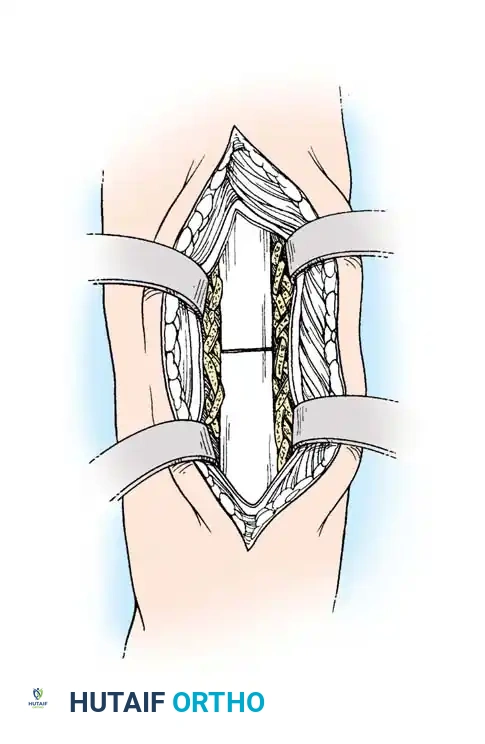
Technique 56-8: Bone Graft of Tibial Nonunion (Banks Technique)
- Exposure: Expose the nonunion through a medial longitudinal incision 10 cm long.
- Preparation: Freshen the fracture surfaces by removing sclerotic bone to create a wedge-shaped defect with its apex directed toward the articular surface of the ankle. Ensure damage to the articular cartilage is minimal.
- Reduction and Fixation: Restore the fragments to their normal anatomic position. Hold them gently with a large pointed reduction forceps (towel clip) and fix them with a 4.5 mm cortical or 4.0 mm cancellous lag screw.
- Window Creation: Make a cortical window in the tibial metaphysis at the proximal end of the surgical wound by removing a square piece of bone with its edges undercut.
- Grafting: Harvest cancellous bone through this window using a curette. Pack this autologous cancellous bone tightly into the wedge-shaped defect at the nonunion site.
- Closure: Replace the square piece of cortex over the metaphyseal window and close the wound in layers.
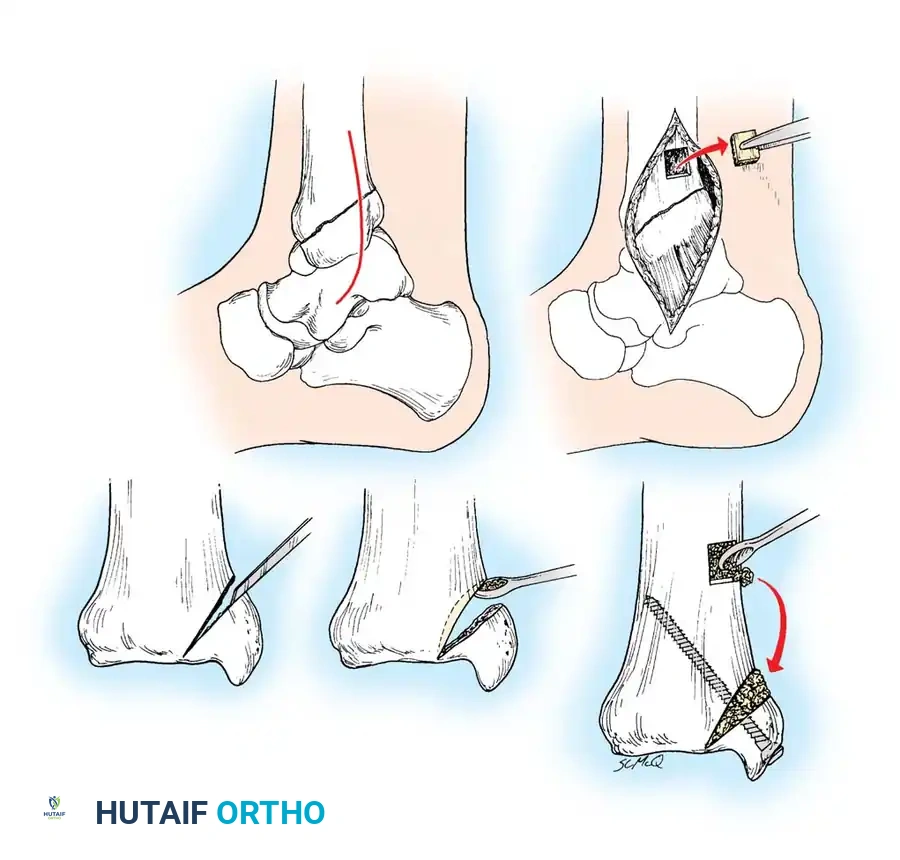
Fig. 56-19 Technique for grafting nonunion of medial malleolus (Banks).
Postoperative Protocol: The aftertreatment is identical to that of the sliding graft technique.
TIBIAL SHAFT NONUNIONS
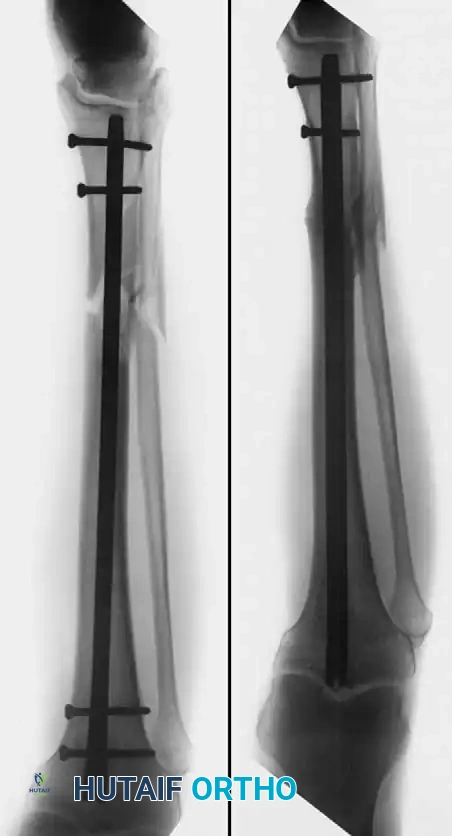
Many treatment methods have been highly successful in obtaining union of tibial shaft nonunions. Union rates of 72.1% to 87.8% have been reported with closed bone grafting procedures in hypertrophic aseptic nonunions. Internal fixation (intramedullary nailing or plating) has been reported to obtain union in up to 98% of cases, and electrical stimulation in 78.8%.
In infected nonunions, the challenge is significantly greater. Freeland and Mutz reported 100% union using closed bone grafting after infection eradication, Green and Diabal reported 81% union with open bone grafting, and Rosen reported 83% union with bone grafting combined with rigid internal fixation.
Because the tibia is a primary weight-bearing bone, its length, alignment, and rotation are critical to the biomechanical function of the knee and ankle. Simply obtaining union is insufficient; union must be achieved in an anatomic position to prevent adjacent joint arthrosis.
Hypervascular vs. Avascular Nonunions
The surgical technique selected depends heavily on whether the nonunion is hypervascular (hypertrophic) or avascular (atrophic), and whether the alignment of the fragments is satisfactory.
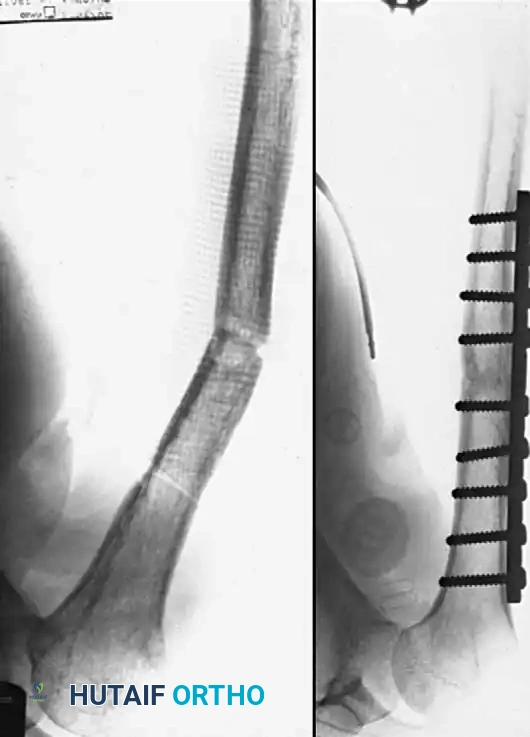
- Hypervascular Nonunions: The bone ends possess excellent biological capacity to unite but lack mechanical stability. In these cases, rigid internal fixation with a compression plate, an intramedullary nail, or a circular external fixator is usually all that is necessary. Supplemental bone grafting is rarely required.
- Avascular Nonunions: The bone ends are sclerotic, necrotic, and lack osteogenic potential. Rigid internal fixation must be supplemented by aggressive decortication of the sclerotic bone ends (shingling) and the application of autogenous bone graft. Weber and Brunner, Müller and Thomas, and Christensen have found these combined methods highly successful.
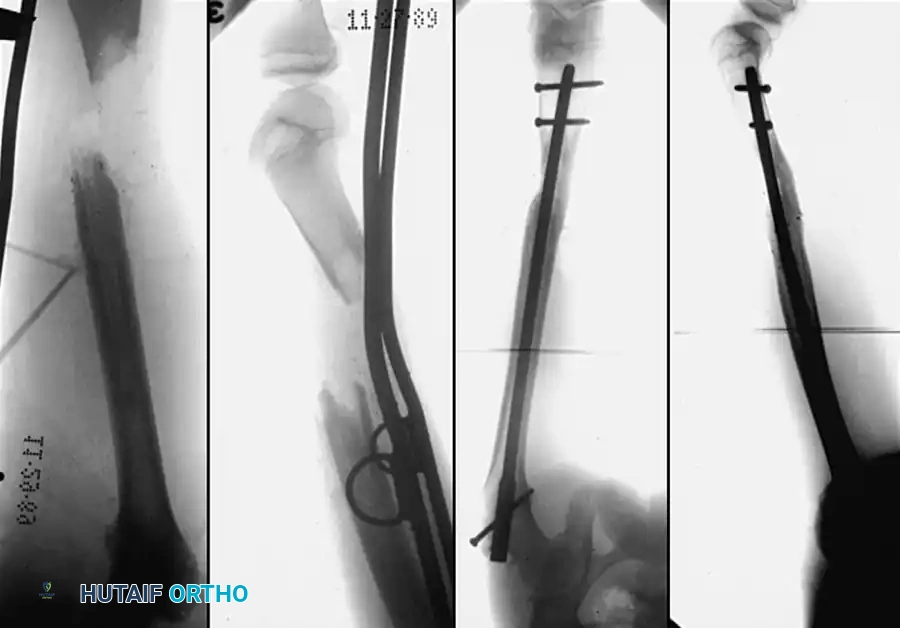
Judet and Patel reported excellent results treating 290 nonunions of the tibial shaft by internal fixation with plates and screws or intramedullary nails. The fragments were decorticated in all instances, but iliac cancellous grafts were rarely added. Clancey, Winquist, and Hansen treated 48 nonunions of the tibial shaft by Küntscher intramedullary nailing. In 30 cases, the nailing was completely closed, and in only 18 was open tibial osteotomy necessary to realign the fracture. Bone grafting was not used, and all but two nonunions healed.

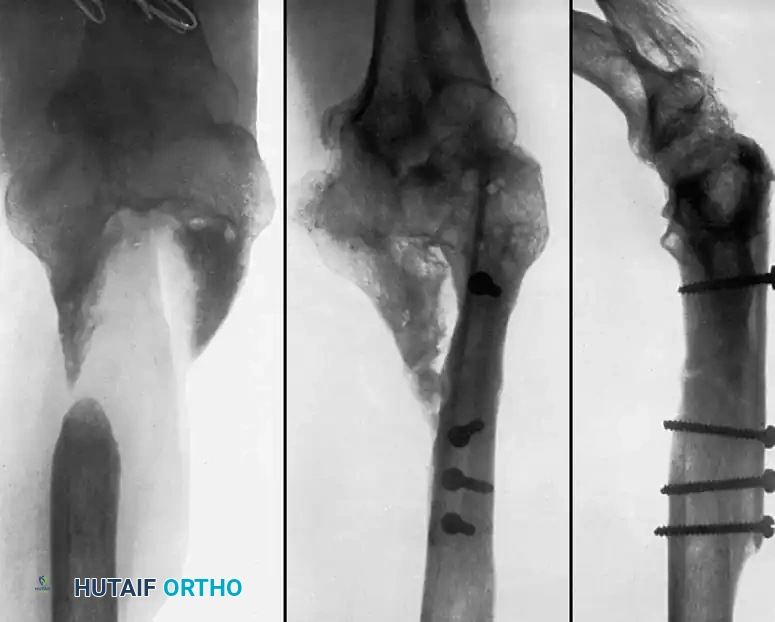
Historical Context: Onlay Bone Grafts
In the past, most nonunions of the tibial shaft were treated with a massive cortical onlay bone graft with satisfactory results. While this method is rarely used today due to the advent of locked intramedullary nailing and locking plate technology, it remains a historically significant technique that is occasionally useful for nonunions in the extreme proximal or distal fourth of the tibia, or when dealing with severely sclerotic fragments where intramedullary instrumentation is impossible.
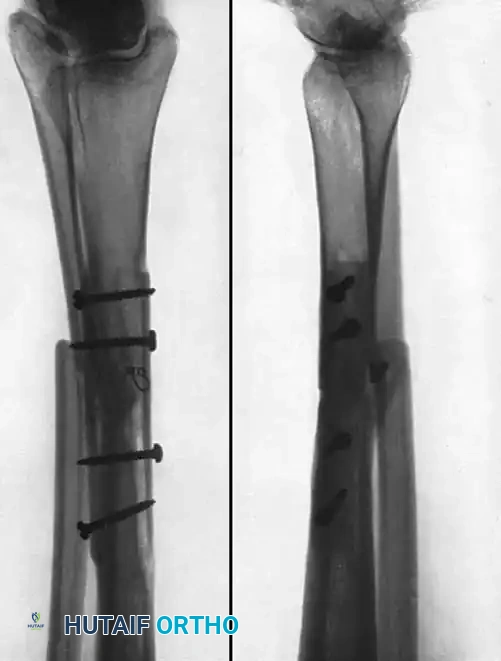
Fig. 56-20 A, Nonunion after osteotomy. Failure to produce union by sliding inlay graft; fibula is intact. B, Four years after application of dual onlay grafts and osteotomy of fibula.


Fig. 56-21 A, Oblique comminuted fracture of proximal third of tibia. B, Satisfactory restoration. C, Fracture of shaft failed to unite; treated by dual onlay graft.
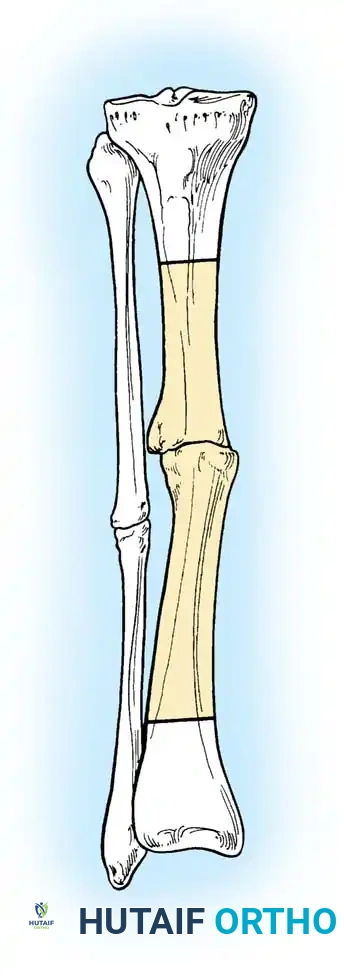
Partial Fibulectomy and Weight Bearing
When the fibula and the tibia are fractured simultaneously, the fibula almost always heals first due to its robust muscular envelope. Once healed, the intact fibula acts as a load-sharing strut that decreases axial loading across the healing tibia. Furthermore, an intact fibula may physically prevent the close apposition of tibial fragments.
Partial fibulectomy removes this strut, allowing closer apposition of the tibial fragments and restoring full axial loading to the tibia, which stimulates osteogenesis according to Wolff's Law.
Sørensen listed four distinct advantages to this technique:
1. It is technically simple and minimally invasive.
2. It allows for the closed correction of minor malpositions.
3. It avoids opening the tibial fracture site, thereby decreasing the risk of infection and preserving the precarious vascular supply to the tibial fragments.
4. It does not burn bridges; it allows for later formal bone grafting or internal fixation if union still fails to occur.
DeLee, Heckman, and Lewis reported healing in 77% of 51 tibial nonunions after partial fibulectomy. Failures were strongly associated with patient noncompliance (failure to bear weight postoperatively), the presence of a true synovial pseudarthrosis, or previous prolonged external fixation.
Surgical Principles of Fibulectomy:
The full-thickness segment removed from the fibula must be approximately 2.5 cm long. Removal of a smaller segment may allow the fibula to heal before the tibia unites, recreating the strut effect. Following resection, the tibia must be carefully aligned by closed manipulation to prevent a varus deformity. A straight long-leg walking cast is applied for 6 weeks, and aggressive full weight-bearing is encouraged.


You Might Also Like
